Since, there are no studies that used both ultrasonic excitation with halogen light as an additional activation method, the present study was done to assess the influence of these as externally applied command set methods on microleakage of Type IX glass ionomer cement.
Materials and Methods
The present in vitro study was done in the Department of Paedodontics and Preventive dentistry, Rajah Muthaih Dental college and Hospital, Annamalai University, Chidambaram, Tamil Nadu, India. Forty human premolars free of caries or any other defects and extracted for orthodontic reasons were chosen for the study. All specimens were cleaned and stored in distilled water till use. Standard Class V cavities were prepared on the facial surface of all the teeth 1.5 mm occlusally from the cemento-enamel junction with an ISO (No.010) straight fissure bur followed by (No.014) inverted cone bur in a high speed airotor hand piece with water spray. Cavity depth was standardized at 3 mm width X 2 mm depth X 2 mm height dimensions measured by bur markings and Williams periodontal probe. The specimens were allocated into four groups (n=10 for each group) by simple random sample method.
The teeth in all four groups were conditioned with GC dentin conditioner (10% polyacrylic acid) using an applicator tip for 20 seconds, thoroughly rinsed with water and air dried. Type IX glass ionomer were selected for this study because they are mostly used for paediatric restorations. GC Gold Label Type IX (GC Corporation, Tokyo, Japan) glass ionomer cement was mixed according to manufacturer’s instructions and the prepared cavities were restored with it. In all four groups, finger press technique was applied for 10 seconds after placing glass ionomer into the cavity and excess cement was removed with hand instruments.
Group 1: GC Fuji varnish was applied over the restoration using an applicator tip immediately after setting of GIC. (Control group).
Group 2: After placing GIC, specimens were irradiated with a halogen light curing unit (Dentamerica, Litex 680 A) operating at 500 mW/cm2 for 60 seconds [Table/Fig-1]. GC Fuji varnish was applied over the restorations using an applicator tip immediately after setting of GIC.
Halogen light irradiation of the specimen.
Ultrasonic scaler excitation of the sample.

Samples after application of nail varnish.

Group 3: After placing GIC, a broad ultrasonic scaler tip driven by a ultrasonic hand scaler SATELEC (MERIGNAC cedex France) was kept on the clear celluloid strip at the middle of the cement surface of each sample [Table/Fig-2] for 40 seconds and finger press technique was done for 15 seconds. The scaler was set at 30 kHz, power set at 2 (medium). GC Fuji varnish was applied immediately after setting of GIC.
Group 4: After restoring with GIC, a broad ultrasonic scaler tip driven by a ultrasonic scaler SATELEC (MERIGNAC cedex France) was kept on the clear celluloid strip at the middle of the cement surface of each tooth for 40 seconds, equipment set at 30 kHz and power set at 2 (medium) and this was followed by immediate irradiation by halogen light curing unit (Dentamerica, Litex 680 A) operating at 500 mW/cm2 for 60 seconds. GC Fuji varnish was applied over the restorations immediately after setting.
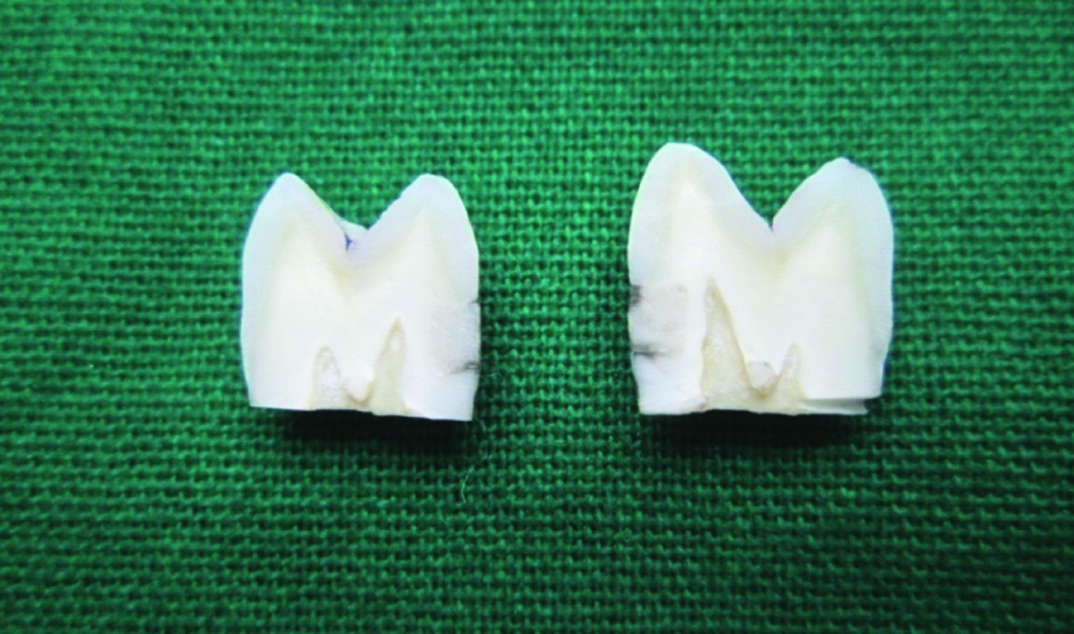
The teeth were then kept in distilled water for 24 hours. The teeth were exposed to 1500 thermocycles at 12°C ± 2 and 60°C ± 2 with one minute dwell time in each bath to simulate oral environment. The samples were then painted with two layers of nail varnish [Table/Fig-3], 1 mm short of the restorative margins and sticky wax used to seal root apices. The teeth were then exposed to a dye solution containing 50% silver nitrate for four hours and then stored in a developing solution (Kodak Ind. Ltd.,) for four hours under 200 watt bulb. The light source was placed as close as possible to the specimens. The teeth were washed under running water for five minutes after dye exposure and with a scalpel, nail varnish was removed. Using a diamond disc under water spray the teeth were sectioned buccolingually through the centre of the restoration creating two specimens with tooth interface exposure from cavosurface margin to the pulpal wall. The degree of microleakage of both halves of the sectioned tooth [Table/Fig-4] were analysed using a stereomicroscope (Model No: XTL-3400 E, China) at 10X magnification connected to a digital video camera (Samsung). The portion showing maximum degree of dye penetration was recorded for microleakage grading [Table/Fig-5,6,7,8 and 9].
Khera S and Chan K criteria [2] were used to record the degree of marginal microleakage [Table/Fig-5,6,7,8 and 9].
Buccolingual section of the tooth.
Score 0-No marginal leakage.
Score 1-Less than and upto one half of the depth of the cavity preparation was penetrated by the dye.
Score 2-More than one half of the depth of the cavity preparation was penetrated by the dye but not upto the junction of the axial and occlusal or cervical wall.
Score 3-Dye penetration was upto the junction of axial and occlusal or cervical wall but did not include the axial wall.
Score 4-Dye penetration included the axial wall.
Statistical Analysis
The results were tabulated and statistically analysed by One-way ANOVA test to evaluate if significant statistical difference exist in microleakage among four groups. A post-hoc Tukey’s comparison test were done to determine if any statistically significant difference is noticed between the groups.
Results
Based on data available in [Table/Fig-10] ultrasonic group (Group 3) showed the highest microleakage scores with scores ranging from 1 to 4. The group where ultrasonic activation was followed by halogen irradiation (Group 4) showed the second highest microleakage scores ranging from 1 to 4. The control group (Group 1) showed the second least microleakage scores ranging from 1 to 3. The halogen group (Group 2) showed the least microleakage scores ranging from 1 to 2.
Microleakage scores and One-Way ANOVA test for study groups.
| Groups | Microleakage scores | Mean (mm) | Std. deviation | F-value | p-value |
|---|
| Control Group I | 1 | 0 | 0 | 0 | 1 | 1 | 0 | 3 | 1 | 2 | 0.90 | 0.99 | 12.53 | 0.001* |
| Halogen Group II | 0 | 1 | 0 | 0 | 0 | 2 | 1 | 0 | 0 | 1 | 0.50 | 0.71 |
| Ultrasonic Group III | 3 | 2 | 1 | 4 | 2 | 4 | 4 | 3 | 4 | 3 | 3.00 | 1.05 |
| US+H Group IV | 2 | 1 | 1 | 3 | 4 | 2 | 1 | 1 | 4 | 4 | 2.30 | 1.34 |
| Total | | | | | | | | | | | 1.68 | 1.44 |
Significant, US+H: Ultrasonic + Halogen
The halogen group recorded the lowest mean microleakage scores followed by control group, ultrasonic + halogen group and ultrasonic group [Table/Fig-10]. Control group showed no significant statistical difference with halogen irradiation group (p>0.05). Ultrasonic activation group showed no significant statistical difference with ultrasonic activation plus halogen group (p>0.05). Control group and halogen group showed significant statistical difference when compared with ultrasonic activation alone and combined ultrasonic activation plus halogen irradiation group (p<0.05) [Table/Fig-11].
Multiple Comparison of microleakage among different groups by I Tukey’s test.
| Groups | Comparison of groups | p-value |
|---|
| Group 1-Control groupGroup 2- Halogen groupGroup 3-Ultrasonic groupGroup 4-Ultrasonic+halogen group | 1 versus 21 versus 31 versus 4 | 0.820.001*0.001* |
| 2 versus 32 versus 4 | 0.001*0.001* |
| 3 versus 4 | 0.45 |
Significant
Discussion
Traditional glass ionomers are very sensitive to water uptake in the first stage of setting which occurs in first 10 minutes. But in second phase which is slow and a long term continuous acid base reaction, it is sensitive to dehydration [9,10]. The acid base reaction is between polyacrylic acid and calcium/aluminium ions from the glass in the maturing stages. If the matrix is exposed to water during first 15 minutes of setting, a superficial surface softening can occur by the inhibition of reaction in the superficial layer of glass ionomer cement [11]. During initial setting phase, integrity problem is caused by water which is loosely bound [9]. The initial exposure of water causes leaching of ions, weakening and swelling but loss of water causes cracking and shrinkage [10]. The clinical performance and physical properties are improved by reducing the period of acid-base setting reaction. Glass ionomer setting is influenced by various external factors like mixing time, temperature and pressure [12]. To increase mechanical strength and to reduce moisture sensitivity in early phases of acid-base setting reaction, various attempts have been done [13]. When dealing with paediatric patients, decrease of setting reaction time is a crucial factor and an added advantage to reduce moisture contamination under clinical condition and it reduces clinical chair time [14]. The mean shear bond strength of glass ionomer to dentine in primary teeth can be compromised by salivary contamination [15]. In paediatric dentistry, external energy source such as light or ultrasonic excitation can be used as a command set method for faster setting of conventional glass ionomers which helps in enhancing surface characteristics at early stage [16]. The surface exposure from a light curing unit or ultrasonic scaler instrument can enhance surface hardness during initial stage of setting reaction of glass ionomers [17]. The surface microhardness increased during the critical 60 minutes when glass ionomer has to be prevented from water contamination when light was used during setting [18]. The properties of glass ionomer are not altered by the use of a halogen light curing unit used as a command set but ultrasonic use can affect its marginal seal [19]. Ultrasound excitatory waves applied during early setting reaction when used as a command set method adds kinetic energy from ultrasound device to the material and this can enhance the rate of setting reaction due to rise in temperature [12]. According to one study, mechanical excitation of scaler tip itself improved the setting rate of glass ionomers and is less influenced by rise of temperature [13]. Higher temperature increase on the material is more provoked by the halogen light curing unit. The mechanical characteristics of glass ionomer like microhardness can be increased by heat application [20]. Earlier studies suggested that when using ultrasonic excitation, if the scaler tip temperature is high it results in liquid evaporation and increases powder to liquid ratio culminating in high strength of the material [12,21]. On the other hand, it can be expected that there occurs a reduction in volume, size and number of voids or porosities which is present in the cement intrinsically, due to high frequency vibration of the material caused by the mechanical movement of the ultrasonic tip allowing better and more efficient mixing of particles and polyalkenoic acid chains resulting in an increased total reactive surface which improves the setting time [22]. The early weakness of glass ionomer restoration can be decreased thus enhancing surface hardening by ultrasound treatment [16]. Towler M et al., proposed that ultrasound causes breaking down of glass particles which increases powder surface area which contributes to acceleration of the reaction [14]. The bonding to the tooth surface is enhanced by ultrasonic excitation of glass ionomer [12].
In our study, the least marginal leakage of enamel adjacent to the Type IX glass ionomer was for the halogen group. This is in accordance with findings of Gorseta K et al., who concluded that heating the glass ionomer cement by external heat source during setting decreased the vulnerability to microleakage and improves the wall adaptation to enamel [23]. Due to elevated temperature, halogen light causes change in the molecular kinetic energy which leads to molecular rearrangement of the material during setting. Even a rise of temperature of 2°C-3°C on the surface of the filling, a better adhesion of the material and a more stable zone of ionic exchange is brought about by this molecular rearrangement [23]. Kristina G et al., concluded that heating of glass ionomer improved the properties of glass ionomer restoration and increases shear bond strength to enamel [24].
The control group showed more microleakage than halogen group because highly viscous glass ionomers do not allow proper wetting of the tooth surface preventing formation of a good seal between tooth restoration interfaces resulting in microleakage [25]. Singla T et al., found that GC Fuji IX glass ionomer showed maximum microleakage when compared to previously exsisting glass ionomer restorative materials [26].
The highest marginal microleakage of enamel adjacent to the Type IX glass ionomer was noticed for the ultrasonic group in this study. Guglielmi CA et al., from their results concluded that ultrasonic activation showed more microleakage compared to control group and may interfere with adaptation of conventional glass ionomer cement but halogen light curing did not interfere with microleakage [19]. In the setting stages of glass ionomer the viscosity increases and reduces the flow of the cement especially in case of highly viscous glass ionomer cement during the formation of polycarboxylate network. When using ultrasound device, the acid-base setting reaction period is reduced which can accelerate the polycarboxylate network formation and this stops the cement flow before the cavity is completely filled. Therefore, mechanical acceleration of the curing process may affect this property because the chemical adhesive capacity of glass ionomer is related to initial reaction of jellification [16]. Currently, there are only few studies that use heat and ultrasound as a command set method for glass ionomer. Hence, it is difficult to compare the results obtained from this study. In our study, even though ultrasonic activation +halogen irradiation group showed less microleakage than ultrasonic group alone, the combination group was not very favourable in reducing microleakage because the inter comparison results between both the groups were statistically not significant with respect to dye penetration scores. Further research is needed to study the exact mechanism of command set method and their effects on microleakage around glass ionomer restorations.
Limitation
It was not possible to simulate the exact oral environment as this was an in vitro study. The sample size could have been increased. Only a single parameter, using dye penetration method to estimate microleakage was used to assess the marginal integrity. In clinical situation, the effect of temperature for command set, needs to be determined and its effects on surrounding pulp and soft tissues has to be detailed.
Conclusion
Within the limitations of the present study, we conclude that the microleakage of the enamel adjacent to GC Type IX glass ionomer restorations is less when using halogen light to accelerate the setting reaction of the glass ionomer. Halogen light can be used as command set modality for Type IX glass ionomer and a good alternative in paediatric dentistry. Since, higher micro leakage was noticed between the restorative material and the adjacent enamel after using an ultrasonic scaler it is not recommended as a command set method even though it improves the physical and mechanical properties of the cement.
*Significant, US+H: Ultrasonic + Halogen
*Significant