Atlantooccipital Fusion: Prevalence and its Developmental and Clinical Correlation
D. K. Sharma1, Deepak Sharma2, Vandana Sharma3
1 Additional Professor, Department of Anatomy, AIIMS, Raipur, Chhattisgarh, India.
2 Demonstrator, Department of Anatomy, Gandhi Medical Colledge, Bhopal, Madhya Pradesh, India.
3 Associate Professor, Department of Anatomy, Gandhi Medical Colledge, Bhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. D. K. Sharma, Additional Professor, Department of Anatomy, AIIMS, Raipur-492099, Chhattisgarh, India.
E-mail: drdksharma@aiimsraipur.edu.in
Introduction
Atlantooccipital fusion or occipitalization of atlas or assimilation of atlas is a rare or uncommon abnormality recorded in anatomical, morphological and radiological studies. It is usually associated with reduction in dimensions of foramen magnum leading to acute or chronic neurovascular compression and clinical manifestations of varying severity. Though, atlantooccipital fusion is rare but it is important and significant for the physicians and surgeons for their diagnostic and therapeutic approach.
Aim
To know the prevalence of atlantooccipital fusion in South Asian population predominantly in Central India and its embryological and clinical correlation by reviewing literature and earlier studies.
Materials and Methods
This study included careful examination for the atlantooccipital fusion on total 192 human skulls of both genders, available in the Department of Anatomy AIIMS Raipur, Chhattisgarh, India, Department of Anatomy and Forensic Medicine of Gandhi Medical Colledge, Bhopal, Madhya Pradesh, India and Pt. Jawahar Lal Nehru Memorial Medical College, Raipur. Morphometric measurements of the abnormal skulls were done, analysed and recorded. Observations and findings of this study were correlated embryologically and clinically with the results and claims of previous studies and literature, and accordingly the conclusions were drawn.
Results
We found only two skulls with atlantooccipital fusion, in overall study of 192 skulls. The first skull showed incomplete atlantooccipital fusion on the left side with little right lateral inclination and missing posterior tubercle/spinous process and adjoining part of posterior arch of atlas, whereas the second skull showed complete atlantooccipital fusion.
Conclusion
We conclude that the prevalence of atlantooccipital fusion including complete and incomplete fusion was 1.04%, which is higher than the proclaimed prevalence rate of 0.12% to 0.72%, by the previous studies. In accordance with the fact that the atlantooccipital fusion represents a synostosis between the atlas and the occipital bone due to developmental abnormal segmentation of cranial part of paraxial mesoderm and abnormal fusion between segments of caudal occipital and cranial cervical sclerotomes, we would like to thereby assert that the fusion associated with the reduction in dimensions of foramen magnum (reduction also seen in our study) is definitely significant for diagnostic and therapeutic purposes to clinicians.
Compression, Foramen magnum, Inclination, Variation
Introduction
Skeletal variations of craniovertebral region have been recorded in the anatomical, morphological and radiological studies. Atlantooccipital fusion is congenital fusion of atlas with the occipital bone. It is one of the rare skeletal variations of the craniocervical region with the occurrence of 0.12% to 0.72%. Person with occipitalization of atlas may have one or more physical features like low hairline, torticollis, restricted neck movements, abnormal short neck and during neurological examination he or she may reveal symptoms and signs like headache, neck pain, numbness and pain in the limbs, weakness, abnormal head posture, tinnitus, visual disturbances and lower cranial nerve palsies leading to dysphagia and dysarthria. Headaches aggravated by Valsalva maneuvers, such as yawning, laughing, crying, coughing, sneezing or straining, bending over, or getting up suddenly [1]. Not all cases of atlantooccipital fusion can be easily distinguished as Arnold-Chiari malformation has similar pathophysiology [2]. There may be varying degree of atlantooccipital fusion that may result in complete and partial assimilation [3].
Fusion between atlas and occipital bone occurs anteriorly between the arch and rim of the foramen with some segment of the posterior arch of atlas present in some instances. This fragment can frequently constrict the spinal canal causing intermittent symptoms depending on the position of the head. Fusion of the atlas to the skull is more or less complete but involves one lateral mass usually. The fusion may involve both lateral masses and mid part of anterior arch and more rarely the entire lateral arch. Two superior facets on the lateral masses completely fuse with the occipital condyles, and the anterior arch incompletely fuses with the basilar part of occipital bone [4]. In majority of reported cases, fusion occurs between anterior arch of atlas and anterior rim of foramen magnum and may be associated with other skeletal malformation as spina bifida of atlas and Klippel-Feil syndrome [5].
In condition of atlantooccipital fusion, the atlas appears as a part of occiput structurally as well as functionally. Atlantooccipital fusion is associated with narrowing of foramen magnum with compression of spinal cord or brain stem. Hypoplasia of the basiocciput can be found in manifestations of the occipital vertebra, in atlas assimilation and in atlantooccipital fusion. These patients with craniovertebral joint anomalies exhibit the first neurological signs and symptoms usually no sooner than the second decade. Atlas assimilation may include alteration of the atlantooccipital articulation or narrowing of the spinal canal. Most of the abnormalities cause no typical symptom, but some patients have neurological problems [6].
This anatomical variation may remain unnoticed until the patient undergoes clinical or radiological investigation for the treatment of symptoms or may be encountered as surgical, autopsy finding or during morphological studies of skull.
Materials and Methods
The study was performed to examine the prevalence of fusion between occipital and atlas bones in the department of anatomy on the available skulls (including skull bases) at the institutes that the authors are associated with. The study included careful examination of 192 human skulls (of both genders) in respective institutes by the authors collectively during third quarter of the year 2016. The institutions involved are as follows:
Department of Anatomy AIIMS Raipur – 25 skulls;
Department of Anatomy and Forensic Medicine Gandhi Medical Colledge Bhopal – 54 skulls;
Department of Anatomy and Forensic Medicine Pt. Jawahar Lal Nehru Memorial Medical College Raipur – 113 skulls;
The study revealed only two skulls with occipitalization of atlas. Morphometric measurements of these abnormal skulls were done, analysed and recorded as [Table/Fig-1] [2].
Morphometric measurements of the skulls with atlantooccipital fusion.
| S. No. | Measurements | Skull-1 | Skull-2 |
|---|
| 1 | Anteroposterior diameter of foramen magnum | 33 mm | 26 mm |
| 2 | Transverse diameter of foramen magnum | 25 mm | 19 mm |
| 3 | Anteroposterior diameter of foramen magnum behind the odontoid process | 16 mm | 13 mm |
| 4 | Anteroposterior diameter of right condylar facet | 17 mm | 19 mm |
| 5 | Transverse diameter of right condylar facet | 16 mm | 15 mm |
| 6 | Anteroposterior diameter of left condylar facet | 18 mm | 20 mm |
| 7 | Transverse diameter of left condylar facet | 18 mm | 17 mm |
| 8 | Cranial index | 69.5% | 70.5% |
The skulls were accumulated over a period of time in these institutes, after cadaveric dissections every year. The skulls were roughly 4 to 50-year-old and were examined in the respective institutes.
All three institutes involved are Central and State Government organizations. The study would aid further research activities around diagnostic and therapeutic purposes. The study obviously doesn’t affect anybody’s moral rights so ethical approval was perceived redundant. We presume no legal issues/implications.
Results
Out of 192 human skulls examined in this study, only 2 skulls showed atlantooccipital fusion. They are shown in [Table/Fig-2a,b].
a) Skull showing left side incomplete atlantooccipital fusion; b) Skull showing complete atlantooccipital fusion.
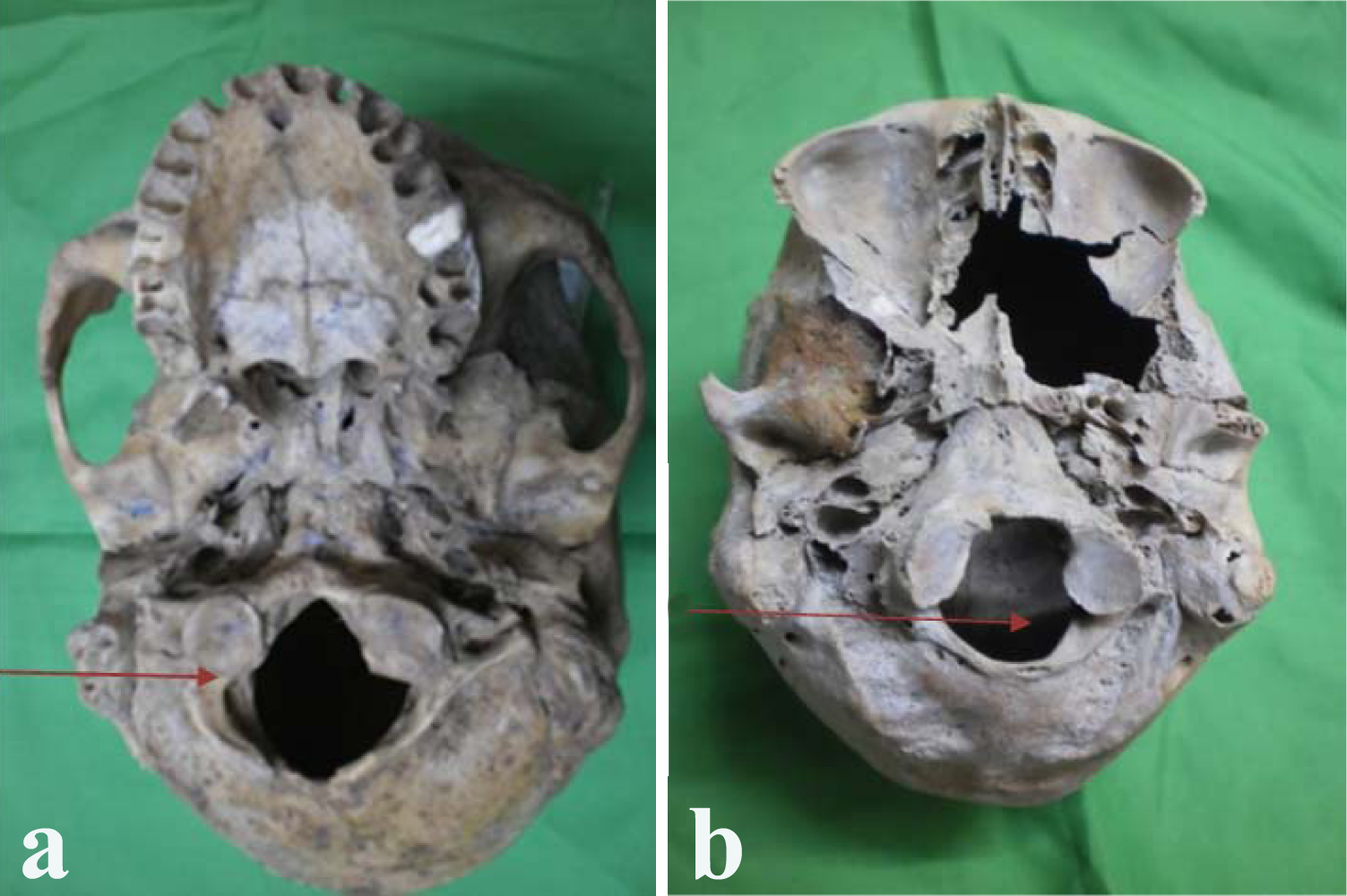
[Table/Fig-2a] shows left sided incomplete atlantooccipital fusion. Anterior arch, right transverse process and the right part of posterior arch of atlas are completely fused to the adjoining part of occipital bone. The left transverse process of atlas has a prominent posterior tubercle with deficient anterior costal element so an incomplete foramen transversarium is present. Both articular processes of atlas and occipital condyles are fused. The anteroposterior and transverse diameters of fused left occipital condyle and left superior articular process of atlas are more than that of the right side. Little asymmetry of foramen magnum and right inclination of skull by about 6 mm are observed. The posterior tubercle and right half of posterior arch of atlas near the midline are missing. The cranial index is 69.5%, suggesting a dolichocephalic skull. The hypoglossal and condylar canals on both sides are normal.
[Table/Fig-2b] shows complete atlantooccipital fusion. The skull has a complete fusion of the anterior and posterior arches and transverse processes of atlas with the adjoining part of occipital bone. Articular process of atlas and corresponding occipital condyle on both the sides are completely fused. Anteroposterior and transverse diameters of left fused articular facet are more than that of right side. Reduction in the size and asymmetry in shape of foramen magnum are seen. The cranial index is 70.5% suggesting a dolichocephalic skull. Hypoglossal and condylar canals on both sides are normal. No any inclination is observed.
Observations and findings of this study are correlated embryologically and clinically with the results and claims of previous studies and literature, and accordingly the conclusions are drawn.
Discussion
As per previous studies, the incidence of atlantooccipital fusion ranges from 0.14% to 0.75% of the population, with both sexes being equally affected [7]. However, the current study reveals higher prevalence i.e., 1.04% in South Asian population predominantly in Central India. Out of 192 skulls of both genders only two skulls presented occipitalization of atlas, where the first skull exhibited partial or hemifusion whereas, the second skull showed complete atlantooccipital fusion. Because of non availability of literature about gender differences among these cases, the gender predominance in this study could not be correlated.
Atlantooccipital fusion was first described by Rokitansky in 1844 and demonstrated roentgenographically by Schuller in 1911 [8]. The same authors also reported that the incidence of atlantooccipital fusion varies from 0.5%-1.0% in Caucasians. Furthermore, Murlimanju et al., in a recent study showed that the occipital bone may fail in some centres of ossification [9].
Disassociated occipital condyles are called a proatlas, because in some lower vertebrates the cranial half of the first cervical sclerotome remains as a separate bone called as proatlas between the occiput and first cervical vertebra, but in human the proatlas fuses with the occipital condyles and the tip of the dens of axis vertebra [10]. The caudal half of the first cervical sclerotome forms the lateral masses and anterior and posterior arches of atlas vertebra. The body of the first cervical vertebra regresses and forms the major part of dens. The first cervical vertebra is formed by the caudal half of fourth occipital somite and cranial half of first cervical somite [10]. The body, posterior arch and transverse process of the second cervical vertebra are derived from the second cervical sclerotome. If the normal segmentations do not occur then it results in atlantooccipital fusion. Embryologically, it seems that either improper division of cranial part of paraxial mesoderm during development of somites especially caudal occipital and cranial cervical sclerotomes or abnormal fusion between divisions of these sclerotome may lead to occipitalization of atlas.
The atlas is commonly ossified from three centres. One appears in each lateral mass at about the seventh week of intrauterine life extending into the posterior arch where they unite between the third and fourth year of life [11]. Two ossification centres one just posterior to lateral mass and other for transverse process appear and meet in the middle posteriorly usually by fourth year of life. The anterior part of the atlas ossifies by two closely lying ossification centres appearing at about six month of age and united within few months of their appearance. Then ossification proceeds posterolaterally along both anterior arch and fuses with the lateral masses during fifth year of life. At birth, the anterior arch is fibrocartilaginous, and a separate centre appears about the end of the first year, which unites with the lateral masses between the sixth and eighth year. Occasionally the anterior arch is formed by the extension and ultimate union of centres in the lateral masses and sometimes from two lateral centres in the arch itself [11]. The failure of fusion at midline posteriorly or restriction of spread of ossification posterolaterally along the anterior arch may result into anomalous atlas and then its failure of separation may result into the occipitalization of atlas of varying degree. Frequently bony spurs arise from the anterior and posterior margins of the groove for the vertebral artery. They are sometimes referred to as ponticles and they occasionally convert the groove into foramen. Rarely the atlas may be wholly or partially assimilated into the occiput [11].
Clinical manifestations associated with atlantooccipital fusion are mainly attributed to the ligamentous laxity of the transverse ligament in relation to the odontoid process. The flexion and extension movements of neck lead to the compression of spinal cord. The chances of regeneration of the central nervous system decreases with increasing age and repeated injuries to the nerves from the odontoid may result in the neurological symptoms. Atlantooccipital fusion is associated with narrowing of foramen magnum, compression of spinal cord or brain stem [12]. Serious clinical manifestation such as myopathy, limitations of neck movements, muscular weakness and atrophy and sensory loss may be associated [5,13]. Patients with atlantooccipital fusion present with headache, neck pain, numbness, pain in the limbs, weakness, abnormal head posture, torticollis, restricted neck movements and may lead to sudden death. Spinal cord compression always occurs when the sagittal spinal canal diameter behind the odontoid process is less than or equal to 14 mm. Cord compression is possible when the sagittal canal diameter is between 15 mm-17 mm and almost never occurs at a distance of 18 mm or more.
Some eminent scientists have expressed their valuable opinions according to their studies, like occipitalization of atlas may remain asymptomatic if the odontoid process is below the level of foramen magnum. Normally, the odontoid process should not cross the level of McRae and Barnon line drawn across the foramen magnum. The anterior atlantooccipital fusion between the rim of the foramen magnum and the arch of atlas causes development of intermittent pressure symptoms depending on the position and movement of head. Atlantooccipital fusion reduces the foramen magnum dimension leading to neurological complications due to compression of spinal cord [14].
In our study, as the anteroposterior diameters of foramen magnum behind the odontoid process after articulation with axis were 16 mm and 13 mm in Skull-1 and Skull-2 respectively, therefore in both these cases, the chances of nervous tissue compression and clinical manifestations would have been more. We accepted that although the atlantooccipital fusion is rare and uncommon developmental abnormality but in these cases, clinical manifestations by associated reduction and change in dimensions of foramen magnum, restricted neck movements and symptoms and signs due to neurological and vascular compression cannot be denied and so these cases are of clinically important to physicians and surgeons for the diagnostic and therapeutic purposes.
The knowledge of assimilation may be of great importance to neurosurgeon, orthopaedician and clinician dealing with the neurological symptoms and signs due to compression of spinal cord or pathogenesis of upper cervical vertebrae. It is also of significance to anaesthetic dealing with the cause of failure of cisternal puncture. Radiologist dealing with craniocervical junction and physiotherapist managing neck pain must also be aware of this situation. The transverse process of atlas is an important landmark for a clinician and when it is inclined and assimilated to occipital bone; there may be uncertainty in reaching various neighboring structures.
The literature review showed association of complete or partial atlantooccipital fusion with reduction in the dimensions and abnormal shape of foramen magnum leading to neighboring neurovascular compression and appearance of its clinical manifestation usually during second decade of life or little later. Though onset of manifestation is mild to moderate but sometimes it may lead to sudden unexpected death and serious consequences of upper cervical manipulation with this osseous anomaly reflect the importance and need for a thorough clinical assessment and evaluation.
Conclusion
We conclude that the prevalence of atlantooccipital fusion including complete and incomplete fusion was 1.04%, which is higher than the proclaimed prevalence rate. In accordance with the fact that the atlantooccipital fusion represents a synostosis between the atlas and the occipital bone due to developmental abnormal segmentation of cranial part of paraxial mesoderm and abnormal fusion between segments of caudal occipital and cranial cervical sclerotomes, we would like to thereby assert that the fusion associated with the reduction in dimensions of foramen magnum (reduction also seen in our study) is definitely significant for diagnostic and therapeutic purposes to clinicians.
[1]. Carmina R, Julio P, Is Chiari type I malformation a reason for chronic daily headache?Current Pain and Headache Reports 2007 11(1):53-55. [Google Scholar]
[2]. Kassim NM, Latiff AA, Das S, Ghafar NA, Suhaimi FH, Othman F, Atlantooccipital fusion: an osteological study with clinical implicationsBratislavske Lekarske Listy 2010 111(10):562-65. [Google Scholar]
[3]. Soni P, Sharma V, Sengupta J, Cervical vertebrae anomalies-incidental findings on lateral cephalogramsAngle Orthod 2008 78:176-80. [Google Scholar]
[4]. Monika L, Sanjay P, Anupama M, Kullar JS, Occipitalization of atlas: A case report with its ontogenic basis and review of literatureCurrent Trends in Diagnosis and Treatment 2017 1(1):34-37. [Google Scholar]
[5]. Nagashima H, Morio Y, Teshima R, No neurological involvement for more than 40 years in Klippel-Feil syndrome with severe hypermobility of the upper cervical spineArchives of Orthopaedic Trauma Surgery 2001 121(1-2):99-101. [Google Scholar]
[6]. Kang RK, Young ML, Young ZK, Yong WC, Joon SK, Kyu HK, Cervical myelopathy secondary to atlanto-occipital assimilation: the usefulness of the simple decompressive surgeryKorean J Spine 2013 10(3):189-91. [Google Scholar]
[7]. Guebert GM, Yochum TR, Rowe LJ, Congenital anomalies and normal skeleton variantsEssentials of Skeletal Radiology 1987 BaltimoreWilliams & Wilkins:197-306. [Google Scholar]
[8]. AL-Motabagani MA, Surendra M, Total occipitalization of the atlasAnatomical Science International 2006 81(3):173-80. [Google Scholar]
[9]. Murlimanju BV, Prabhu LV, Paul MT, Pai MM, Krishnamurthy A, Rai A, Variant morphogenesis of squamous part of occipital bone in human skullsJournal of Morphological Sciences 2010 27(3-4):139-41. [Google Scholar]
[10]. Susan Standring. Gray’s AnatomyDevelopment of sclerotomes 2013 14th edChurchill Livingstone:770 [Google Scholar]
[11]. Susan Standring. Gray’s AnatomyDevelopment of sclerotomes 2013 14th edChurchill Livingstone:720 [Google Scholar]
[12]. Gholve PA, Hosalkar HS, Ricchetti ET, Pollock AN, Dormans JP, Drummond DS, Occipitalization of the atlas in children, Morphologic classification, associations, and clinical relevanceJ Bone Joint Surgery Am 2007 89:571-78. [Google Scholar]
[13]. Martellacci S, Ben SD, Mejean N, Sautreaux JL, Krause D, A case of foramen magnum syndrome caused by atlanto-occipital assimilation with intracranial fibrosisSurg Radio Anat 2008 30:149-52. [Google Scholar]
[14]. Jayanthi V, Kulkarni R, Kulkarni RN, Atlantooccipital fusion - report of two casesJournal of the Anatomical Society of India 2003 52:71-73. [Google Scholar]