Materials and Methods
Ethical approval: The study was approved by Institute Ethical Committee of Banaras Hindu University, Varanasi.
A total of 126 cases were included for collection of blood, stool and urine, out of them 90 patients were suffering from acute typhoid fever and 36 were chronic typhoid carriers. About 47 (37.3%) S. Typhi isolates were included in the present prospective study. The inclusion criteria for the collection of clinical specimens was having clinical history of acute typhoid fever, confirmed for the presence of S. Typhi by Widal test having titre ≥1:160 for TO/TH and apparently healthy chronic typhoid carriers were included on the basis of high titer against the Vi-antigen (≥1:160) by Indirect Haemagglutination Assay (IHA). These strains were isolated during February 2011 to March 2013 in the University Hospital of Banaras Hindu University, Varanasi. Identification and characterisation of the all isolates were done by phenotypic, biochemical and serological agglutination tests using different antisera i.e., poly O, poly H, factor O9, Hd and Vi-antisera. We have further confirmed these isolates by Polymerase Chain Reaction (PCR) amplification and sequencing of 16S rDNA [8] and specific flagellin (fliC) gene sequences of S. Typhi. The isolates were then subjected to antimicrobial susceptibility testing by modified Kirby-Bauer disc diffusion method following the recommendation of Clinical and Laboratory Standards Institutes (CLSI) guidelines [9]. Escherichia coli American Type Culture Collection (ATCC 25992) strain was used as standard strain for the antimicrobial susceptibility test. The drugs tested were nalidixic acid (NA, 30 µg), amoxicillin (AMC, 30 µg), cephalexin (CP, 30 µg), cefuroxime (CXM, 30 µg), ciprofloxacin (CIP, 5 µg), ceftriaxone (CTR, 30 µg), cefoxitin (CX, 30 µg), co-trimoxazole (COT, 25 µg), imipenem (I, 10 µg), chloramphenicol (C, 30 µg) and azithromycin (AZM, 15 µg). The antibiotics discs were procured from Hi-Media, Mumbai, India. The MIC of cefuroxime, ceftriaxone and azithromycin was determined for by agar dilution method [10]. When MIC values were ≤1 µg/ml for ceftriaxone, and ≤4 µg/ml for cefuroxime, the strains were considered as sensitive, while isolates with MIC values of ≥4 and ≥32 µg/mL for ceftriaxone, and cefuroxime respectively were considered as resistant. There is no Clinical and Laboratory Standards Institutes (CLSI) guideline for MIC interpretation against azithromycin for Salmonella Typhi. Therefore, to determine the azithromycin susceptibility and resistance, we used breakpoint criteria recommended by National Committee for Clinical Laboratory Standards (NCCLS) for azithromycin [11,12]. The isolates having zone diameter ≤2 µg/ml were designated as sensitive and those having zone diameter ≥8 µg/ml as resistant [9].
Results
Antibiotic Susceptibility Testing by Disc Diffusion Method
Of the 47 S. Typhi isolates, only 1 (2.1%) was observed to be resistant against chloramphenicol. Nalidixic acid was found to face the highest resistance 76.6% (36/47). The second highest resistance was seen against amoxicillin 38.3% (18/47) followed by cephalexin 27.6% (13/47), cefuroxime 27.6% (13/47), ciprofloxacin 25.5% (12/47), ceftriaxone 23.4% (11/47), cefoxitin 21.3% (10/47), azithromycin 21.3% (10/47), co-trimoxazole 19.1% (9/47), imipenem 8.5% (4/47) of the isolates [Table/Fig-1,2].
Drug resistance pattern of Salmonella Typhi over three decades at this centre. (n=47) [5,13].
| Antimicrobial agents | Nath G et al.,2000 | Pratap CB et al.,2012 | This study |
|---|
| 1979-1989 n=44(%) | 1990-1998 n=96(%) | 1998-1999 n=22 (%) | 2009-2010 n=36(%) | 2011-2013 n=47(%) |
|---|
| Nalidixic acid (NA) | nd* | nd | nd | nd | 36 (76.6) |
| Amoxicillin (AMC) | 20 (45.4) | 46 (47.9) | 8 (36.4) | 21 (58.3) | 18 (38.3) |
| Cephalexin (CP) | 24 (54.5) | 60 (62.5) | 10 (45.4) | nd | 13 (27.6) |
| Cefuroxime (CXM) | 4 (9.0) | 12 (12.5) | 2 (9.0) | 8 (22.2) | 13 (27.6) |
| Ciprofloxacin (CIP) | 3 (6.8) | 00 | 00 | 7 (19.4) | 12 (25.5) |
| Ceftriaxone (CTR) | 2 (4.5) | 2 (2.1) | 00 | 6 (16.7) | 11 (23.4) |
| Cefoxitin (CX) | nd | nd | nd | nd | 10 (21.3) |
| Azithromycin (AZM) | nd | nd | nd | nd | 10 (21.3) |
| Co-Trimoxazole (COT) | 18 (40.9) | 38 (39.5) | 2 (9.0) | 10 (27.8) | 9 (19.1) |
| Imipenem (I) | nd | nd | nd | nd | 4 (8.5) |
| Chloramphenicol (C) | 22 (50) | 52 (54.2) | 7 (31.8) | 9 (25) | 1 (2.1) |
nd=Not determined.
Mean minimum inhibitory (MIC in μg/ml) values of ceftriaxone, cefuroxlme, and azithromycin.
| Duration of Isolation | Ceftriaxone | Cefuroxime | Azithromycin |
|---|
| Range | Mean | Range | Mean | Range | Mean |
|---|
| 1987-1991 (Nath et al.,2010) [5] | 0.0312-0.0625 | 0.04709 | 2-32 | 12.5 | nd* | - |
| 1992-1996 (Nath et al.,2010) [5] | 0.0312-0.125 | 0.098 | 0.5-32 | 11.687 | nd* | - |
| 1997-2001 (Nath et al.,2010) [5] | 0.0625-2.0 | 0.211 | 0.5-64 | 16.5 | nd* | - |
| 2002-2006 (Nath et al.,2010) [5] | 0.0625-2.0 | 0.3652 | 2-128 | 21.28 | nd* | - |
| 2009-2010 (Pratap et al.,2012) [13] | 0.125-128 | 7.36 | nd* | nd* | nd* | - |
| 2011-2013 (Present study) | 0.125-128 | 23.7 | 0.5512 | 131.9 | 0.125128 | 26.5 |
nd=Not determined.
Multi-drug Resistance Patterns of Salmonella Typhi
Two of the 47 isolates were sensitive to all the drugs tested, while 65.9% (31/47) were resistant to one drug only. Further, two isolates (4.2%) were resistant to two drugs. Thus, 25.6% of the isolates could be designated as multidrug resistant. Further, 5 (10.6%) isolates were sensitive to only two drugs namely imipenem and chloramphenicol, while two isolates were susceptible only to one drug i.e., chloramphenicol [Table/Fig-3].
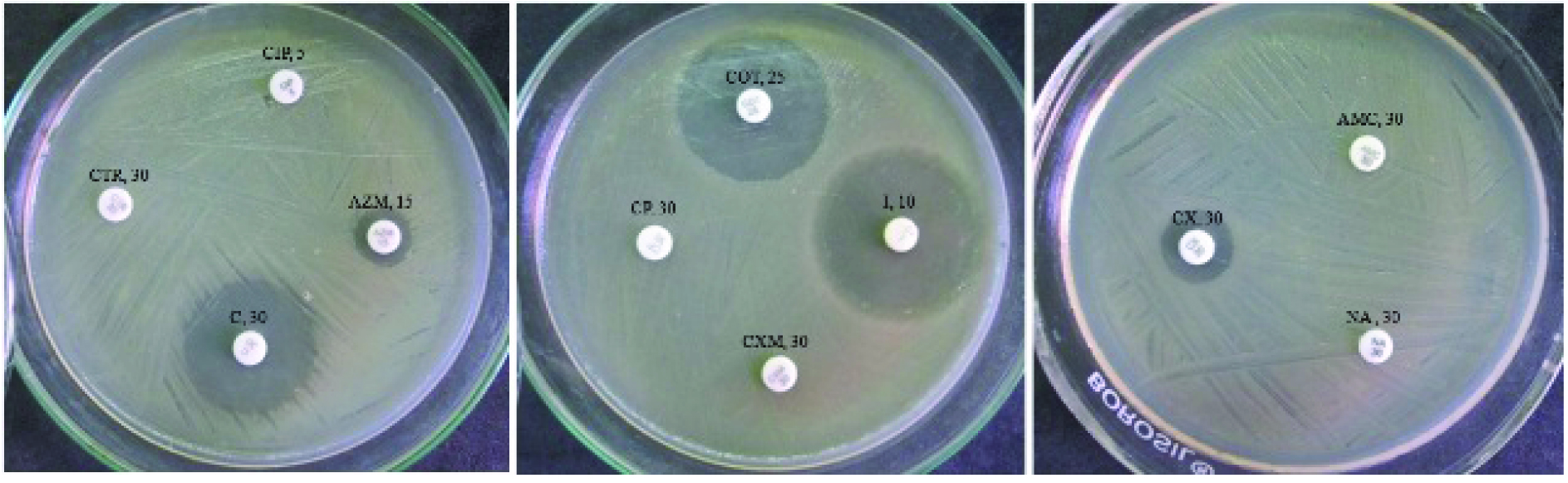
Image shows the antibiotic sensitivity test by disc diffusion method against S. Typhi isolates.
[Antibiotics uses: CTR-Ceftriaxone (30µg), Zone size=0 mm; CIP-Ciprofloxacin (5µg), Zone size=0 mm; AZM-Azithromycin (15µg), Zone size=12 mm; C- Chloramphenicol (30µg), Zone size=30 mm; CP-Cephalexin (30µg), Zone size=0 mm; COT-Co-Trimoxazole (25µg), Zone size=30 mm; I- Imipenem (10µg), Zone size=35 mm; CXM-Cefuroxime (30µg), Zone size=0 mm; AMC-Amoxicillin (30µg), Zone size=0 mm; NA-Nalidixic acid (30µg), Zone size=0 mm; and CX-Cefoxitin (30µg), Zone size=14 mm].
Minimum Inhibitory Concentration (MICs) of the Commonly Used Antimicrobial Drugs
All 47 S. Typhi isolates were tested against cefuroxime. The result of MIC showed that, 19 (40.4%) were found to be recommended breakpoint of MIC ≥32 µg/ml was taken into the consideration. The mean MIC value of all the 47 isolates was 131.9 µg/ml while the range of 0.5-512 µg/ml [Table/Fig-2]. Against ceftriaxone, a total of 19 (40.4%) isolates were found to be resistant with the mean MIC value of 23.7 µg/ml with the range of 0.125-128 µg/ml [Table/Fig-2]. For recently introduced azithromycin,18 (38.3%) isolates were found to be resistant when ≥8 µg/ml was taken as MIC breakpoint. The range of MIC was 0.125-128 µg/ml. Of them 6 (12.8%) had MIC value ≥64 µg/ml, one (2.1%) had ≥32 µg/ml, 10 (21.9%) had ≥16 µg/ml while one (2.1%) had ≥8 µg/ml. However, 29 (61.7%) isolates were found to be sensitive as they had MIC value ≤2 µg/ml.
Discussion
In the present study, the reversal of drug resistance pattern of S. Typhi is quite obvious. Study conducted on the isolates of this tertiary level hospital during 1980-1998, showed the isolation rate of multidrug resistant S. Typhi to be 79.6% [5], while those isolated during 2009-2010 showed the Multi-drug Resistance (MDR) rate of 25% [13]. It is intriguing to observe almost similar level (24.6%) of MDR isolation rate of S. Typhi during 2011-2013 in the present study. Similar declining pattern has also been reported from different parts of the India and other countries [14,15].
This change in pattern might be the result of restricted use of antibiotics for the therapy of typhoid fever after the report of emergence of Multidrug Resistance Salmonella Typhi (MDRST) against all the traditional drugs i.e. amoxicillin, chloramphenicol, and co-trimoxazole in late 1980s. As mentioned earlier, the quinolones were in vogue but within a decade, we were compelled to switch over to other groups of antibiotics. The most commonly used antibiotics were extended spectrum cephalosporins [16,17].
There were reports of gradual increase of mean MIC of the cephalosporins in the S. Typhi isolates from different parts of the world which later became obvious with clinical failures with ceftriaxone [18,19]. From our centre, while there was no report of resistance against this drug during 1990-1999, 16.7% of the isolates of the year 2009-2010 could be detected resistant that has further increased to 23.4% in the present study which has been carried out on the isolates of 2011-2013 [Table/Fig-1,2]. Azithromycin introduced for the treatment of typhoid fever is now showing therapeutic failures at our centre which could be verified by the finding of resistance in 21.3% of the recent isolates. However, rise in resistant isolates of S. Typhi against azithromycin has been reported from India and abroad (31%, 33.65%) [7,20]. However, it is very encouraging to see the return of conventional anti-typhoid drugs again. As reported by others, we have also observed that only one isolate (2.1%) was resistant to chloramphenicol, while 60% of the isolates were sensitive to amoxicillin and 80% of them to co-trimoxazole. Therefore, even if chloramphenicol is not being prescribed, co-trimoxazole alone or in combination with amoxicillin may be recommended for the empirical use in the treatment of typhoid fever. The increasing MIC with resultant emergence of drug resistance as shown the [Table/Fig-2] indicates that presently both the drugs i.e., azithromycin and ceftriaxone are not better than co-trimoxazole. On the basis of above observations, it may be suggested that the conventional drugs e.g., co-trimoxazole, ampicillin and chloramphenicol should be prescribed and ceftriaxone and azithromycin may be kept on hold for a while with the expectation of their come back in the treatment of S. Typhi infection. Moreover, large-scale randomised control trials with follow up and laboratory correlation is needed for usage of azithromycin and ceftriaxone in Southeast Asian countries and restraining from blindly following the western prescribing practices as typhoid is primarily not a problem to the developed countries. We have to generate actual data from the developing countries where typhoid is an endemic problem along with antibiotic resistance.
Limitation
The present study has included small number of isolates. It will not be prudent to draw a conclusion on such small pilot study. It would be better to carry out multicentric study involving eastern, western, and southern part of India. However, it is still better if other countries of South East Asia will also be involved.
Conclusion
It was intriguing to observe that there was significant come back of conventional anti-typhoid antibiotics with the resistance rate of 38.3% for amoxicillin, 19.1% for co- trimoxazole and 2.1% for chloramphenicol. On the basis of present findings, we may suggest that combination of any of the two above conventional drugs may be prescribed empirically in the therapy of typhoid fever.