Intraosseous Epidermoid Cyst Associated with Impacted Mandibular Wisdom Teeth: An Uncommon Entity
Orcun Toptas1, Ismail Akkas2, Mustafa Tek3, Fatih Ozan4, Cetin Boran5
1Assistant Professor, Department of Oral and Maxillofacial Surgery,Abant Izzet Baysal University Bolu,Turkey.
2Faculty, Department of Oral and Maxillofacial Surgery,Abant Izzet Baysal University Bolu,Turkey.
3Faculty, Department of Oral and Maxillofacial Surgery,Abant Izzet Baysal University Bolu,Turkey.
4Faculty, Department of Oral and Maxillofacial Surgery,Abant Izzet Baysal University Bolu,Turkey.
5Faculty, Department of Pathology and Medicine,Abant Izzet Baysal University Bolu,Turkey.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Orçun Toptas, Assistant Professor, Department of Oral and Maxillofacial Surgery, Abant Izzet Baysal University Bolu, Turkey.
E-mail: otoptas@ibu.edu.tr
Epidermoid and dermoid cysts of the jaws are seen rarely. The formation theories of the intraosseous epidermoid cyst (IEC) are not clear. The radiographic appearance is similar with unilocular cysts. Surgical enucleation is the suggested treatment method for epidermoid cysts. This case report presents bilateral mandibular intraosseous epidermoid cysts with impacted wisdom teeth which is the first documented case in the literature.
Enucleation, Epidermoid cyst, Impacted wisdom teeth, Mandible
Case Report
A 24-year-old patient was referred to our clinic for treatment of impacted wisdom teeth. The patient had odontogenic pain on upper and lower right jaw. Clinical examination showed that upper and lower right first molars have deep caries and pulpitis pain. The wisdom teeth were not seen in mouth clinically. The patient anamnesis gives no wisdom teeth extraction story in past. The orthopantomograph was taken to see the positions and situations of all wisdom teeth. Bilaterally impacted teeth surrounded by large radiolucency were detected by orthopantomograph [Table/Fig-1].
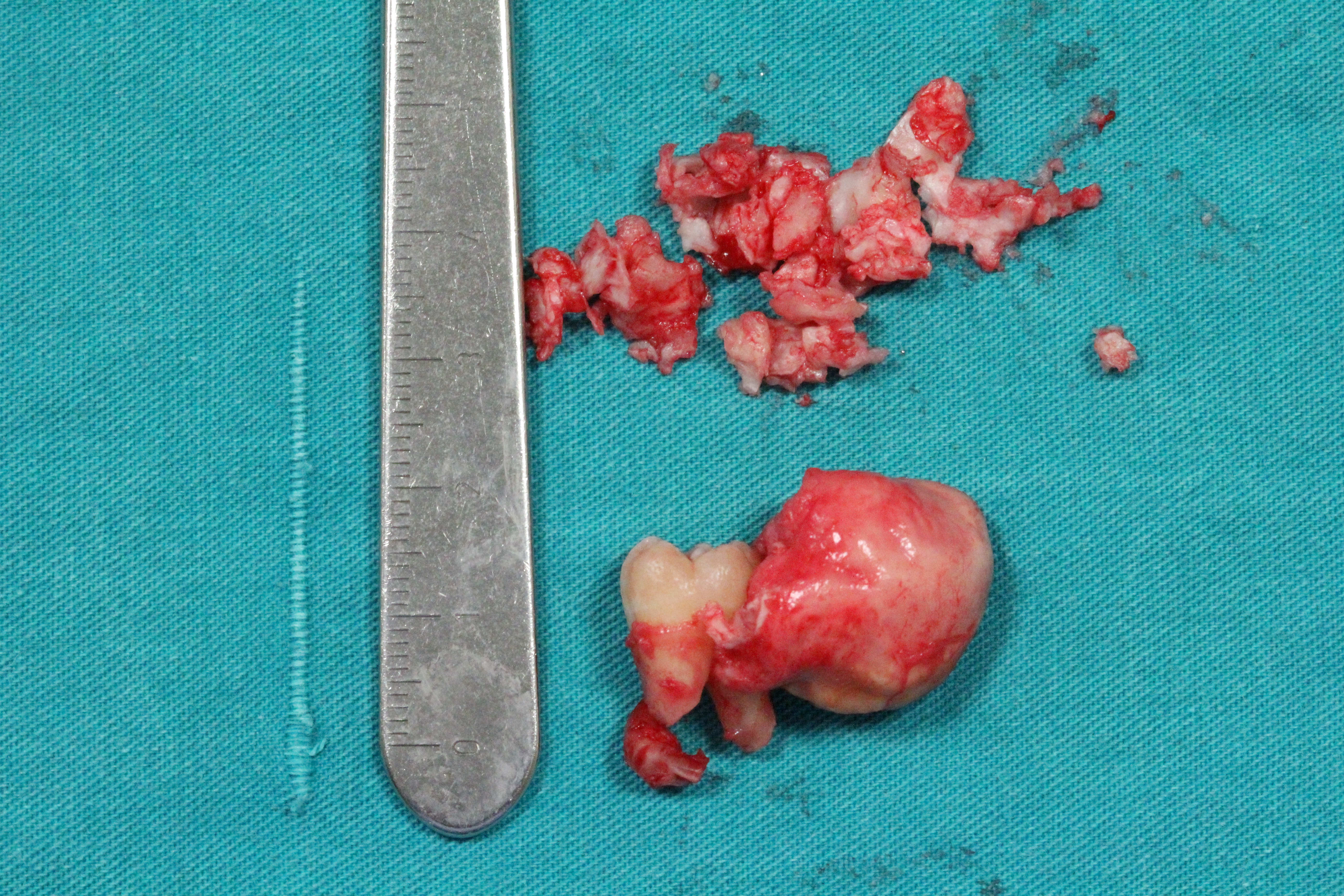
cystsThe patient had no complaints like swelling, pain, paresthesia etc. related to the cystic lesions. The results of clinical and radiological examination was considered the odontogenic cyst especially dentigerous cyst, ameloblastoma, and keratocystic odontogenic tumour. Because of surgical accessibility of lesion and typical odontogenic cyst appearance on radiograph, the aspiration biopsy was not performed. Instead, it was decided the enucleation of the lesion directly. Surgical procedure was performed under local anesthesia. Lesions were elastic, and consisted of cheese-like masses and enucleated with associated impacted third molars. Macroscopically, the specimens were cysts with smooth surfaces [Table/Fig-2].
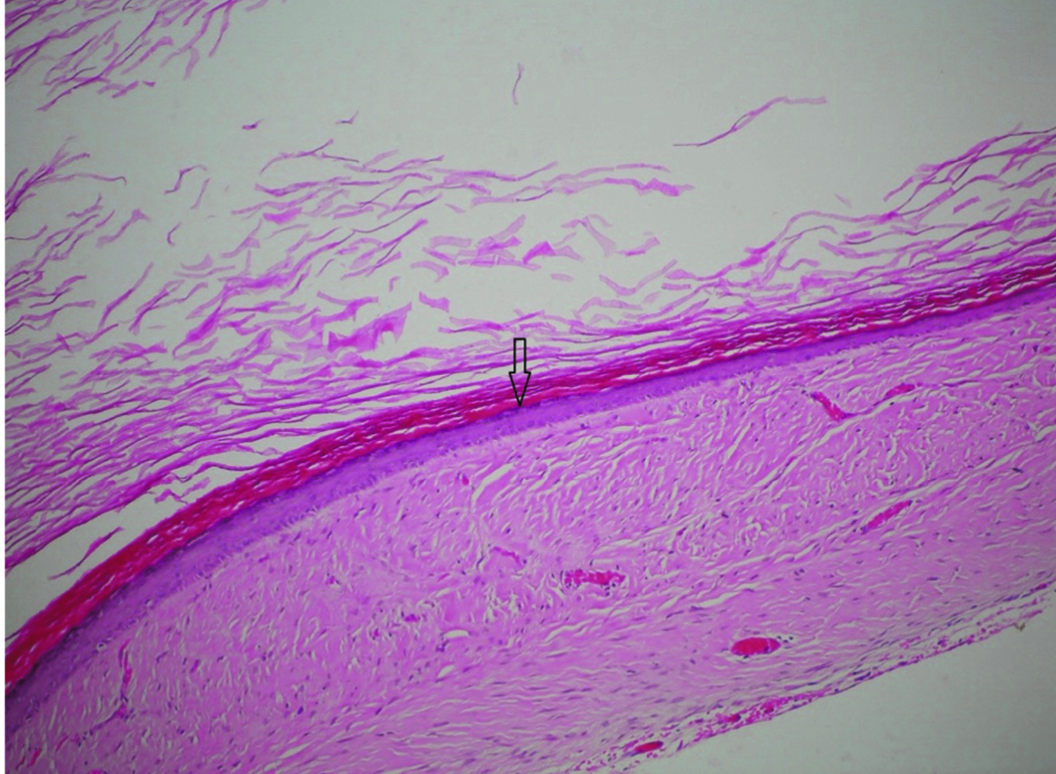
Histopathologically, cyst wall was showing stratified squamous epithelial lining with orthokeratotic production which is similar to epidermis. But, the lesion wall had no skin appendage that confirms the diagnosis of the lesion as IEC instead of dermoid cyst [Table/Fig-3].
Radiological view of the bilateral intraosseous epidermoid cystsThe

Macroscopic appearence is smooth-surfaced, elastic mass associated with impacted tooth
Histological view of epidermal cyst showing stratified squamous epithelial lining (arrow) with orthokeratotic production (H&E, X100)
Discussion
The causes of both epidermoids and dermoids include failure of surface ectoderm to separate from underlying structures, sequestration and implantation of surface ectoderm. Most congenital dermoid and epidermoid cysts probably arise due to an embryologic accident during the early stages of development, between 3 and 5 weeks of gestation. Enclosed ectodermal cysts can occur when the surface ectoderm fails to separate completely from the underlying neural tube. Alternately, they may result from abnormal sequestration or invagination of surface ectoderm along the embryologic sites of dermal fusion that form the eyes, ears, and face [1,2]. In literature search, we couldn’t find any intraosseous epidermoid cyst (IEC) located in the mandibula bilaterally and associated with impacted mandibular third molars.
Up to now numerous ıntraosseous epidermoid lesions were reported by many authors. Shear defined a primary intraalveolar epidermoidcarcinoma [3]. In World Health Organization (WHO) classification system, primary intraosseous carcinoma term recommended in lieu primary intraalveolar carcinoma [4]. It has been considered that the malignant alterations of the odontogenic cyst epithelia is the major cause of the primary intraalveolar epidermoid carcinomas [3]. Ishida et al., showed multiple intraosseous epidermoid and trichilemmal characterised lesions in tibia as a rare manifestation of Gardner syndrome [5]. Arora et al., described a subungual IEC by sonographie [6].
The epidermal lesions especially IEC can occur anywhere at the body. The pathogenesis of IEC is not clear. Generally it has been thought that the entrapped epidermal tissues in other tissues by trauma or iatrogenic causes differentiates the IEC [6]. IEC is named as “epidermoid inclusion cyst” and located commonly in subungual region [7]. In our case IECs were placed bilaterally and both of them were associated with impacted third molars. A case that implantation type epidermoid cyst injury in the mandible due the gun shot presented in the literature [8]. In our case, the patient was a temporary military private but has no trauma or gunshot injury story.
Dermoid, epidermoid and teratoid cysts can develop in midline or sublingual region in oral cavity [9,10]. Congenital epidermoid cysts are usually originated from fuse site of embryogenic parts especially 1st and 2nd branchial archs[10]. The acquired type of the cyst generally originates from trauma, inflammation, surgery or iatrogeniccauses [10,11]. The reports defines the dermoid or epidermoid cysts in the midline of the body and most frequently in the periorbital region in head and neck [12]. The production theories of IEC of the mandible are various. Embryonic ectoderm entrapment theory seems invalid for our case. Although the cysts were bilateral, there is no embryonic cleft in angulus mandible region and also the IECs had no skin appendages like hair follicles and sweat glands. The second theory suggests the Fordyce’s granules which migrates from oral mucosa into bone through fistula or due the surgical operations as the origin of IECs [13]. Because of detecting no fistulas or no surgical history from patient, this theory seems also invalid for our case. Final theory explains the reason of IECs by metaplasia of the epithelium of dentigerous cysts. Sebaceous differentiation of cyst wall byinduction of mesodermal organizer causes the epidermoid cysts [14]. This theory also supports the absence of skin appendages in our case. The attached impacted teeth also preoccupies that thelast theory is suitable for mandibular IECs.
The researchers suggests the diagnostic work up for IEC including ultrasonography, computed tomography or magnetic resonanceimaging to evaluate the adjacent anatomical structures, determine the exact location of lesion and decide the appropriate surgical approach [14]. In our case, we used only orthopantomographs and did not consider the IEC in differential diagnosis. The aspiration biopsy was not performed, either, because IEC is very rare condition and the lesions were bilaterally placed with impacted third molar teeth.
Histopathologically, cyst wall was showing stratified squamous epithelial lining with orthokeratotic production which is similar to epidermis. Histologic appearance of epidermoid cyst is similar to keratocystic odontogenic tumour. However, keratocystic odontogenic tumours have high level keratinising epithelial layer which is separated from basal cell layer, epidermoid cysts have mild keratinising epidermis. The absence of skin appendages eliminated the dermoid cyst in diagnosis.
Conclusion
The lesion enucleated by intraoral approach which is suitable and suggested technique for IECs. It is important that IEC should be placed in differential diagnosis of mandibular cystic lesions in dental practice. The aspiration biopsy and further radiological investigations like ultrasonography, computed tomography or magnetic resonance imaging should be considered for cystic lesions of the jaws. Although, we have a large literature of jaw pathologies, we may still come across unique and unclear cases. Clinical examination, conventional radiographs and surgical experience is not enough for diagnosis of all pathologies. Our case is very rare and first case in the literature because of bilateral placement and being relationship with impacted third molars.
[1]. MH Brownstein, EB Helwig, Subcutaneous dermoid cystsArchives of Dermatology. 1973 107(2):237-39.Epub 1973/02/01 [Google Scholar]
[2]. BL Pear, Epidermoid and dermoid sequestration cysts.The American journal of roentgenology, radium therapy, and nuclear medicine. 1970 110(1):148-55.Epub 1970/09/01. [Google Scholar]
[3]. M Shear, Primary intra-alveolar epidermoid carcinoma of the jawThe Journal of pathology 1969 97(4):645-51.Epub 1969/04/01. [Google Scholar]
[4]. RP Elzay, Primary intraosseous carcinoma of the jaws. Review and update of odontogenic carcinomasOral surgery, Oral Medicine, and Oral Pathology 1982 54(3):299-303.Epub 1982/09/01. [Google Scholar]
[5]. T Ishida, S Abe, Y Miki, T Imamura, Intraosseous pilomatricoma: a possible rare skeletal manifestation of Gardner syndrome.Skeletal Radiology 2007 36(7):693-98.Epub 2007/01/20 [Google Scholar]
[6]. A Arora, D Srivastava, H Gupta, V Kumar, PP Kotwal, Sonographic diagnosis of subungual intraosseous epidermoid cystJournal of Clinical Ultrasound : JCU 2013 41Suppl 1:35-7. Epub 2013/07/24 [Google Scholar]
[7]. HJ Baek, SJ Lee, KH Cho, HJ Choo, SM Lee, YH Lee, Subungual tumours: clinicopathologic correlation with US and MR imaging findingsRadiographics: a review publication of the Radiological Society of North America, Inc 2010 30(6):1621-36.Epub 2010/11/13 [Google Scholar]
[8]. CE Noffke, Implantation-type epidermoid cyst of the mandibleDento Maxillo Facial Radiology 1999 28(6):383-85.Epub. 1999/12/01 [Google Scholar]
[9]. H Leveque, CA Saraceno, CK Tang, CL Blanchard, Dermoid cysts of the floor of the mouth and lateral neck.The Laryngoscope 1979 89(2):296-305.Epub 1979/02/01. [Google Scholar]
[10]. C Makos, G Noussios, M Peios, S Gougousis, P Chouridis, Dermoid cysts of the floor of the mouth: two case reportsCase Reports in Medicine 2011 2011(362170.)Epub 2011/09/17. [Google Scholar]
[11]. M Kudoh, H Harada, K Omura, Y Ishii, Epidermoid cyst arising in the submandibular regionCase reports in medicine 2013 2013(419289.)Epub 2013/11/06 [Google Scholar]
[12]. C Bonet-Coloma, I Minguez-Martinez, C Palma-Carrio, B Ortega-Sanchez, M Penarrocha-Diago, JM Minguez-Sanz, Orofacial dermoid cysts in pediatric patients: a review of 8 cases.Medicina Oral, Patologia Oral Y Cirugia Bucal 2011 16(2):e200-3.Epub 2010/08/17 [Google Scholar]
[13]. M Dror, SC Allon, Kaplan. Ilana, Intraosseous compound-type dermoid cyst of the jawInternational Journal of Head and Neck Surgery 2010 1(2):103-06. [Google Scholar]
[14]. BL Bodner, Y Woldenberg, N Sion-Vardy, Dermoid cyst of the maxillaInternational Journal of Oral and Maxillofacial Surgery 2005 34(4):453-55.Epub 2005/08/02 [Google Scholar]