Mastoid Osteoma of Temporal Bone – A Rare Case Report
Rahul Kumar Singh1, Amit Goyal2, Amit Kumar3, Gaurav Kataria4, Amber Kesarwani5
1 Senior Resident, Department of Otorhinolaryngology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
2 Additional Professor, Department of Otorhinolaryngology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
3 Senior Resident, Department of Otorhinolaryngology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
4 Senior Resident, Department of Otorhinolaryngology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
5 Senior Resident, Department of Otorhinolaryngology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rahul Kumar Singh, Department of Otorhinolaryngology, All India Institute of Medical Sciences, Jodhpur-342005, Rajasthan, India.
E-mail: dr.rksingh23@gmail.com
Osteomas of the temporal bone are rare entity with incidence of 0.1% - 1% of all benign tumours of skull. They are slow growing benign lesion of temporal bone. We report a rare case of mastoid osteoma of size more than 5 cm. A 40-year-old female patient presented to us with left post auricular bony swelling of size greater than 5 cm. Diagnosis of mastoid osteoma was made after relevant investigations including High Resolution Computed Tomography (HRCT) temporal bone. Complete surgical excision was done with good cosmetic outcome without recurrence.
Auricular incision, Benign lesion, Cosmetic deformity
Case Report
A 40-year-old female presented to Outpatient Department of our hospital with the chief complaint of hard swelling in post auricular region for 3-4 years which was progressively increasing in size. She didn’t complain of any pain or other symptoms related to swelling except for cosmetic deformity. On examination, there was a single pyramidal shaped swelling with smooth margin of size around 5.5 x 4.5 cm at left post auricular region [Table/Fig-1]. Swelling was bony hard in consistency, covered with skin, non tender and its base fixed to underlying bone. Surrounding area was devoid of any sinus or fistula. Past history of patient didn’t reveal any history of trauma or infection. Otoscopic examination and audiometry were normal.
Patient presenting with left mastoid osteoma with size more than 5 cm. (Left to right).

X-Ray of mastoid of temporal bone showing mastoid osteoma (arrow). (Left to right).
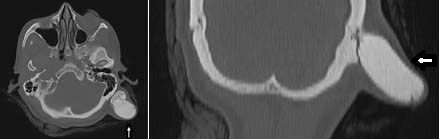
X-Ray skull lateral view showed a well defined, round to oval dense radiopacity in left mastoid region [Table/Fig-2]. On HRCT scan of the temporal bone, exophytic osseous mass in left post auricular region arising from left mastoid bone was noted [Table/Fig-3]. The middle ear cavity along with ossicular chain and inner table of skull plus diploe were normal with no intracranial extension. On the basis of above findings, a provisional diagnosis of mastoid osteoma was made.
High Resolution Computed Tomography (HRCT) of temporal bone in axial and coronal plane showing mastoid osteoma (arrow). (Left to right).
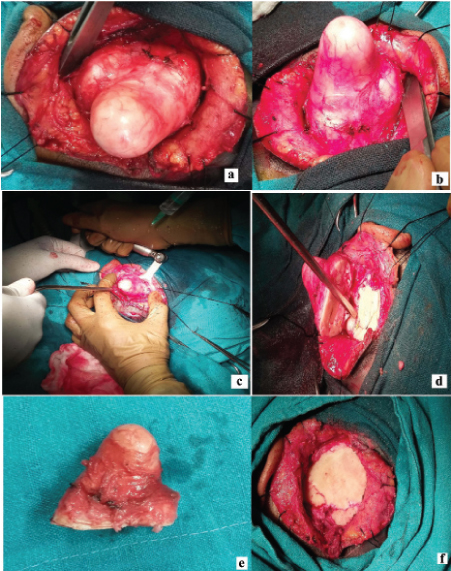
A 10 cm modified post auricular incision was given over the swelling and subcutaneous flap was elevated to provide complete exposure of the osteoma. Osteoma was removed from base using electric saw and rest of osteoma bone was drilled flush to outer table of skull to ensure complete removal and prevent recurrence [Table/Fig-4]. The wound was closed in layers over a corrugated rubber drain and stitches were removed seven days after surgery without any complications. On regular follow up (two months), no reccurance of lesion was noted. Patient was with good cosmetic cover and complains of no pain.
Intraoperative pictures of left mastoid osteoma from wide exposure to complete surgical excision; (a) Exposure of mastoid osteoma; (b) Exposure of base of osteoma; (c) Cutting mastoid osteoma from its base; (d) Removing osteoma and its underlying attachment to bone; (e) Osteoma after complete removal; (f)Underlying normal bone after removal of osteoma.
Discussion
Temporal bone osteomas are rare. Incidence of temporal bone osteomas generally is 0.1%- 1% of all benign tumours of skull [1]. Within the temporal bone, osteomas are commonly reported in the external auditory meatus, middle ear, styloid process, temporomandibular joint, apex of the petrous temporal bone, internal auditory canal. However, it is reported rarely of this size in the mastoid region as in our case [2].
Clinically, it is difficult to classify type of osteoma because of similar presentations. There are three types of osteoma of mastoid reported in literature as: osteoma compactum, osteoma cancellare, and osteoma cartilagineum based on histology. Compact osteomas have a wider base and are very slow growing whereas spongy osteomas are more likely to be pedunculated and grow relatively faster [3]. Osteoma occurrence can be divided into syndromic and nonsyndromic. For example, Gardener’s syndrome comprises of multiple intestinal polyps, mesentery and skin fibromas, epidermoid inclusion cysts and osteomas with a tendency of occurrence in membranous bones such as maxilla and mandible [4].
Aetiology of nonsyndromic temporal bone osteomas are not known and various possible causes have been reported in literature and previous case reports. These include genetic origin, trauma, surgery, radiotherapy, chronic infections and pituitary dysfunctions [3]. Our case had single pyramid shaped mastoid osteoma without any obvious aetiological history as stated above.
Temporal bone osteoma swellings are usually painless like in our case. They however can be painful gradually with cosmetic disfigurement as well as there can be difficulty in wearing glasses. Rarely, the petrous part of the temporal bone may be involved along with facial nerve and part of the internal ear that leads to hearing loss as a complication [5]. Differential diagnosis of mastoid osteomas may include osteosarcoma, osteoblastic metastasis, isolated eosinophilic granuloma, Paget’s disease, giant cell tumour, osteoid osteoma, calcified meningioma and monostotic fibrous dysplasia [3].
Non contrast CT scan is the imaging method of choice for temporal bone osteomas and other osteomas. On imaging, ivory osteomas appear radiodense, similar to normal cortex, whereas mature osteomas may demonstrate central marrow. It is seen as a high opacity, well-demarcated, and dense growth of sclerotic lesion from the mastoid bone [5].
Surgical resection is the treatment of choice with most common indication being cosmetic disfigurement followed by associated symptoms, and also to prevent its later complications, which can be caused by giant osteomas [5].
Conclusion
Mastoid osteomas of temporal bone are rare benign slow growing tumours. They are usually asymptomatic unless it gradually increases in size to cause cosmetic disfigurement and sometimes pain. Radiological investigations are required to find extent with Non contrast CT as modality of choice. Complete surgical excision is treatment of choice with drilling of mastoid cortex if necessary to prevent recurrences which are occasionally reported. Complete removal of osteoma invariably achieves good cosmetic results.
[1]. Smud D, Augustin G, Kekez T, Kinda E, Majerovic M, Jelincic Z, Gardner’s syndrome:Genetic testing and colonoscopy are indicated in adolescents and young adults with cranial osteomas:A case reportWorld Journal of Gastroenterology 2007 13(28):3900-03. [Google Scholar]
[2]. El Fakiri M, El Bakkouri W, Halimi C, Aı¨t Mansour A, Ayache D, Mastoid osteoma: Report of two casesEuropian Annals of Otorhinolaryngology, Head Neck Dis 2011 128:266-68. [Google Scholar]
[3]. Parelkar K, Thorawade V, Jagade M, Kar R, Pandare M, Nataraj R, Osteoma of temporal bone—A rare case reportInternational Journal of Otolaryngology and Head and Neck Surgery 2014 3:252-58. [Google Scholar]
[4]. Harley EH, Berkowitz RG, Imaging case study of the month, osteoma of the middle earAnn Otol Rhinol Laryngol 1997 106:714 [Google Scholar]
[5]. Parashari UC, Khanduri S, Singh N, Bhadury S, Mastoid osteomaIndian J Otol 2014 20:132-33. [Google Scholar]