The goal of root canal therapy is the elimination of infected tissue and prevention of apical tissue [1]. Proper root canal shaping is the predictive factor for the success of endodontic treatment. Root canal shaping aims to eliminate microorganism, remove infected and necrotic dentin and shape the root canal system [2]. Mechanical root canal instrumentation should create a continuous tapered preparation in order to facilitate antiseptic irrigation and the placement of filling materials [3]. Various techniques have been proposed for canal preparation including corono-apical and apico-coronal [4]. In endodontics, shaping of root canals has been proposed using various Ni-Ti rotary instruments [5]. Limited procedural errors, reduction in operator fatigue and preparation time has been considered to be the advantages of Ni-Ti instruments over stainless steel instruments [6]. In primary teeth, pulpectomy is the choice of treating decayed primary teeth with pulpal involvement, thus preserving the integrity of the dental tissues [7]. Pulpectomy is a procedure involving complete removal of pulp tissue from the root canal space in primary teeth followed by filling it with an inert resorbable material [7,8]. Using hand files for instrumentation of the primary root canals has been well documented in the literature [9]. There are certain potential limitations like increased canal preparation time, uneven preparation of root canal space associated with the use of hand files despite its widespread usage for the instrumentation of primary root canals [10]. To overcome the disadvantages of the manual instrumentation and to preserve the tortuous root canal path of the primary teeth, rotary instrumentation was introduced into paediatric dentistry.
Only a handful of studies have been reported using different rotary file systems for canal instrumentation in primary teeth [11-22]. Use of ProTaper system in primary teeth has been reported and is well accepted [11,12]. Till date, one clinical study has been documented the use of K3 rotary file system for canal instrumentation in primary teeth [13]. Use of rotary files, being an emerging practice in the field of paediatric dentistry, it is essential to conduct systematic clinical trials to arrive to definite conclusive results. Hence, the aim of this study was to comparatively evaluate the instrumentation time and the quality of canal filling on using manual instrumentation and two different rotary file systems – ProTaper and K3 rotary file techniques for instrumentation of the primary teeth.The hypothesis of the present study is that there is a significant difference in the instrumentation time and quality of obturation using modified rotary instrumentation technique compared to manual instrumentation in primary molars.
Materials and Methods
The randomized clinical trial was carried out in the Department of Paediatric and Preventive Dentistry, Saveetha Dental College, Tamil Nadu, India and Hospitals following the approval from the Institutional Review Board (STP/SDMDS2015PED42) from November 2016-February 2017. The informed consent was obtained from the parents of the children who participated in the study.
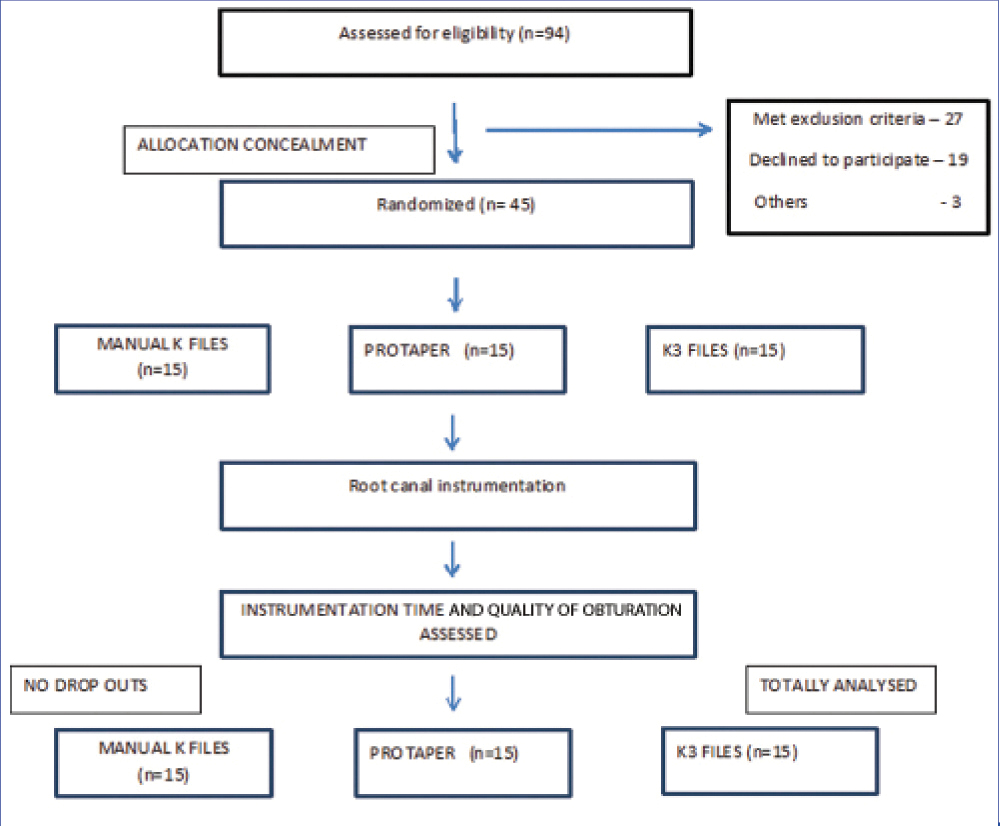
The sample size was calculated from a previous study with 95% power using G Power analysis and arrived to a total sample of 45 [13]. Children between 4-8 years of age requiring pulpectomy in any one of the primary mandibular molars were randomly selected and allotted to one of the three groups according to the computer generated randomization sequence where instrumentation was done using: Group 1: Manual K-files (15-30) (Mani); Group 2: S2 ProTaper rotary file (Dentsply/Maillefer, Switzerland); Group 3: K3 rotary system (0.04 taper, 0.25 tip) (Sybron Dental, westcollins, CA, USA) [Table/Fig-1]. The inclusion criteria considered for selecting the children are: vital or non-vital mandibular primary molars without sinus tract, absence of internal or external pathologic root resorption, patients having pain during night, presence of adequate coronal tooth structure to receive Stainless Steel (SS) crown. The exclusion criteria involved the children lacking cooperative ability, children with underlying systemic diseases and those with special healthcare needs.
Flow chart describing the randomization of the participants and the parameters evaluated during the clinical trial.
A full mouth examination with intraoral periapical radiographs of the teeth indicated for pulpectomy was taken prior to the start of the clinical procedure. The working length was determined with the pre-operative radiograph using Ingle’s radiographic method [23]. Local anesthesia was administered using 2% lignocaine with 1:2,00,000 adrenaline (LOX* 2% ADRENALINE, Neon Laboratories limited, India). The tooth indicated for pulpectomy was isolated using rubber dam (GDC Marketing, India) for better visibility and to improve the efficiency of the operator. Using No.6 round bur (Mani) was used in a high speed hand piece to remove the superficial caries and No.330 pear shaper bur (Mani) was used to completely de-roof the pulp chamber. No.10 size K file (Mani) was used to determine the patency of the canals. The canal preparation was done using:
Group 1: Fifteen teeth were instrumented using K-files from size 15 to size 30 (Mani) in quarter pull turn method.
Group 2: Fifteen teeth were instrumented using only S2 ProTaper file (Dentsply India Pvt. Ltd., Delhi, India) till the working length using X-Smart endodontic motor (Dentsply India Pvt. Ltd., Delhi, India).
Group 3: Fifteen teeth were instrumented using (4 % taper, 0.25 tip) K3 (Sybron Dental, Westcollins, CA, USA).
A 0.25 tip 4% taper rotary file using X-Smart endodontic motor (Dentsply India Pvt. Ltd., Delhi, India) till the full working length.
The time taken for the instrumentation of the canals was recorded in seconds using a stop watch by an assistant. The canals were then irrigated with physiologic saline and the canals were dried using sterile absorbent paper points. Calcium hydroxide and iodoform paste (Metapex, Meta Biomed co. Ltd., Korea) was used for the canal obturation by gently pushing the paste with cotton pellets.
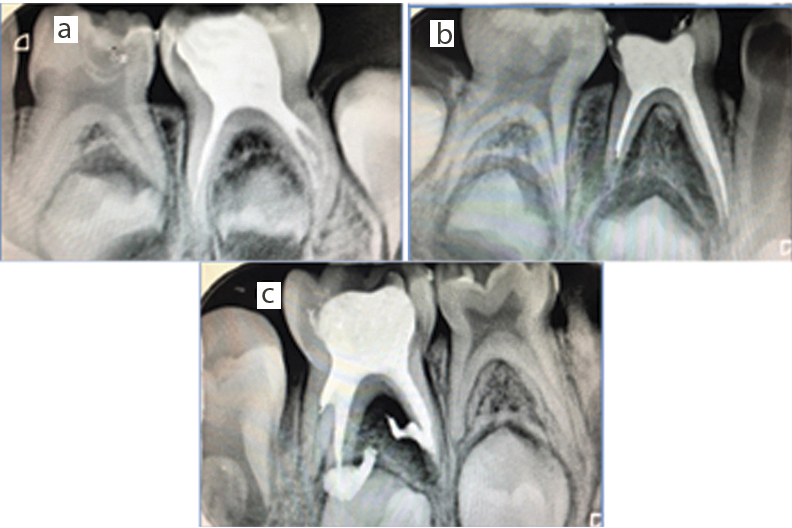
A postobturation radiograph was taken to assess the quality of obturation. The assessment of obturation quality was graded as under filling-all the canals were filled more than 2 mm short of the apex, optimal filling- one or more of the canals having ZOE ending at the radiographic apex or upto 2 mm short of the apex, over filling-any canal showing ZOE outside the root (modification of Coll JA and Sadrian R) [24] by another paediatric dentist who was blinded to the type of instrumentation used for canal preparation. The glass ionomer cement (Shofu, Shofuinc. Japan) was used as the entrance filling and was restored with SS crown on the same appointment.
Statistical Analysis
The statistical analysis was done using SPSS software version 17.0 (SPSS Inc., Chicago, IL, USA). The mean values of different study groups were compared using ANOVA and Chi-square test. ANOVA test was used to compare the instrumentation time between the groups followed by Tukey post-hoc analysis to list out the significant groups with a significance level set at 5% level. Pearson’s Chi-square test was used to compare the quality of obturation between the groups. In the current study, p<0.05 was considered as the level of significance.
Results
A total of 45 healthy children (21 females and 24 males) participated in the study. The distribution of the participants is tabulated in [Table/Fig-2]. Of 45 treated primary mandibular molars, 9 (20%) and about 11 (24.4%) were mandibular left primary first and second molars respectively. Mandibular right first and second molars comprised of 9 (20%) and 16 (35.6%) respectively. An intergroup comparison using ANOVA and Chi-square test indicated an equal distribution of the subjects between the three groups with respect to the age (p= 0.968); gender (p=0.765) and distribution of teeth (p=0.812). With respect to the quality of obturation among the groups, 53% (n=8) of the teeth instrumented with hand files; 60% (n=9) of the teeth instrumented with ProTaper and 67% (n=10) of the teeth instrumented with K3 rotary files showed optimal fill [Table/Fig-3]. Intergroup comparison between the three groups showed no significant differences (p=0.791) [Table/Fig-4].
Demographic variables describing sample size, age and percentage of male and female participants in each group.
| Groups | Ν (Sample Size) | Age (mean+ standard deviation) | Female (21) | Male (24) |
|---|
| K file | 15 | 5.60+1.121 | 53.3% (8) | 46.7% (7) |
| ProTaper | 15 | 5.60+1.183 | 40.0% (6) | 60.0% (9) |
| K3 | 15 | 5.67 +1.496 | 46.7% (7) | 53.3% (8) |
| Total | 45 | 5.62+1.248 | 46.7% (21) | 53.3% (24) |
Immediate postoperative radiographic showing different quality of obturation a) under filling; b) optimal filling; c) over filling.
Comparison of quality of obturation among the different groups described in percentage. Intergroup comparison between the three groups revealed no significant differences.
| Assessement of quality of obturation | Hand files | Protaper files | K3 Files | over all p-value* |
|---|
| Under fill | 6.7% | 13.3% | 13.3% | 0.791 |
| Optimal fill | 53.3% | 60% | 66.7% |
| Over fill | 40.0% | 26.7% | 20.0% |
p<0.05 statistically significant values.
The mean instrumentation time was recorded and an intergroup comparison was done using ANOVA test. A statistically significant difference was noted between the three groups (p<0.001) [Table/Fig-5]. Tukey post-hoc analysis confirmed that there was a significant difference in the instrumentation time between all the three groups [Table/Fig-6].
Comparison of instrumentation time among three groups.
| Instrumentation time (in seconds) | N | Mean | Std. Deviation | Over all p-value* |
|---|
| K file | 15 | 95.47 | 12.716 | <0.001 (sig.) |
| ProTaper | 15 | 45.93 | 10.074 |
| K3 | 15 | 64.73 | 16.276 |
| Total | 45 | 68.71 | 24.379 |
Over all p-value is significant (p<0.05).
Intergroup comparison of instrumentation time among the groups.
| Groups | Groups | Over all p-value* |
|---|
| K file | ProTaperK3 | <0.001 (sig) |
| ProTaper | K3 | <0.001 (sig) |
| K3 | K fileProTaper | <0.001 (sig) |
Over all p-value is significant (p<0.05).
Discussion
The present study compared the quality of obturation and the instrumentation time of manual and two rotary systems in preparation of primary mandibular molars. The objective of treating an infected primary tooth in children is to retain it in the oral cavity until its physiological exfoliation to guide the erupting permanent teeth [7]. Retention of the primary teeth can be made possible by performing root canal procedure. Pulpectomy of the primary teeth involves removal of the infected tissue from the root canal and filling it with a resorbable material [6]. In recent years, endodontic instruments and techniques have undergone various modifications to attain the better cleaning and shaping efficacy [14]. Ni-Ti instruments are proven to be efficient and safe during root canal preparation in curved canals due to their better elasticity and flexibility. This study was a randomized clinical trial that compared the instrumentation time and the quality of obturation of ProTaper file system and K3 rotary systems with the traditional manual instrumentation in primary teeth.
Guidelines for the sequence of using rotary files in primary teeth have not been established. Potential limitation for its use in primary teeth is due to the morphology of the primary teeth [7]. Primary teeth have softer root dentin, curved roots with undetectable root tip resorption and ribbon shaped root morphology [8]. Hence, a modified sequence for rotary instrumentation of the primary root canals has to be established. In the current study only, S2 file in ProTaper system and 0.25 tip 4% taper of K3 rotary file were used for root canal instrumentation. This modified sequence combined with its use in a torque limited hand piece resulted in no instrument separation within the canals. However, in the previous study done by Romero TO et al., in 2011, K3 instrumentation was done using 0.06 taper file, progressively increasing to the next three larger files in a crown down technique [13]. ProFile 0.04 rotary file, when used for canal instrumentation in primary teeth resulted in better root canal obturation compared to manual instrumentation [15] whereas, in our study, there was no significant difference in the quality of obturation of the primary teeth using rotary files. Romero TO et al., reported 80%, 50% optimal filling with K3 rotary files and manual instrumentation respectively. Whereas, in our study, optimal filling was 67% using k3 rotary file system for primary root canal instrumentation followed by ProTaper 60% and hand instrumentation 53%. There were no significant differences between the three groups with respect to the obturation quality. This result is in contradiction to the study reported by Romero TO et al., who reported superior obturation quality with rotary files in primary teeth [13]. This controversial result could be attributed due to the use of different material for obturation and different techniques for obturation.
A statistically significant reduction was noticed in the instrumentation time on using K3 rotary file system for primary root canal instrumentation [13]. Rosa FM et al., reported K3 rotary files showed lesser instrumentation time compared to hand instrumentation technique in primary teeth [19]. Comparison of instrumentation time between manual files, ProTaper rotary files and Hero 642 rotary files revealed rotary files had lesser instrumentation time than manual files [21]. In this present study, instrumentation time for preparation of primary molars with ProTaper system (46 seconds) was significantly shorter compared to the K3 rotary system (65 seconds) and manual instrumentation (95 seconds).This reduction in the instrumentation time significantly reduces the chairside procedural time which in turn positively influences the behavior of the child during the treatment. On literature search, there is a lack in the clinical studies reported to evaluate the quality of root canal obturation and instrumentation time in primary teeth using modified rotary file systems. Further research on the clinical use of various rotary files in primary teeth will aid in the development of a new, faster and safer protocol for endodontic treatment in the primary teeth.
Limitation
The limitation of the present study is that only two-dimensional evaluation of the quality of obturation was performed using intraoral periapical radiograph. Long term follow up is required to assess the clinical and radiographic success of the pulpectomy procedure performed using different instrumentation techniques.
Conclusion
The obturation quality with rotary system is more acceptable than manual instrumentation technique. There is a reduction in instrumentation time during pulpectomy procedure with use of rotary file in primary molars. Therefore, a modified ProTaper or K3 rotary systems can be used as an alternative technique during root canal preparation of primary teeth.
*p<0.05 statistically significant values.
*Over all p-value is significant (p<0.05).
*Over all p-value is significant (p<0.05).