Surgical Site Infection Caused by Aeromonas hydrophila in a Patient with Underlying Malignancy
Frincy Khandelwal Baruah1, Nishat Hussain Ahmed2, Rajesh Kumar Grover3
1 Senior Resident, Department of Laboratory Medicine, Delhi State Cancer Institute, Delhi, India.
2 Assistant Professor, Department of Laboratory Medicine, Delhi State Cancer Institute, Delhi, India.
3 Director and Chief Executive Officer, Department of Clinical Oncology, Delhi State Cancer Institute, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nishat Hussain Ahmed, Assistant Professor, Department of Laboratory Medicine, Delhi State Cancer Institute, Delhi- 110095, India. E-mail : drnishathussain@rediffmail.com
Aeromonas skin and soft tissue infections in cancer patients can lead to serious life threatening conditions such as cellulitis, necrotizing fasciitis and myonecrosis. We report here a case of surgical site infection, post radical mastectomy, in a 58-year-old female with carcinoma breast. Cultures of exudates from the wound grew Aeromonas hydrophila on repeated occasions. Recovery was uneventful following targeted antimicrobial therapy and regular dressing of the wound. Early suspicion, diagnosis, and treatment with potent antibiotics are needed to prevent any further complications resulting from infection by this emerging pathogen.
Carcinoma breast, Immunocompromised, Necrotising fasciitis, Radical mastectomy, Surgical site infection
Case Report
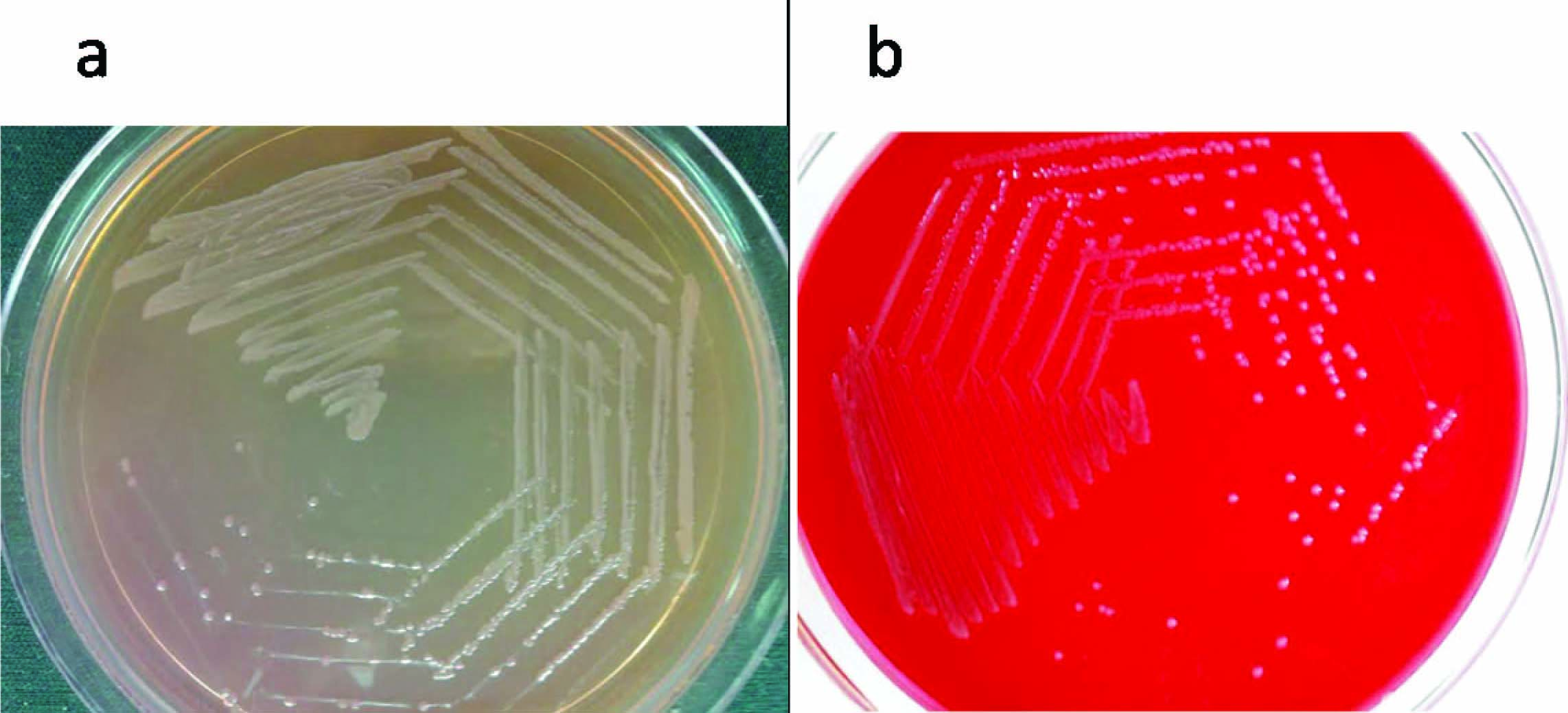
A 58-year-old female, admitted to Delhi State Cancer Institute, a tertiary care centre in Delhi on 23rd Dec’2013 with carcinoma breast, underwent modified radical mastectomy. Postoperative stay was uneventful and the patient was discharged from the hospital in satisfactory condition. However, after two weeks, she revisited with complaints of pain, redness and purulent discharge from the site of surgery. Gram stain of the purulent material revealed plenty of polymorphonuclear cells, and no microorganisms. Later, on culture, pure growth of non-lactose fermenting colonies was obtained on MacConkey agar while on blood agar, the colonies were small, round, opaque and beta hemolytic [Table/Fig-1a&b] The organism was found to be a Gram negative bacillus and motile. The colonies were catalase test and oxidase test positive. The Gram negative rods were identified as Aeromonas hydrophila by the Vitek-2 compact system (BioMe’rieux, North Carolina/USA) with Gram negative GN REF21341 identification (GNID) card. Antimicrobial sensitivity was performed using AST-N281 card which showed the organism to be sensitive to pipercillin/tazobactam (MIC≤4μg/ml), ceftazidime (MIC≤1μg/ml), cefepime (MIC≤1μg/ml), cefoperazone/sulbactam (MIC≤8μg/ml), ciprofloxacin (MIC≤0.25μg/ml), levofloxacin (MIC≤0.12μg/ml), trimethoprim/sulfamethoxazole (MIC≤20μg/ml), imipenem (MIC≤0.25μg/ml) and meropenem (MIC≤0.25μg/ml). A second pus sample from the same site also yielded Aeromonas hydrophila with the same antibiogram which confirmed the pathogenicity of this rare organism. Blood culture obtained on this occasion was found to be sterile. Daily dressing of the wound and administration of levofloxacin, 500 mg for five days helped in proper healing of the wound. Follow up after two weeks was satisfactory and the wound became clean with healthy granulation tissue.
Colonies of Aeromonas hydrophila on a) MacConkey agar and b) Blood agar
Discussion
Aeromonads are Gram-negative rods, oxidase-positive, facultatively anaerobic, widely distributed in aquatic environment [1]. Typically, patients acquire Aeromonas species infection by oral consumption or direct contact with contaminated water or sea food [2].
Aeromonas infection is often polymicrobial and fatality rates range from 28% to 46% in cases of bacteremia mostly caused by Aeromonas hydrophila and Aeromonas veronii biovar sobria [2,3].
In immunocompromised patients, serious fatal infections such as hepatobiliary infection, invasive skin and soft tissue infections, primary bacteremia, burn infections, pleuropulmonary infection, meningitis and endocarditis may also occur [2,4].
Skin and soft tissue infection by Aeromonas hydrophila has been associated with a number of complications such as abscesses, fatal myofascial necrosis, septic arthritis, septic shock, gas gangrene and extremity amputation [5,6].
Necrotizing fasciitis or myonecrosis is often seen in patients with underlying malignancy and can be associated with high mortality rates approaching 60% to 75% [4,7].
In the present case, the patient presented with a non-healing ulcer at surgical site post radical mastectomy which was infected with A. hydrophila. Infection in this case may have been acquired from exposure of wound to contaminated water as this organism has been reported to be present in aqueous environments [1].
An earlier study reported A. hydrophila to be the most common species of Aeromonas causing skin and soft tissue infection among cancer patients [3]. Papadakis et al., reported a patient with fulminant soft tissue infection and septicaemia caused by A. hydrophila during acute lymphoblastic leukemia treatment who recovered well with antibiotic administration and surgical management [8]. Kuo chin et al., also reported a case of serious necrotizing fasciitis due to A. hydrophila in an immunocompromised host which resulted in death of the patient [5].
In India, Mukhopadhyay et al., reported eight cases of Aeromonas infection; out of which, there was one case of skin and soft tissue infection due to A. hydrophila in a 55-year-old male with underlying soft tissue sarcoma. The patient had recovered well with antibiotics and surgical excision of the intramuscular mass [9]. Sood et al., reported isolation of Aeromonas hydrophila from necrotic tissue obtained during fasciotomy in an immunocompetent patient which was resistant to carbapenems and all second and third generation cephalosporins. The patient died within two days of hospitalization due to sepsis and multi organ failure [10].
Though Aeromonas isolates are susceptible to a broad range of antibiotics, the members of this genus may also produce beta lactamase which makes them resistant to ampicillin and first-generation cephalosporins.
Timely diagnosis and prompt antimicrobial administration helped in complete recovery of our patient.
Conclusion
Thus, in light of the complications associated with Aeromonas skin and soft tissue infection, utmost microbiological vigilance is required to promptly identify this rare organism, especially in immune-compromised patients such as those with underlying malignancy; so that timely management of the condition is possible with appropriate antibiotics and surgical debridement, irrigation etc, if required.
[1]. Igbinosa IH, Igumbor EU, Aghdasi F, Tom M, Okoh AI, Emerging Aeromonas species infections and their significance in public healthScientific World Journal 2012 2012:625023 [Google Scholar]
[2]. Okumura K, Shoji F, Yoshida M, Mizuta A, Makino I, Higashi H, Severe sepsis caused by Aeromonas hydrophila in a patient using tocilizumab: a case reportJ Med Case Reports 2011 5:499 [Google Scholar]
[3]. Chao CM, Lai CC, Gau SJ, Hsueh PR, Skin and soft-tissue infection caused by Aeromonas species in cancer patientsJournal of Microbiology, Immunology and Infection 2013 46(2):144-46. [Google Scholar]
[4]. Janda JM, Abbott SL, The genus Aeromonas: taxonomy, pathogenicity, and infectionClin Microbiol Rev 2010 23:35-73. [Google Scholar]
[5]. Kuo-Chun L, Po-Tsung Y, Cheng L, Necrotizing fasciitis caused by inconspicuous infection of Aeromonas hydrophila in an immunocompromised hostJ Surg Case Rep 2010 7:2 [Google Scholar]
[6]. Behera B, Bhoriwal S, Mathur P, Sagar S, Singhal M, Misra MC, Post-traumatic skin and soft tissue infection due to Aeromonas hydrophilaIndian J Crit Care Med 2011 15(1):49-51. [Google Scholar]
[7]. Fatima A, Afridi FI, Qureshi A, Farooqi BJ, Hussain A, Bacteremia due to Aeromonas hydrophila in Acute Lymphoblastic LeukemiaJ Coll Physicians Surg Pak 2013 23(12):893-95. [Google Scholar]
[8]. Papadakis V, Poniros N, Katsibardi K, Charissiadou AE, Anastosopoulos J, Polychronopoulou S, Fulminant Aeromonas hydrophila infection during acute lymphoblastic leukemia treatmentJ Microbiol Immunol Infect 2012 45:154-57. [Google Scholar]
[9]. Mukhopadhyay C, Chawla K, Sharma Y, Bairy I, Emerging extra-intestinal infections with Aeromonas hydrophila in Coastal region of Southern KarnatakaJ Postgrad Med 2008 54:199-202. [Google Scholar]
[10]. Sood S, Nerurkar V, Fatal Necrotizing Soft Tissue Infection by Aeromonas hydrophilaJournal of Clinical and Diagnostic Research 2014 8(4):6-7. [Google Scholar]