Small Intestinal Lymphangioma Presenting as an Acute Abdomen with Relevant Review of Literature
Basant Kumar1, Ankur Bhatnagar2, Vijai Datta Upadhyaya3, Ajay Narayan Gangopadhyay4
1 Associate Professor, Department of Paediatric Surgery, SGPGIMS, Lucknow, Uttar Pradesh, India.
2 Associate Professor, Department of Plastic Surgery, SGPGIMS, Lucknow, Uttar Pradesh, India.
3 Associate Professor, Department of Paediatric Surgery, SGPGIMS, Varanasi, Uttar Pradesh, India.
4 Professor, Department of Paediatric Surgery, IMS BHU, Varanasi, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vijai Datta Upadhyaya, Associate Professor, Department of Paediatric Surgery, SGPGIMS, Varanasi-221206, Uttar Pradesh, India.
E-mail: upadhyayavj@rediffmail.com
Cystic lymphangioma of small bowel mesentery is rare with clinical features ranging from an asymptomatic abdominal lump to acute intestinal obstruction. We discuss two cases of lymphangioma of small bowel mesentery who presented to us as acute intestinal obstruction. In the first case exploratory laparotomy revealed a large multicystic lesion arising from small bowel mesentery just distal to the duodenojejunal junction having multiple small cysts filled with milky white fluid. The involved region of the bowel was excised. The second case had a large multicystic lesion involving the mesentery of proximal jejunum, dudenojejunal junction, encasing the entire superior mesenteric vessels. For this patient, debulking was done.
Abdominal obstruction, Laparotomy, Multicystic lesion
Case – 1
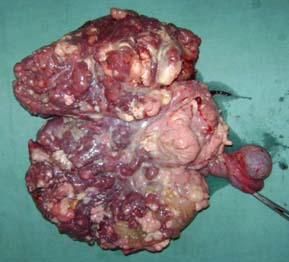
A 10-year-old male child presented with abdominal pain and distension and diagnosed as case of acute intestinal obstruction. On physical examination, the abdomen was uniformly distended, with mild tenderness and guarding without rigidity. Initial hematological and biochemical investigation did not reveal gross abnormality. Plain x-ray abdomen was suggestive of intestinal obstruction. Exploratory laparotomy revealed a large multicystic lesion arising from small bowel mesentery just distal to the duodenojejunal junction [Table/Fig-1]. The lesion on examination had multiple small cysts filled with milky white fluid. The involved bowel was excised and end to end jejuno-ileal anastomosis was done. Postoperative course was uneventful and histology was consistent with lymphangioma. Patient is doing well after follow up of five years.
Resected specimen showing multiple lymphangioma involving the small intestine and its mesentery.
X-ray abdomen erect: showing gasless abdomen.

Case – 2
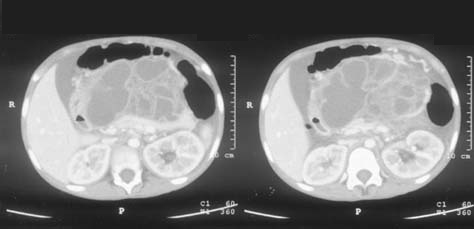
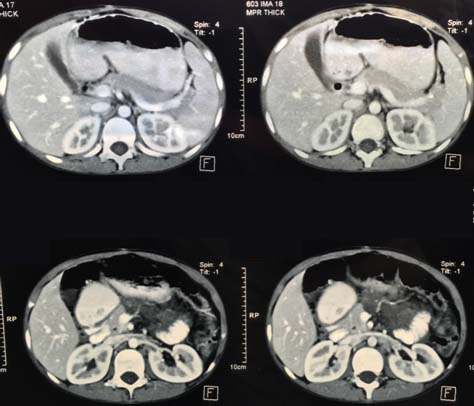
An eight-year-old male child, presented with feature suggestive of acute intestinal obstruction for last two days. History revealed on and off abdominal distension, pain and vomiting since one month. Ill-defined lump in upper abdomen, which was soft to firm in consistency, non-tender, moving with respiration was observed on local examination. X-ray showed gasless abdomen [Table/Fig-2], Ultrasound abdomen showed large multicystic mass encasing superior mesenteric vessel, duodenum and small bowel loops. CT scan revealed a large intrabdominal multicystic lesion involving the small bowel [Table/Fig-3] however, site of origin of the lesion could not be ascertained. Since diagnosis was not clear and patient was having features of acute intestinal obstruction, it was decided to perform an exploratory laparotomy which revealed a large multicystic lesion, involving the mesentery of proximal jejunum, dudenojejunal junction as well as encasing the entire superior mesenteric vessels. Debulking of lesion was done as complete excision was not possible. Histopathology was consistent with lymphatic malformation. Postoperative period was uneventful and repeat CECT at end of one year showed minimal residual mass [Table/Fig-4].
CT Scan: showing multiple cystic lesion involving small bowel and its mesentery.
CT scan after one year showing very small residual lesion of lymphangioma.
Discussion
Mesenteric cystic lymphangioma is a rare benign intraabdominal anomaly with uncertain aetiology, predominantly occurring in children [1]. Almost 60% of mesenteric cystic lymphangiomas are diagnosed before the fifth year of life [2]. Most (95%) occur in the neck and axillary regions; the remaining 5% is located in the mesentery, retroperitoneum, abdominal viscera, lung, and mediastinum [3-5]. Isolated occurrence in the mesentery of small intestine is exceptionally rare accounting to less than 1% of all lymphangioma [5]. Mesenteric cystic lymphangioma may remain asymptomatic or present with complications depending on the size and location of the lesion.
Aetiology of lymphangioma is uncertain but a popular theory, the ‘blind sac’ hypothesis, postulates that a lack of lymphatic connections causes them to proliferate and dilate [6-8]. However, these malformations may occur after: abdominal trauma, lymphatic obstruction, inflammatory process, and surgery or radiation therapy. Mesenteric lymphangiomas my remain asymptomatic though clinical presentation can range from an incidentally-discovered abdominal mass to symptoms of an acute abdomen [4,5]. The most common presentation for this entity is freely mobile non tender abdominal mass, with feature of partial small intestinal obstruction [9-11]. Intestinal obstruction in these patients may be due to adhesion of intestine because of infected cyst or due to intestinal volvulus when they are in close proximity of Duodeno-jejunal Junction (DJ), (one of our cases the lesion was involving the DJ but was not associated with volvulus as described in literature). The exact diagnosis is usually made after surgical exploration on histopathological evaluation.
Ultrasonography and CT are considered as the most appropriate radio-diagnostic modalities to evaluate mesenteric lymphangioma, although ultrasonography is usually sufficient. Ultrasonography can differentiate the lymphangiomas from simple mesenteric cyst, because the fluid contents in lymphangiomas are usually homogeneous, and attenuation values may range between those of fat and fluid.
On CT scans, mesenteric lymphangiomas appear as uni- or multilocular masses containing septa of variable thickness; enhancement of the wall is revealed by contrast medium. Optimal treatment is radical excision [10-12], but it is not always possible to excise the cyst in toto, as in our second case debulking surgery was done. Though debulking surgery has not been described in literature but was effective in our case. In cases where complete excision of cyst is not possible intralesional sclerotherapy with OK-432 had been advocated by few authors to prevent recurrence [8]. However, we did not perform intralesional sclerotherapy in our patients. None of the patients showed an increase in the residual lesion after one year of follow up. Thus, we believe that debulking surgery without sclerotherapy has a role in such lesion. It helps to relive the acute intestinal obstruction, but such patients need strict follow up for long time.
Conclusion
Mesenteric lymphangiomas may be invasive and grow to an enormous size but are not malignant hence possesses good prognosis. Complete excision is treatment of choice though debulking surgery may be of help in certain cases.
[1]. Konen O, Rathaus V, Dlugy E, Freud E, Kessler A, Shapiro M, Childhood abdominal cystic lymphangiomaPediatr Radiol 2002 32:88-94. [Google Scholar]
[2]. Steyaert H, Guitard J, Moscovici J, Juricic M, Vaysse P, Juskiewenski S, Abdominal cystic lymphangioma in children:benign lesions that can have a proliferative courseJ Pedatr Surg 1996 31(Pt5):677-80. [Google Scholar]
[3]. Liu Y, Peng Y, Li J, Zeng J, Sun G, Gao P, MSCT manifestations with pathologic correlation of abdominal gastrointestinal tract and mesenteric tumor and tumor-like lesions in children:a single center experienceEur J Radiol 2010 75:293-300. [Google Scholar]
[4]. Guth S, Gocke C, Gebhardt J, Schwenk W, Caselitz J, Bamberger CM, Mesenterial lymphangiolipoma - a rare finding in an asymptomatic patientMed Klin (Munich) 2010 105(12):948-51. [Google Scholar]
[5]. Mendez-Gallart R, Solar-Boga A, Gomez-Tellado M, Somoza-Argibay I, Giant mesenteric cystic lymphangioma in an infant presenting with acute bowel obstructionCandian Journal of Surgery 2009 52(3):E42-E43. [Google Scholar]
[6]. Minocha PK, Roop L, Persad R, Cases of atypical lymphangiomas in childrenCase Reports in Pediatrics 2014 2014:626198 [Google Scholar]
[7]. Chen CW, Hsu SD, Lin CH, Cheng MF, Yu JC, Cystic lymphangioma of the jejunal mesentery in an adult:a case reportWorld J Gastroenterol 2005 11:5084-86. [Google Scholar]
[8]. Chung JC, Song OP, Cystic lymphangioma of the jejunal mesentery presenting with acute abdomen in an adultCanadian Journal of Surgery 2009 52:E286-88. [Google Scholar]
[9]. Kosir MA, Sonnino RE, Gauderer MW, Pediatric abdominal lymphangiomas:a plea for early recognitionJ Pediatr Surg 1991 26(11):1309-13. [Google Scholar]
[10]. Talrico F, Iusco D, Negri L, Valieri L, Mesenteric cystic lymphangioma treated with laparoscopic excision:case report and review of literatureG Chir 2009 30(8-9):362-64. [Google Scholar]
[11]. Weeda VB, Booij KAC, Aronson DC, Mesenteric cystic lymphangioma:a congenital and an acquired anomaly?Two cases and a review of the literatureJ Pediatr Surg 2008 43(6):1206-08. [Google Scholar]
[12]. Losanoff JE, Kjossev KT, Mesenteric cystic lymphnagioma:unusual cause of intra abdominal catastrophe in adultInt J Clini Pract 2005 59:986-87. [Google Scholar]