Bilateral Solitary Glomus Tumour of Thumb: A Case Report
Vinay Mathew Joseph1, Venkateshwar Reddy Maryada2, Gurava Reddy Venkata3, Praharsha Mulpur4, Muralidhar Sagi5
1 Resident, Department of Orthopaedics, Sunshine Hospital, Secunderabad, Andhra Pradesh, India.
2 Consultant Hand Surgeon, Department of Orthopaedics, Sunshine Hospital, Secunderabad, Andhra Pradesh, India.
3 Consultant, Department of Orthopaedics, Sunshine Hospital, Secunderabad, Andhra Pradesh, India.
4 Resident, Department of Orthopaedics, Sunshine Hospital, Secunderabad, Andhra Pradesh, India.
5 Registrar, Department of Orthopaedics, Sunshine Hospital, Secunderabad, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vinay Mathew Joseph, Resident, Department of Orthopaedics, Sunshine Hospital, Secunderabad-500003, Andhra Pradesh, India.
E-mail: dr.vinayjoseph@gmail.com
Glomus tumours are benign neoplastic lesions of glomus body, a thermoregulatory apparatus of cutaneous microvasculature. These tumours can arise at any location of the body but most commonly seen in subungual region of fingers. Bilateral solitary glomus tumour of hand is a rare entity. We report a case of 54-year-old female who presented with complaints of pain in the right thumb since three years and left thumb pain since 20 years. Clinical examination revealed acute tenderness of both the thumbs. Love’s pin test and Hildreth’s test were positive. MRI revealed characteristic features of glomus tumour. Excision of both the lesions was done and proceeds forwarded to histopathology which confirmed diagnosis. Patient was symptom free immediately following surgery. No nail deformities were noticed and there was no recurrence of symptoms in one year follow up. Glomus tumours of the hand are a rare entity and often missed.
Finger pathology, Phalynx, Transungual approach
Case Report
We report a case of a 54-year-old female who presented to the outpatient department with complaints of pain over left thumb since 20 years and right thumb since three years.
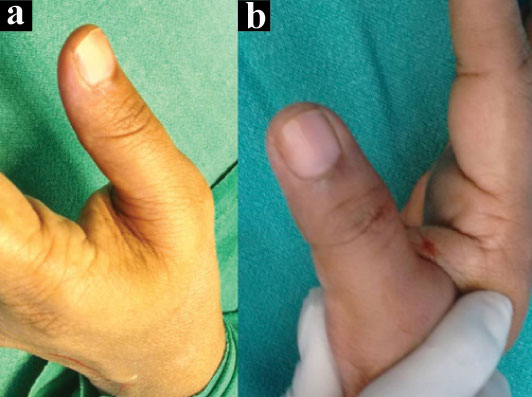
She had sought medical attention for the same before and was advised various non specific treatment. Clinical examination revealed acute tenderness of both thumbs with no visible deformity or skin changes [Table/Fig-1]. Love’s pin test and Hildreth’s test were positive.
Pre operative clinical picture of left thumb (a); and right thumb (b).
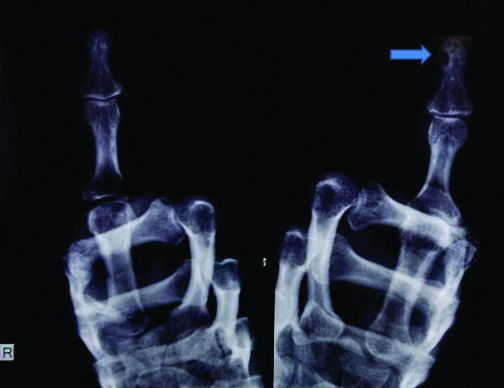
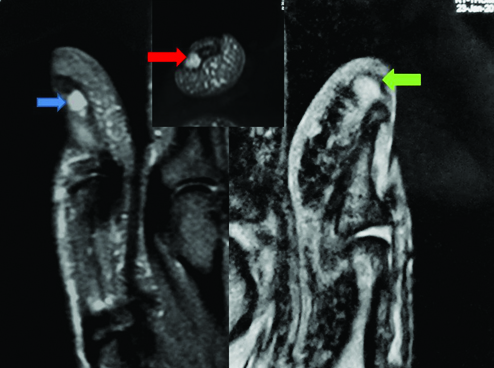
Radiography revealed erosion of the left thumb terminal phalynx and no obvious changes in the right thumb [Table/Fig-2]. Clinical diagnosis of glomus tumour was made and MRI was advised. MRI showed well circumscribed hyperintense lesion in fat saturated T2 weighted images in the distal tip of right thumb beyond the phalynx and subungual region of left thumb with erosive changes of the distal phalynx suggestive of glomus tumour [Table/Fig-3].
Preoperative radiograph - Solid arrow showing erosion of the terminal phalynx of left thumb.
Pre operative MRI- T2W image showing well circumscribed hyperintese lesion at subungual region of left thumb (blue arrow) and distal tip of volar pulp on the right thumb (green arrow). Axial image showing subungual location of lesion in left thumb (red arrow).
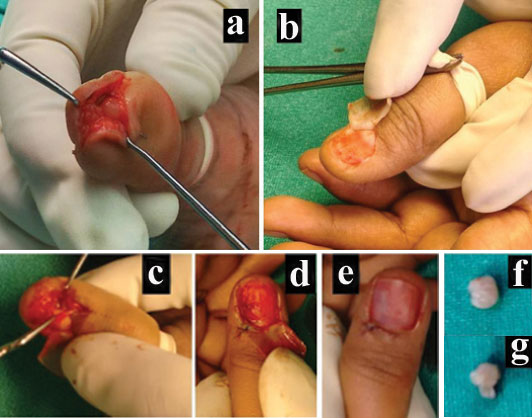
Both the lesions were managed with surgical excision in toto under digital block and tourniquet cover. Transungual approach was taken for the left thumb and lesion in the right thumb was approached directly by fish mouth incision [Table/Fig-4]. The proceeds were sent for histopatholocial examination and confirmed to be glomus tumour [Table/Fig-5]. The patient was symptom free following surgery and developed no nail deformity or recurrence in up to one year of follow up.
Surgical steps- Volar apporach for right thumb (a). Subungual approach for left thumb (b), vertical incison over nail bed taken and tumour excised (c) after which nail bed is repaired (d) and nail repositioned (e) Lesion excised from right thumb (f). Lesion excised from left thumb (g).
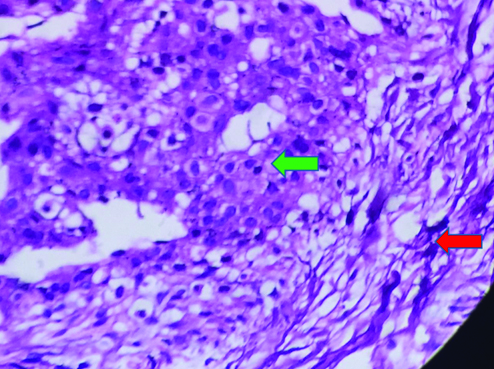
Histopathology: section showing well circumscribed tumour tissue in the dermis composed of smooth muscle fibres arranged in bundles (red arrow) separated by ectatic thin walled blood vessels surrounded by monotonous population of round to oval cells (green arrow), with no evidence of necrosis, mitosis or nuclear pleomorphism (40X).
Discussion
Glomus body is a thermoregulatory apparatus of cutaneous microvasculature. A hamartomatous lesion of this apparatus results in a benign tumour which is termed as glomus tumour [1]. Specialized perivascular smooth muscles in this area are temperature sensitive and are known as glomus cells. The glomus tumour arises from arterial portion of this anastomosis or the Sucquet-Hoyer canal as hamartomatous changes in the glomus cells [1]. These lesions can occur at any cutaneous location or mucous membrane lining of internal organs [2,3]. The most common location is the subungual region of fingers [4]. They can be solitary or multiple the former being more common. Multiple glomus tumours when present should be differentiated from other pathological lesions like cavernous haemangioma and blue rubber-bleb nevus syndrome [2]. Solitary lesions unlike multiple variant are symptomatic and show predilection to fingers. These constitute 1-5% of all hand tumours [1]. Bilateral glomus tumours are rare entity and in our literature search we found only one isolated case report on bilateral solitary glomus tumour of hand [5]. Glomus tumours of the hand are painful and debilitating lesions. The mean duration on presentation due to faulty diagnosis and mismanagement also ranges between one to nine years. The largest reported series of glomus tumour mentions the importance of clinical diagnosis with classic triad of pain, tenderness and cold insensitivity [6-8]. Solitary lesions are more frequent in women and show predilection to subungual region of hand [4]. Bilateral subungual glomus tumours are very rare. Surgical excision is the best modality of treatment for symptomatic lesions [6,7]. Approach is decided according to the location of the lesion and various approaches have been described including periungual, paraungual and transungual. Various published reports have stated that transungual approach is associated with nail deformity [6,7]. Jawalkar H et al., in a study of 12 glomus tumours treated with transungual excision reported to have no recurrence or new nail deformity [9]. In our case, we have operated the right thumb with paraungual approach and left thumb with transungual approach based on location of the tumour and no recurrence was noted up to one year of follow up. Similarly in a case report by Sank AC et al., the lesion became symptomatic and showed no recurrence after complete surgical excision [5].
Conclusion
Glomus tumours of hands which are symptomatic are successfully treated with surgical excision. High index of suspicion and careful clinical examination is the crux of diagnosing this condition. Delayed or misdiagnosis and improper management results in undue suffering for patient. Though bilateral glomus tumours are rare, the possibility should not be excluded in bilateral unexplained digital pain.
[1]. McDermott EM, Weiss AP, Glomus tumoursJ Hand Surg Am 2006 31:1397-400. [Google Scholar]
[2]. Chatterjee JS, Youssef AH, Brown RM, Nishikawa H, Congenital nodular multiple glomangioma: a case reportJ Clin Pathol 2005 58:102-03. [Google Scholar]
[3]. Shugart RR, Soule EH, Johnson EW Jr, Glomus tumourSurg Gynecol Obstet 1963 117:334-40. [Google Scholar]
[4]. Rettig AC, Strickland JW, Glomus tumour of the digitsJ Hand Surg Am 1977 2:261-65. [Google Scholar]
[5]. Sank AC, McClinton MA, Bilateral solitary glomus tumours of handsAnn Plast Surg 1992 28(3):301-03. [Google Scholar]
[6]. Vasisht B, Watson HK, Joseph E, Lionelli GT, Digital glomus tumours: a 29-year experience with a lateral subperiosteal approachPlast Reconstr Surg 2004 114:1486-89. [Google Scholar]
[7]. Van Geertruyden J, Lorea P, Goldschmidt D, e Fontaine S, Schuind F, Kinnen L, Glomus tumours of the hand: a retrospective study of 51 casesJ Hand Surg Br 1996 21:257-60. [Google Scholar]
[8]. Gandon F, Legaillard P, Brueton R, Le Viet D, Foucher G, Forty eight glomus tumours of the hand. Retrospective study and four year follow upAnn Chir Main Memb Super 1992 11(5):401-05. [Google Scholar]
[9]. Jawalkar H, Maryada VR, Brahmajoshyula V, Kotha GK, Subungual glomus tumours of the hand: Treated by transungual excisionIndian J Orthop 2015 49(4):403-07. [Google Scholar]