Atypical Imaging Features of a Simple Intramuscular Lipoma
Umamageswari Amirthalingam1
1 Assistant Professor, Department of Radiodiagnosis, Indira Gandhi Medical College and Research Institute, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Umamageswari Amirthalingam, 26B, Vaigai Street, Vasanth Nagar, Muthialpet, Puducherry-605003, India.
E-mail: dr_amirthauma@yahoo.co.in
Lipoma is a benign tumour of mesenchymal tissue which closely resembles normal fat even histologically but for its biochemical and ultrastructural differences. Simple lipoma presents as a mass which resembles fat on all the imaging modalities. Atypical lipoma, lipoma variants and liposarcoma show specific imaging features. We report this case due to the varied imaging appearance of a simple lipoma. A 52-year-old lady presented with history of swelling along the anterior aspect of thigh. Sonography, CT and MRI had done which revealed an atypical lipoma; however excision biopsy proved to be a simple lipoma.
Lipomatous soft tissue tumour, Well differentiated liposarcoma
Case Report
A 52-year-old lady presented with history of swelling along the anterior aspect of right thigh for the past three years. There was no history of pain or sudden increase in size of the swelling. There was no history of previous treatment for the same complaint. Clinically, the swelling appeared to be along the deep intramuscular plane, measured about 20 cm in length and 5 cm in width, soft on palpation, with no bruit, leading to the clinical diagnosis of a probable benign soft tissue tumour.
Ultrasonogram done with Philips HD7XE, 3-5 MHz curvilinear and 6-12 MHz linear transducer showed an echogenic intramuscular mass lesion along the anterior and medial aspect of right mid thigh. No cystic changes or calcification was seen. Imaging differential diagnosis of lipoma or lipomatosis was made.
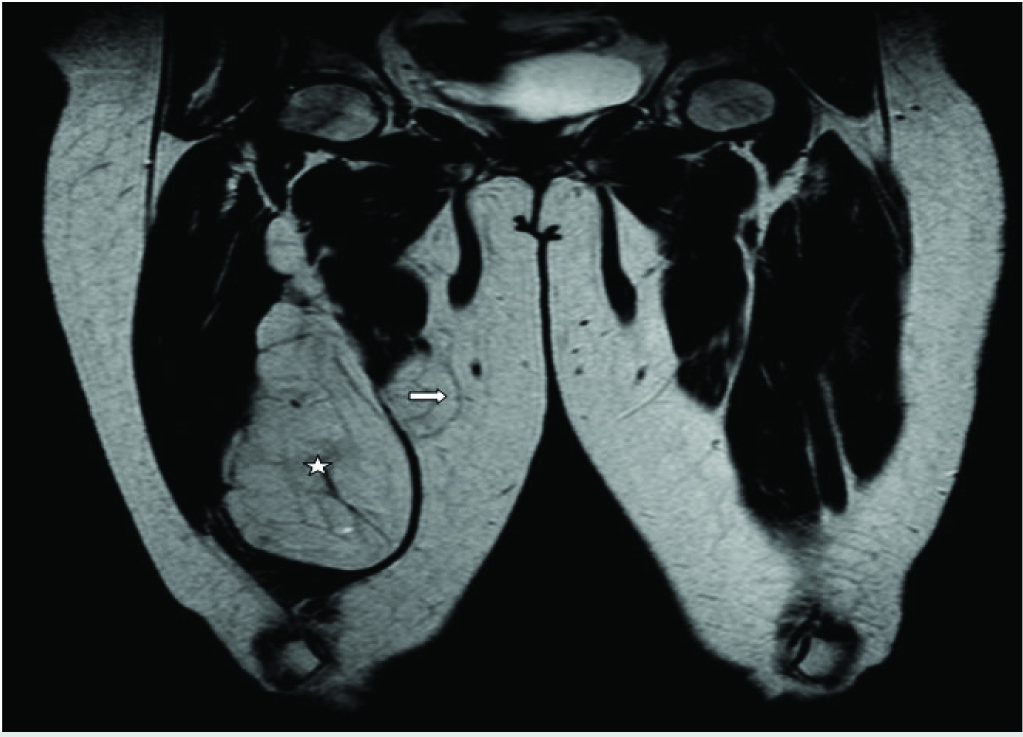
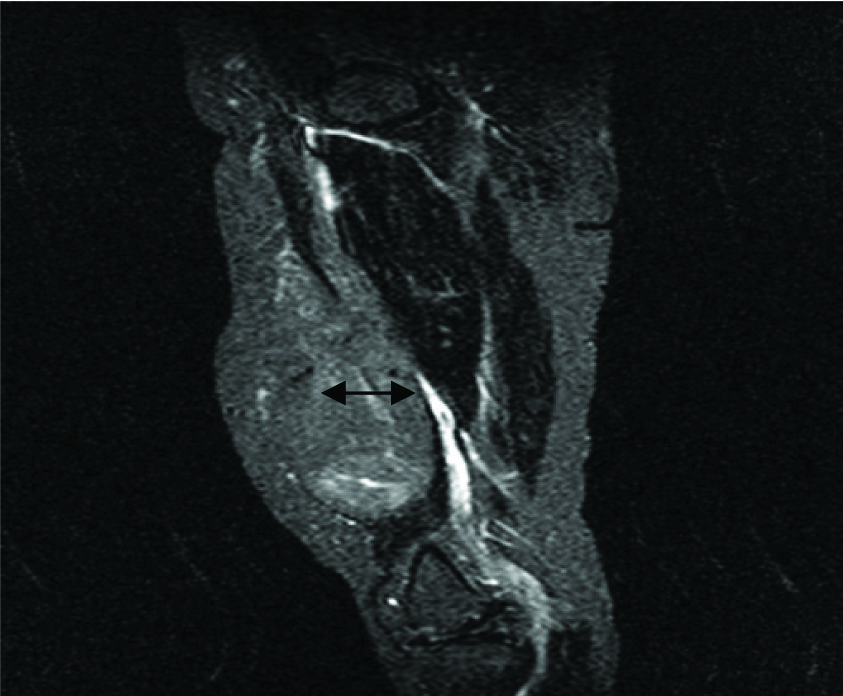
MRI (Philips Intera 1.5T) plain and Gadolinium enhanced contrast showed a 23.0 x 6.8 x 6.6 cm (cc x tr x ap) sized lobulated encapsulated lesion along the medial compartment of right thigh, which was predominantly isointense to the subcutaneous fat [Table/Fig-1], which also showed doubtful extracapsular extension; however few hyperintensities were noted on T2 fat saturated sequence [Table/Fig-2]. The lesion appeared to be intramuscular involving the adductor magnus and brevis with extension along the intermuscular plane, also extending to the subcutaneous plane.
T2 weighted coronal image of both thighs, shows a lobulated intramuscular lesion ☆ along the right thigh, isointense to subcutaneous fat. (➡) denotes the doubtful extracapsular extension.
T2 weighted sagittal image with fat saturation, showing hyperintense foci ( ).
).
Post Gadolinium T1 weighted sagittal image with fat saturation showing scattered and multifocal contrast enhancement ( ).
).
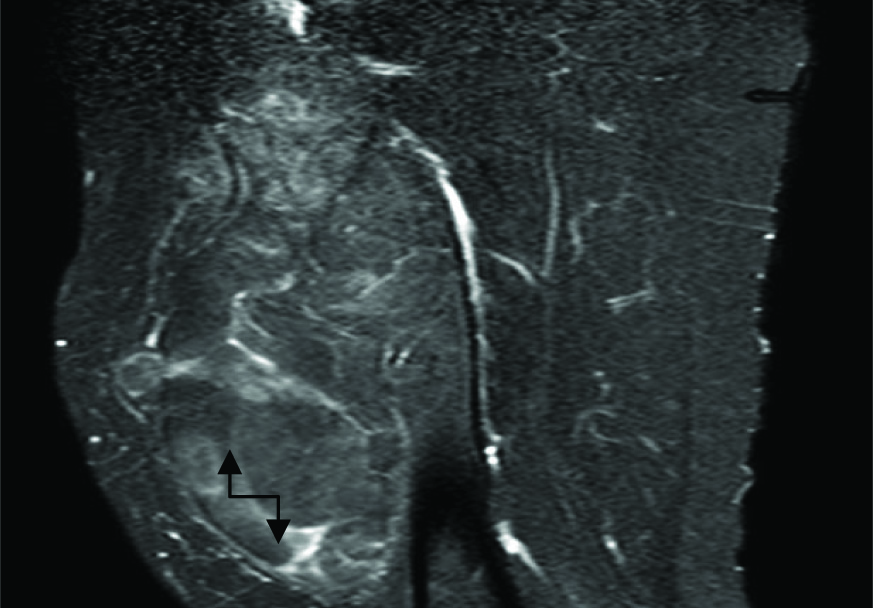
Superiorly the lesion extended upto the inguinal region, to terminate inferiorly just above (3.5 cm) the patella. Medial extension noted upto the gracilis. The lesion was abutting the superficial femoral vessels, causing mass effect over the superficial femoral vein. Multiple septae of about 1 mm thickness were noted within. Post contrast images showed multifocal scattered and septal enhancement [Table/Fig-3]. No intralesional nodularity was made out.
CT (Philips MX 16) plain study showed a well-defined encapsulated lesion with attenuation of -85 to -115 HU, suggestive of a lipomatous lesion. Extensions were seen similar to that in MRI. No underlying bony erosion or calcifications.
To summarize, a lobulated encapsulated fatty lesion along the intra and intermuscular plane with post contrast enhancement, enhancing septae and doubtful extracapsular extension; suggesting atypical lipoma/well differentiated liposarcoma.
Fine Needle Aspiration Cytology (FNAC) showed clumps of adipocytes, suggesting a benign lipogenic tumour.
Intraoperatively, the lesion appeared intramuscular and few out pouching and lobulations were observed. However, the lesion remained entirely intracapsular and was excised in toto.
Excision biopsy showed yellowish soft tissue mass on gross pathology and mature adipose tissue separated by fibrous septae, with the diagnosis of lipoma. The patient was followed up for a period of six months, during which there was no recurrence.
Discussion
The World Health Organization’s (WHO) committee for classification of soft tissue tumours in 2002 has classified the benign lipomatous lesions into lipoma, lipomatosis, lipomatosis of nerve, lipoblastoma/ lipoblastomatosis, angiolipoma, myolipoma of soft tissue, chondroid lipoma, spindle cell/pleomorphic lipoma, and hibernoma [1].
Lipoma is a benign tumour of mature adipocytes and represents the most common soft tissue tumour [2]. It occurs in all age groups, with age range between 40-60 years [3]. Depending on the location, lipomas can be classified into superficial and deep and parosteal. The deep seated lipomas may be intramuscular or intermuscular.
Simple lipomas present as painless masses; neural compression is associated with pain. On gross pathology simple lipomas are yellowish greasy masses; which on microscopy show lobules of mature adipocytes. On conventional radiography large lipomas demonstrate radiolucency. On sonography they appear as echogenic masses without posterior enhancement; presence of septae, show heterogeneity. CT and MR imaging reveal simple lipomas as homogenous fatty masses, containing few thin septae (<2 mm); show complete fat saturation. Intramuscular lesion demonstrates muscle fibers. No contrast material enhancement seen at CT or MR imaging except of the fibrous capsule [4].
Chondroid lipoma, osteolipoma, hibernoma, lipoleiomyoma, angiolipoma and infarcted lipoma are included under benign lipoma variants [5]. These lesions are neither simple lipomas nor well-differentiated liposarcomas; contain varying amounts of cartilaginous, osteoid, smooth muscle and vascular elements.
Well differentiated liposarcoma, known synonymously as atypical lipoma, atypical lipomatous tumours and adipocytic liposarcomas [6]. The most common locations include the extremities and retroperitoneum. Bony erosions may be associated with higher grade lesions. On CT and MRI, the lesions show lobulations, fat density, nodularities, thickened (>2 mm) nodular septae, non adipose masses, prominent high T2 signal foci and areas of enhancement.
Conclusion
Our case showed few atypical features such as enhancing septae, enhancing areas and doubtful extracapsular extension. However non adipose masses and nodularity were absent. A mere presence of a few atypical imaging features does not confirm the diagnosis of liposarcoma; which however needs histopathological correlation.
[1]. Christopher D, Unni K, Mertens F, Adipocytic tumors WHO Classification of tumors. Pathology and genetics:tumors of soft tissue and boneIARC 2002 :19-46. [Google Scholar]
[2]. Kaeser MA, Smith LW, Kettner NW, Case report of an intermuscular lipoma:presentation, pathophysiology, differential diagnosisJ Chiropr Med 2010 9(3):127-31. [Google Scholar]
[3]. Christopher D, Unni K, Mertens F, WHO Classification of tumorsPathology and genetics:tumors of soft tissue and bone. International Agency for Research on Cancer, IARC 2002 19:46 [Google Scholar]
[4]. Kransdorf MJ, Bancraft LW, Peterson JJ, Murphey MD, Foster WC, Temple HT, Imaging of fatty tumors:distinction of lipoma and well-differentiated liposarcomaRadiology 2002 224(1):99-104. [Google Scholar]
[5]. Gaskin CM, Helms CA, Lipomas, lipoma variants, and well-differentiated liposarcomas (atypical lipomas):results of MRI evaluations of 126 consecutive fatty massesAJR Am J Roentgenol 2004 182(3):733-39. [Google Scholar]
[6]. Mavrogenis AF, Papagelopoulos PJ, Well-differentiated liposarcomaAtlas Genet Cytogenet Oncol Haematol 2013 17(8):579-82. [Google Scholar]