Evaluation of Antibacterial Efficacy of MTA with and without Additives Like Silver Zeolite and Chlorhexidine
Kiran Ghatole1, Anand Patil2, Ramesh Halebathi Giriyappa3, Thakur Veerandar Singh4, Sistla Venkata Jyotsna5, Surabhi Rairam6
1 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Sri Sai College of Dental Surgery, Vikarabad, India.
2 Professor and Head, Department of Conservative Dentistry and Endodontics, K.L.E. V.K. Institute of Dental Sciences, Belgaum, India.
3 Professor, Department of Conservative Dentistry and Endodontics, K.L.E. V.K. Institute of Dental Sciences, Belgaum, India.
4 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Sri Sai College of Dental Surgery, Vikarabad, India.
5 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Sri Sai College of Dental Surgery, Vikarabad, India.
6 Reader, Department of Conservative Dentistry and Endodontics, HKE’S S. Nijalingappa Dental College, Kalaburgi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kiran Ghatole, Sri Sai College of Dental Surgery, Kothrepally, Vikarabad, India.
E-mail: ghatolek@gmail.com
Introduction
Microorganisms, predominantly Enterococcus faecalis are found responsible in the progression of pulpal, periradicular diseases and in endodontic failures. Unsuccessful conventional treatment might necessitate the need for a surgical approach; where in retrograde restorative materials are used to seal the apex. Among the root end filling materials, Mineral Trioxide Aggregate (MTA) is considered biocompatible and is most commonly used in clinical applications but it has limited antibacterial activity. Metallic silver and chlorhexidine have been added into various dental materials to enhance the antibacterial activity.
Aim
This study aimed to compare the antibacterial effect of MTA, MTA mixed with silver zeolite and MTA mixed with chlorhexidine against Enterococcus faecalis.
Materials and Methods
Test materials used in the study were divided into three groups namely Group 1- MTA, Group 2-MTA + Silver Zeolite, Group 3-MTA + Chlorhexidine. Direct contact test was done by placing a standardized suspension of Enterococcus faecalis on the test materials in a 96 well microtiter plate. The bacterial growth was measured spectrophotometrically using ELISA reader at intervals of one, three and seven days.
Statistical Analysis
Data was collected by recording the optical density and analyzed using two-way ANOVA and Tukey’s multiple post hoc test followed by paired-t test.
Results and Conclusion
All test groups showed antibacterial activity against Enterococcus faecalis at day one, three and seven. MTA with silver zeolite showed the maximum antibacterial activity followed by MTA with 2% chlorhexidine. The least antibacterial effect was shown by MTA mixed with sterile water.
Antibacterial additives, Direct contact test, Enterococcus faecalis, Root end filling materials
Introduction
The endodontic treatment aims at cleaning, shaping followed by complete obturation of the root canal system [1]. Failure after endodontic therapy is due to persistent or secondary infection especially of Enterococcus faecalis in poorly and in well treated root canals [2]. Surgical intervention aims to remove the infected root end and ensure good root canal sealing using root end filling materials. Among the numerous root end filling materials available MTA is most frequently used and has shown long term clinical success [3]. However some studies showed MTA to have no effect or to delay the growth of Enterococcus faecalis [4–6].
Incorporation of certain additives like metallic silver and chlorhexidine has shown to enhance antibacterial properties of various dental materials [7,8]. So the purpose of the study was to assess whether incorporation of these additives enhance the antibacterial efficacy of MTA especially against E. Faecalis.
Antibacterial efficacy of root end filling materials can be evaluated using agar diffusion test, however it was found to be insensitive and unable to differentiate with bactericidal or bacteriostatic ability [9]. Therefore a more appropriate, quantitative and reproducible test such as direct contact test would be more appropriate [10].
Aim
So the present study aimed to evaluate the antibacterial effect of MTA, MTA mixed with silver zeolite and MTA mixed with chlorhexidine against Enterococcus faecalis using direct contact test.
Materials and Methods
This in-vitro study was conducted in Department of Conservative Dentistry and Endodontics in collaboration with Department of Microbiology, KLE’s VK Institute of Dental Sciences, Belgaum, Karnataka, India in the year 2013.
The study had three main groups based on the addition of antibacterial agents to MTA as follows:
Group 1: Mineral Trioxide Aggregate (ProRoot MTA, Dentsply.) was dispensed and mixed with sterile distilled water in the ratio of 1:1 as the control group.
Group 2: Powder form of silver zeolite (Sigma Aldrich Chemie GmbH, Germany, Batch #06306CJ.) was added at 2% mass fraction to Mineral Trioxide Aggregate powder and mixed with sterile distilled water.
Group 3: Mineral Trioxide Aggregate was mixed with 2% chlorhexidine (V – Consept) in 1:1 ratio.
Test Microorganism
Enterococcus faecalis (ATCC 29212) was grown on brain heart infusion agar plate and then sub-cultured on nutrient agar medium. After confirming the purity of the strain, the bacterial suspension was inoculated into 5ml of 85% saline and adjusted spectrophotometrically at 800nm to match the transmittance of 90T (equivalent to 0.5 McFarland scale =1.5x108 C.F.U) [11].
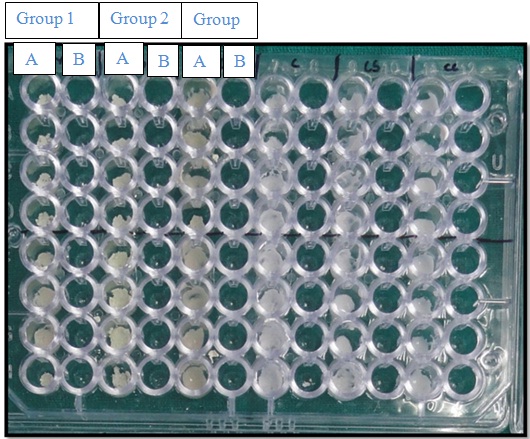
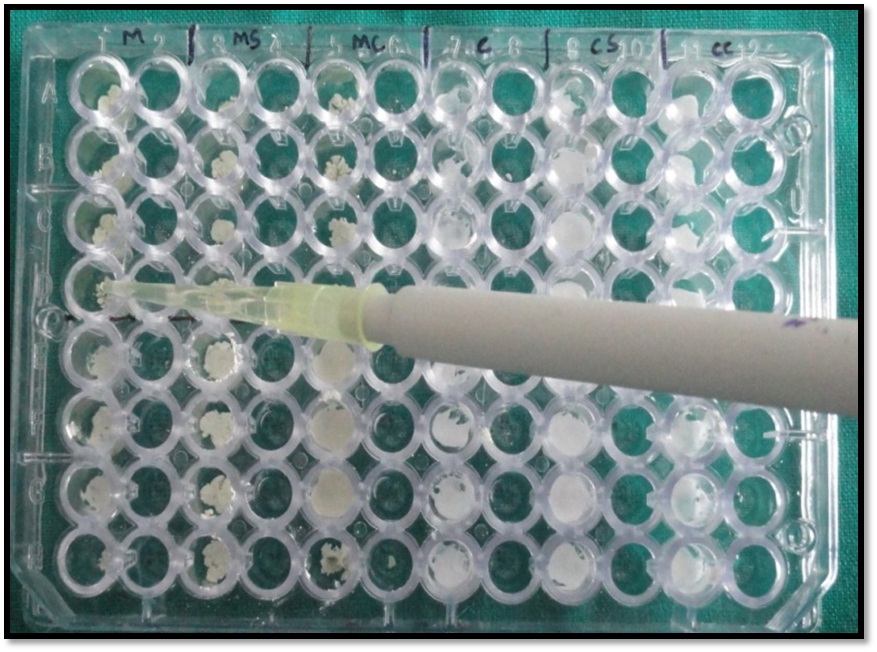
Direct contact test is based on determining the turbidity of bacterial growth in 96 well microtiter plates. In the present study all the test materials were freshly mixed and were placed at the bottom of four wells in the microtiter plate (subgroup A) to a height of 2mm which were then exposed to 10μl bacterial suspension [Table/Fig-1]. BHI broth (245μl) was added after ensuring direct contact of the bacteria to the test material [Table/Fig-2]. After mixing for 2 min, 15μl was transferred into four adjacent wells (subgroup B) containing 215μl fresh medium. The kinetics of bacterial outgrowth in each well were then followed by continuous measurements by ELISA reader measured at 630 nm [Table/Fig-3]. Densitometric readings were taken on the first, third and seventh day from each set of samples. The experiments were triplicated.
Wells coated with test materials.
Transfer of brain heart infusion broth to the microtiter wells.
Elisa Reader (Stat Fax 2100) (Awareness Technology).

Statistical Analyisis
All the data collected by recording the optical density were analyzed using two-way ANOVA and Tukey’s multiple post hoc test followed by paired-t test.
Results
According to the results of the study, two way ANOVA and Tukey’s multiple post hoc test showed that MTA mixed with silver zeolite (Group 2) had maximum antibacterial activity followed by MTA mixed with 2% chlorhexidine (Group 3). The least antibacterial activity was seen with MTA mixed with sterile distilled water(Group 1) in fresh as well as in aged samples of three and seven days. The optical densities at day one were 0.2649±0.0112, 0.14027±0.0021 and 0.1931±0.0067 for Group 1, 2, 3 respectively [Table/Fig-4, 5]. At day three, optical densities were 0.3455±0.0066,0.2367±0.0111,0.2883±0.0070 [Table/Fig-6,7] and for day seven they were 0.4598±0.0014, 0.3411±0.0039, 0.3924±0.0099 for Group 1,2 and 3 respectively [Table/Fig-8, 9]. There was significant difference (p<0.05) in the optical density among the three test materials at all time intervals.
Two way ANOVA between main groups (1,2 and 3) and sub groups (A and B) with respect to optical density at 1st day.
| SV | DF | SS | MSS | F-value | p-value |
|---|
| Main effects |
| Groups | 2 | 0.0431 | 0.0215 | 485.1430 | <0.0001 |
| Sub groups | 1 | 0.0124 | 0.0124 | 279.3269 | <0.0001 |
| 2-way interactions |
| Groups x Sub groups | 2 | 0.0020 | 0.0010 | 22.4702 | <0.0001 |
| Error | 18 | 0.0008 | 0.0000 | | |
| Total | 23 | 0.0583 | | | |
*Abbreviations: SV-Sources of variation, DF-Degrees of freedom, SS-Sum of squares, MSS-Mean sum of squares, p-Probability, SD-Standard deviation
Pair wise comparison of main groups (1, 2 and 3) and sub groups (A and B) with respect to optical density at 1st day by Tukey’s multiple post hoc procedures.
| Main groups | Group 1 | Group 2 | Group 3 |
|---|
| Sub groups | Sub group A | Sub group B | Sub group A | Sub group B | Sub group A | Sub group B |
|---|
| Mean | 0.2649 | 0.1940 | 0.1402 | 0.1112 | 0.1931 | 0.1567 |
| SD | 0.0112 | 0.0035 | 0.0021 | 0.0063 | 0.0067 | 0.0063 |
| Group 1 | Sub group 1 | - | | | | | |
| Sub group 2 | 0.0002* | - | | | | |
| Group 2 | Sub group 1 | 0.0002* | 0.0002* | - | | | |
| Sub group 2 | 0.0002* | 0.0002* | 0.0002* | - | | |
| Group 3 | Sub group 1 | 0.0002* | 0.9998 | 0.0002* | 0.0002* | - | |
| Sub group 2 | 0.0002* | 0.0002* | 0.0271* | 0.0002* | 0.0002* | - |
*p<0.05
Two way ANOVA between main groups (1,2 and 3) and sub groups (A and B) with respect to optical density at 3rd day.
| SV | DF | SS | MSS | F-value | p-value |
|---|
| Main effects |
| Groups | 2 | 0.0453 | 0.0226 | 408.4914 | <0.0001 |
| Sub groups | 1 | 0.0172 | 0.0172 | 309.4468 | <0.0001 |
| 2-way interactions |
| Groups x Sub groups | 2 | 0.0006 | 0.0003 | 5.5780 | 0.0130* |
| Error | 18 | 0.0010 | 0.0001 | | |
| Total | 23 | 0.0641 | | | |
*Abbreviations: SV-Sources of variation, DF-Degrees of freedom, SS-Sum of squares, MSS-Mean sum of squares, p-Probability, SD-Standard deviation
Pair wise comparison of main groups (1, 2 and 3) and sub groups (A and B) with respect to optical density at 3rd day by Tukey’s multiple post hoc procedures.
| Main groups | Group 1 | Group 2 | Group 3 |
|---|
| Sub groups | Sub group A | Sub group B | Sub group A | Sub group B | Sub group A | Sub group B |
|---|
| Mean | 0.3455 | 0.2954 | 0.2367 | 0.1936 | 0.2883 | 0.2211 |
| SD | 0.0066 | 0.0085 | 0.0111 | 0.0033 | 0.0070 | 0.0059 |
| Group 1 | Sub group 1 | - | | | | | |
| Sub group 2 | 0.0002* | - | | | | |
| Group 2 | Sub group 1 | 0.0002* | 0.0002* | - | | | |
| Sub group 2 | 0.0002* | 0.0002* | 0.0002* | - | | |
| Group 3 | Sub group 1 | 0.000*2 | 0.7571 | 0.0002* | 0.0002* | - | |
| Sub group 2 | 0.0002* | 0.0002* | 0.0765 | 0.0008* | 0.0002* | - |
*p<0.05
Two way ANOVA between main groups (1,2 and 3) and sub groups (A and B) with respect to optical density at 7th day.
| SV | DF | SS | MSS | F-value | p-value |
|---|
| Main effects |
| Groups | 2 | 0.0531 | 0.0266 | 245.3901 | <0.0001 |
| Sub groups | 1 | 0.0246 | 0.0246 | 226.8104 | <0.0001 |
| 2-way interactions |
| Groups x Sub groups | 2 | 0.0001 | 0.0001 | 0.5199 | 0.6033 |
| Error | 18 | 0.0019 | 0.0001 | | |
| Total | 23 | 0.0797 | | | |
*Abbreviations: SV-Sources of variation, DF-Degrees of freedom, SS-Sum of squares, MSS-Mean sum of squares, p-Probability, SD-Standard deviation
Pair wise comparison of main groups (1, 2 and 3) and sub groups (A and B) with respect to optical density at 7th day by Tukey’s multiple post hoc procedures.
| Main groups | Group 1 | Group 2 | Group 3 |
|---|
| Sub groups | Sub group A | Sub group B | Sub group A | Sub group B | Sub group A | Sub group B |
|---|
| Mean | 0.4598 | 0.3900 | 0.3411 | 0.2785 | 0.3924 | 0.3329 |
| SD | 0.0114 | 0.0096 | 0.0039 | 0.0032 | 0.0099 | 0.0175 |
| Group 1 | Sub group 1 | - | | | | | |
| Sub group 2 | 0.0002* | - | | | | |
| Group 2 | Sub group 1 | 0.0002* | 0.0002* | - | | | |
| Sub group 2 | 0.0002* | 0.0002* | 0.0002* | - | | |
| Group 3 | Sub group 1 | 0.0002* | 0.9994 | 0.0002* | 0.0002* | - | |
| Sub group 2 | 0.0002* | 0.0002* | 0.8710 | 0.0002* | 0.0002* | - |
*p<0.05
Discussion
Complete elimination of the bacteria from the pulp space plays an important role in the success of endodontic treatment. Post-endodontic failures are due to inadequate cleaning and shaping and/or insufficient obturation. Microorganisms have been isolated from 35% to 100% of failed cases, predominantly E. faecalis [11]. Hence E. faeaclis was taken as test organism in the study.
Failure after conventional endodontic treatment necessitates surgical intervention which aims to remove the infected root end and ensure good sealing by root end filling materials, among which MTA seems to be promising; however its antibacterial properties are controversial [12]. Grey MTA was found to invoke a more desirable biologic response than White MTA and hence should be used as root end filling material as esthetics is not the prime concern at these sites [13]. Hence in the study ProRoot MTA was used.
Addition of silver containing zeolite to materials like GIC and resins has improved their antimicrobial activity [7,14]. Chlorhexidine (CHX) is a known antimicrobial agent especially against E.Faecalis along with bicompatibility with periodontal tissues [15]. Luddin N, and Ahmed HM have showed CHX to be effective in reducing or completely eliminating E. faecalis [15,16]. Hence in this study silver zeolite and chlorhexidine were used as additives with MTA to increase its antibacterial property.
Antibacterial activity has been evaluated using agar diffusion test in in-vitro studies but it has shown to lack inoculum standardization, culture adequacy, sample size etc., [17]. To overcome these disadvantages, a standardized protocol suggested by Weiss et al., that is direct contact test was followed [10]. Direct contact test is a qualitative and reproducible method, which is ineffective and insensitive to the inoculums size brought in contact to the test material.
According to the results of this study, antimicrobial activity of MTA mixed with silver zeolite was maximum followed by MTA mixed with chlorhexidine. MTA mixed with sterile water showed least antimicrobial activity at all the time intervals tested. These results are similar to findings of Eldeniz and Hasan Zarrabi M et al., whose study showed that MTA was ineffective against E. faecalis [6,18]. In contrast, Al-Hezaimi K et al., stated that gray MTA was effective against E. faecalis [19]. The ineffectiveness of MTA on E. faecalis in most of studies is due to the capacity of this microorganism to survive under various stressful environmental condition [20]. This could be the reason for low antimicrobial activity of MTA against E. Faecalis.
Silver zeolite incorporation enhanced the antimicrobial property of MTA, which was also confirmed by Odabas ME et al., [21]. Silver zeolite shows antimicrobial activity because of metallic silver as its constituent, as it has highest antibacterial activity among metal ions. Zeolite is a porous crystalline material of hydrated sodium and alumino-silicate, having void spaces within frameworks of 3-10 angstroms in diameter that are capable of hosting cations such as silver or zinc [22]. Kawahara suggested silver zeolite as a useful vehicle to enhance the antibacterial activity of the dental materials [23]. Davies showed that antimicrobial activity of glass ionomer cement could be enhanced by incorporating silver zeolite with it [24].
MTA with 2% chlorhexidine showed good antibacterial activity as compared to MTA alone; however it was less effective as compared with MTA and silver zeolite. This could be attributed to the chlorhexidine crossing the microbial cell wall by passive diffusion, and disturbing the cytoplasmic membrane causing reduction in leakage, leading to lysis. Similar results were shown by Stowe who substituted chlorhexidine gluconate for water to enhance the antimicrobial activity of ProRoot MTA [25].
Limitation
To fully access the viability of silver zeolite MTA, further studies are needed to evaluate the physical properties and test antibacterial effect in clinical conditions.
Conclusion
Under the parameters of the study, it can be concluded that all the test materials exhibited antibacterial activity against E. faecalis. MTA mixed with silver zeolite showed the maximum antibacterial activity followed by MTA mixed with 2% chlorhexidine and the least shown by MTA mixed with sterile water. Silver zeolite and chlorhexidine can be incorporated into MTA to enhance its antibacterial effect against E. Faecalis.
*Abbreviations: SV-Sources of variation, DF-Degrees of freedom, SS-Sum of squares, MSS-Mean sum of squares, p-Probability, SD-Standard deviation
*p<0.05
*Abbreviations: SV-Sources of variation, DF-Degrees of freedom, SS-Sum of squares, MSS-Mean sum of squares, p-Probability, SD-Standard deviation
*p<0.05
*Abbreviations: SV-Sources of variation, DF-Degrees of freedom, SS-Sum of squares, MSS-Mean sum of squares, p-Probability, SD-Standard deviation
*p<0.05
[1]. Celikten B, F, Uzuntas C, I Orhan A, Tufenkci P, Misirli M, O Demiralp K, Micro-CT assessment of the sealing ability of three root canal filling techniquesJ Oral Sci 2015 57(4):361-66. [Google Scholar]
[2]. Binoy D, Sajjan GS, Peddireddi S, Kumar MS, Bhavana V, Raju SR, A comparitive evaluation of sealing ability, pH and rheological properties of zinc oxide eugenol sealer combined with different antibiotics: an in vitro studyJ Clin Diagn Res 2014 8(11):ZC05-08. [Google Scholar]
[3]. Parirokh M, Torabinejad M, Mineral trioxide aggregate: a comprehensive literature review-part III: clinical applications, drawbacks, and mechanism of actionJ Endod 2010 36(3):400-13. [Google Scholar]
[4]. Al-Hezaimi K, Al-Shalan TA, Naghshbandi J, Oglesby S, Simon JH, Rotstein I, Antibacterial effect of two mineral trioxide aggregate (MTA) preparations against Enterococcus Faecalis and Streptococcussanguis in vitroJ Endod 2006 32(11):1053-56. [Google Scholar]
[5]. Estrela C, Bammann LL, Estrela CR, Silva RS, Pecora JD, Antimicrobial and chemical study of MTA, portland cement, calcium hydroxide paste, sealapex and dycalBraz Dent J 2000 11(1):3-9. [Google Scholar]
[6]. Eldeniz AU, Hadimli HH, Ataoglu H, Orstavik D, Antibacterial effect of selected root end filling materialsJ Endod 2006 32(4):345-49. [Google Scholar]
[7]. Cinar C, Ulusu T, Ozcelik B, Karamuftuoglu N, Yucel H, Antibacterial effect of silver zeolite containing root canal filling materialJ Biomed Mater Res B Appl Biomater 2009 90(2):592-95. [Google Scholar]
[8]. Holt DM, Watts JD, Besson TJ, Kirkpatrick TC, Rutledge RE, The antimicrobial effect against Enterococcus Faecalis and the compressive strength of the two types of mineral trioxide aggregate mixed with sterile water or 2% chlorhexidine liquidJ Endod 2007 33(7):844-47. [Google Scholar]
[9]. Anumula L, Kumar S, Kumar VS, Sekhar C, Krishna M, An assessment of antibacterial activity of four endodontic sealers on Enterococcus Faecalis by a direct contact test: an in vitro studyISRN Dent 2012 2012:989781 [Google Scholar]
[10]. Weiss EI, Shallav M, Fuss Z, Assessment of antibacterial activity of endodontic sealers by a direct contact testEndo Dent Traumatol 1996 12(4):179-84. [Google Scholar]
[11]. Adl A, Shojaee NS, Motamedifar M, A comparison between the antimicrobial effects of triple antibiotic paste and calcium hydroxide against Entrococcus FaecalisIran Endod J 2012 7(3):149-55. [Google Scholar]
[12]. Saxena P, Gupta SK, Newaskar V, Biocompatibility of root-end filling materials: recent updateRestor Dent Endod 2013 38(3):119-27. [Google Scholar]
[13]. Perez Al, Spears R, Gutmann Jl, Opperman LA, Osteoblasts and MG-63 osteosarcoma cells behave differently when in contact with ProRoot MTA and white MTAInt Endod J 2003 36(8):546-70. [Google Scholar]
[14]. Casemiro LA, Gomes Martins CH, Pires-de-Souza Fde C, Panzeri H, Antimicrobial and mechanical properties of acrylic resins with incorporated silver-zinc zeoliteGerodont 2008 25(3):187-94. [Google Scholar]
[15]. Luddin N, Ahmed HM, The antibacterial activity of sodium hypochlorite and chlorhexidine against Enterococcus Faecalis: a review on agar diffusion and direct contact methodsJ Conserv Dent 2013 16(1):9-16. [Google Scholar]
[16]. Mohammadi Z, Abbott PV, The properties and applications of chlorhexidine in endodonticsInt Endod J 2009 42(4):288-302. [Google Scholar]
[17]. Adl A, Shojaee NS, Motamedifar M, A Comparison between the antimicrobial effects of triple antibiotic paste and calcium hydroxide against Entrococcus FaecalisIran Endod J 2012 7(3):149-55. [Google Scholar]
[18]. Hasan Zarrabi M, Javidi M, Naderinasab M, Gharechahi M, Comparative evaluation of antimicrobial activity of three cements: new endodontic cement (NEC), mineral trioxide aggregate (MTA) and PortlandJ Oral Sci 2009 51(3):437-42. [Google Scholar]
[19]. Al-Hezaimi K, Al-Hamdan K, Naghshbandi J, Oglesby S, Simon JH, Rotstein I, Effect of white-colored mineral trioxide aggregate in different concentrations on Candida Albicans in vitroJ Endod 2005 31(9):684-86. [Google Scholar]
[20]. Wang QQ, Zhang CF, Chu CH, Zhu XF, Prevalence of Enterococcus Faecalis in saliva and filled root canals of teeth associated with apical periodontitisInt J Oral Sci 2012 4(1):19-23. [Google Scholar]
[21]. Odabas ME, Cinar C, Akca G, Araz I, Ulusu T, Yucel H, Short term antimicrobial properties of mineral trioxide aggregate with incorporated silver-zeoliteDent Traumatolo 2011 27(3):189-94. [Google Scholar]
[22]. Uchida M, Antimicrobial zeolite and its applicationsChem Ind 1995 46:48-54. [Google Scholar]
[23]. Kawahara K, Tsuruda K, Morishita M, Uchida M, Antibacterial effect of silver zeolite on oral bacteria under anaerobic conditionsDent Mater 2000 16(6):452-55. [Google Scholar]
[24]. Thom DC, Davies JE, Santerre JP, Friedman S, The hemolytic and cytotoxic properties of a zeolite-containing root end material in vitroOral Surg Oral Med Oral Pathol Oral Radiol Endod 2003 95(1):101-08. [Google Scholar]
[25]. Stowe TJ, Sedgley CM, Stowe B, Fenno JC, The effects of chlorhexidine gluconate (0.12%) on the antimicrobial properties of tooth-colored ProRoot mineral trioxide aggregateJ Endo 2004 30(6):429-31. [Google Scholar]