Denture disinfection has been recommended as an indispensable procedure for preventing cross contamination and the maintenance of a healthy oral mucosa in patients rehabilitated with removable dental prosthesis [1]. Removable dentures are susceptible to colonization of microorganisms including pathogenic and opportunistic bacteria and fungi resulting in cross contamination between patients, dentists and laboratory technicians [2-4]. Denture base surface retaining microorganisms are difficult to clean with conventional toothbrushing methods necessitating disinfection procedures. A microorganism commonly associated with dentures is Candida albicans whose colonization is significantly predisposed to insufficient oral hygiene [5]. To bring about effective disinfection, literature suggests the use of various chemical disinfectants that include glutaraldehyde, sodium hypochlorite, iodoform, carbon dioxide, chlorhexidine, or alcoholic solutions [6]. Few denture cleansers such as alkaline peroxide solutions, hypochlorite, vinegar solutions have also been proven to be effective chemical disinfectants [7,8]. Alternative to chemical disinfection, various studies have recommended microwave irradiation which is a proven method to kill microorganisms [9,10].
Introduced in the early 1930s, acrylic resin teeth are still used today in removable dental prostheses due to their superior aesthetics, high adhesion to the denture base material, excellent impact absorption and passivity to occlusal adjustment and polishing [11]. This, ideally, demands an inherent inertness of physical and mechanical properties of poly methylmethacrylate copolymer, commonly used material in denture base resins and acrylic resin denture teeth following the disinfection process [12]. However, immersion of a denture in a suitable chemical disinfectant solution or by undergoing microwave irradiation for an adequate length of time have known to cause changes in different physical and mechanical properties of acrylic resins [1,6,13]. One such commmonly examined mechanical property indicator for synthetic artificial tooth materials is hardness [14-16].
Considering the clinical scenario wherein several disinfection procedures may be necessary for infection control, the effect of repeated exposure of the materials to the disinfection methods should be evaluated. Thus, the current study aims to assess the surface hardness of acrylic resin teeth of three different commercial brands (Ivoclar, Newace, Acryrock) used in dental prostheses following chemical (2% glutaraldehyde, 1% sodium hypochlorite) and microwave disinfections. The null hypothesis of this study was that different disinfection methods would not cause any effects on the surface hardness of acrylic resin teeth of different commercial brands.
Materials and Methods
The in vitro study was conducted in Christian Dental College, CMC, Ludhiana, Punjab, India, for a period of five weeks during the months of March 2016 and April 2016 after the research committee clearance was obtained. Three commercially available brands of teeth were used in the study: Ivostar (Ivoclar Vivadent, Schaan, Liechtenstein); Newace Anterior (Yamahachi Dental Co., Gamagori, Japan) and Acryrock V (Ruthinium group, Italy). Ivostar and Newace Anterior are conventional polymethylmethacrylate acrylic resin teeth while Acryrock V is a crosslinked polymethylmethacrylate acrylic resin tooth. Lower central and lateral incisors were used for the experiment as the almost flat labial surface of the lower incisors allowed measurement of the microhardness values in a surface that did not need to be flattened by grinding and polished again. Based on the previous study, sample size of ten teeth of each brand was selected for the following experimental protocols [6]:
| Sample groups |
|---|
| C | Control without any disinfection |
| G1 | Glutaraldehyde disinfection following one cycle |
| G3 | Glutaraldehyde disinfection following three cycles |
| H1 | Sodium hypochlorite disinfection following one cycle |
| H3 | Sodium hypochlorite disinfection following three cycles |
| M1 | Microwave disinfection following one cycle |
| M3 | Microwave disinfection following three cycles |
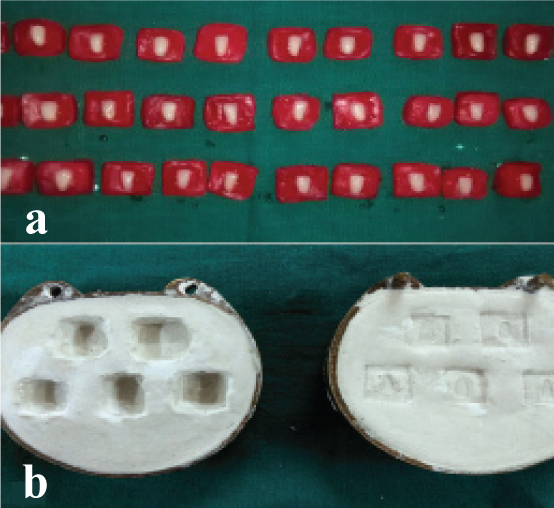
PVC cylinders (Tupperware India Pvt. Ltd., Gurgaon, India) of 6 mm high, 20 mm length and 20 mm breadth dimensions were impressed with putty (Flexceed, GC Tokyo; Japan) and wax (Cavex Set Up Wax, Cavex Holland BV; Netherlands) were poured into the putty mold to obtain wax cylinders. Teeth were fixed in the wax with the labial surface facing up [Table/Fig-1a]. Flasking (Varsity flask, Jabbar & Co, New Delhi; India) and dewaxing, of waxed up teeth blocks were done [Table/Fig-1b]. These procedures were succeeded by packing and acrylisation in acryliser unit (Unident Instruments Private Limited, New Delhi; India) in the conventional manner. After cooling of the flasks, the specimens were retrieved. Sharp and uneven edges of specimen were trimmed with acrylic trimmer. Ten specimens of each commercial brand were made for control and each simulated disinfection type and stored in distilled water at room temperature for 24 hours [Table/Fig-2].
a) Teeth fixed in wax; b) Dewaxed moulds.
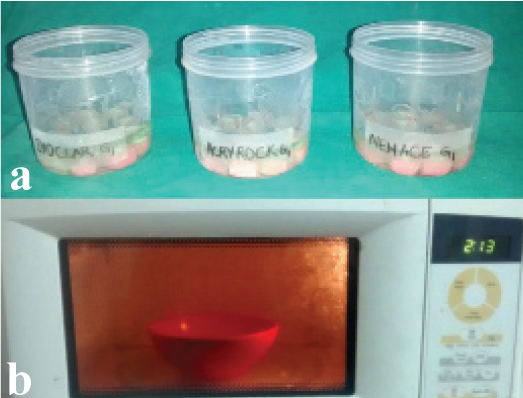
Specimens immersed in distilled water.

After water storage, separate sets of specimens of ten sample each were immersed in 2% glutaraldehyde (Glutarex, 3M, Mumbai) for G1 and G3 cycles and 1% sodium hypochlorite (Hypox, Kashyap Industries, Gujarat) for H1 and H3 cycles at room temperature for 10 minutes [Table/Fig-3a]. After every cycle of chemical disinfection, the specimens were washed in tap water for 30 seconds, dried with air jets and stored in distilled water at room temperature for seven days. Irradiation with microwave for M1 and M3 cycles was done in domestic microwave (Samsung India, Gurgaon, India) with 650 W for 3 minutes with the specimens immersed in 150 ml of distilled water [Table/Fig-3b].
a) Specimens in glutaraldehyde solution; b) Microwave irradiation of specimens.
For G3, H3 and M3, the process of disinfection was repeated thrice with an interval of seven days between each disinfection cycle. After the last cycle, the specimens remained in distilled water for another seven days. Vickers hardness measurements were made using a diamond hardness indenter (Banbros Engineering Private Limited) under a load of 50 g force (0.5 Newton) for 10 seconds for the procedures [Table/Fig-4].
Vickers hardness measurements were made using a hardness indenter.

Three indentations were made on the labial surface of the teeth, and the arithmetic mean was considered as the Vickers hardness number of each tooth. A single examiner performed all tests.
Statistical Analysis
Data was subjected to repeated measure two-way ANOVA test and Tukey’s test. The level of significance for the study was considered as p<0.05. Statistical Package for the Social Sciences (SPSS) version 17.0 software was used for statistical analysis.
Results
[Table/Fig-5] describes mean and standard deviation of the three readings of Vickers hardness number for different experimental groups. It was observed that there were statistically significant differences for the variables disinfection, tooth, and cycle. The interactions between disinfection and tooth, disinfection and cycle were statistically significant (p<0.001 for teeth and disinfectant interaction, p<0.001 cycle and disinfectant interaction) [Table/Fig-6, 7].
Descriptive table showing mean and standard deviation.
| Tooth | Cycle | Disinfectant | n | First reading | Second reading | Third reading |
|---|
| Mean | SD | Mean | SD | Mean | SD |
|---|
| Acryrock | 0 | Control | 10 | 16.40 | 0.84 | 16.40 | 1.08 | 16.00 | 0.67 |
| 1 | Glutaraldehyde | 10 | 15.50 | 0.97 | 15.80 | 0.63 | 16.10 | 0.88 |
| Sodium hypochlorite | 10 | 15.90 | 0.99 | 16.10 | 0.74 | 16.40 | 0.84 |
| Microwave | 10 | 16.00 | 0.81 | 15.90 | 0.88 | 16.30 | 0.48 |
| 3 | Glutaraldehyde | 10 | 15.80 | 0.63 | 16.20 | 0.79 | 15.90 | 0.74 |
| Sodium hypochlorite | 10 | 15.80 | 1.03 | 16.30 | 0.48 | 16.50 | 0.71 |
| Microwave | 10 | 13.50 | 1.08 | 14.70 | 0.95 | 14.20 | 1.62 |
| Newace | 0 | Control | 10 | 18.10 | 0.74 | 18.00 | 0.94 | 17.50 | 0.85 |
| 1 | Glutaraldehyde | 10 | 16.80 | 1.23 | 17.10 | 1.10 | 17.00 | 1.16 |
| Sodium hypochlorite | 10 | 17.80 | 1.03 | 17.20 | 0.42 | 17.60 | 0.70 |
| Microwave | 10 | 17.60 | 1.43 | 17.50 | 1.18 | 17.70 | 1.34 |
| 3 | Glutaraldehyde | 10 | 17.30 | 1.42 | 17.00 | 0.94 | 17.80 | 0.79 |
| Sodium hypochlorite | 10 | 17.00 | 1.25 | 17.70 | 1.06 | 17.30 | 1.06 |
| Microwave | 10 | 15.20 | 0.79 | 15.40 | 1.27 | 15.80 | 0.79 |
| Ivoclar | 0 | Control | 10 | 20.50 | 0.85 | 20.70 | 0.95 | 20.30 | 0.95 |
| 1 | Glutaraldehyde | 10 | 19.70 | 1.34 | 19.40 | 0.97 | 19.30 | 1.34 |
| Sodium hypochlorite | 10 | 19.60 | 1.08 | 19.40 | 1.58 | 19.90 | 1.10 |
| Microwave | 10 | 19.80 | 1.03 | 19.30 | 0.95 | 19.40 | 1.35 |
| 3 | Glutaraldehyde | 10 | 20.30 | 1.16 | 19.90 | 1.20 | 20.30 | 1.34 |
| Sodium hypochlorite | 10 | 19.40 | 0.84 | 19.00 | 0.82 | 19.00 | 0.82 |
| Microwave | 10 | 15.70 | 1.57 | 16.00 | 1.33 | 16.50 | 2.12 |
(n: sample, SD: Standard deviation)
Vickers microhardness for disinfection and tooth interaction.
| Tooth | Control (n=10) | Glutaraldehyde (n=20) | Sodium hypochlorite (n=20) | Microwave (n=20) |
|---|
| Mean | SD | p | Mean | SD | p | Mean | SD | p | Mean | SD | p |
|---|
| Acryrock | 16.27 | 0.41 | - | 15.88 | 0.51 | 0.601 | 16.17 | 0.47 | 0.988 | 15.10 | 1.28 | 0.002* |
| Newace | 17.87 | 0.53 | - | 17.17 | 0.88 | 0.249 | 17.43 | 0.65 | 0.654 | 16.53 | 1.38 | 0.004* |
| Ivoclar | 20.50 | 0.59 | - | 19.82 | 1.02 | 0.564 | 19.38 | 0.78 | 0.154 | 17.78 | 2.13 | 0.001* |
Test applied: Two-way ANOVA and Tukey test; SD: Standard deviation, n: sample,
p<0.05: statistically significant
Vickers microhardness means for cycle and disinfection interaction.
| Cycle | Control (n=30) | Gluteralde- hyde (n=30) | Sodium Hypochlorite (n=30) | Microwave (n=30) |
|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD |
|---|
| 1 | 18.21 | 1.84 | 17.41 | 1.74 | 17.77 | 1.62 | 17.72 | 1.62 |
| 3 | 18.21 | 1.84 | 17.83 | 1.95 | 17.56 | 1.34 | 15.22 | 1.39 |
| Cycle 1 vs 3 (p-value) | - | 0.379 | 0.584 | <0.001* |
Test applied: Two-way Anova and Tukey test; SD: Standard deviation, n: sample,
p<0.05: statisti-cally significant
The comparison among disinfections showed that for Acryrock and Newace, the surface microhardness after disinfection with hypochlorite was significantly higher than that of microwave and glutaraldehyde disinfection. For Ivoclar, microhardness following glutaraldehyde disinfection presented statistically significant higher values than hypochlorite and microwave irradiation. In all the three brands, control group had the highest microhardness value [Table/Fig-6].
[Table/Fig-7] reveals mean of the surface hardness following one microwave disinfection cycle was lower than control, glutaraldehyde and hypochlorite. Further, three cycles of microwave irradiation showed hardness values significantly lower than control, glutaraldehyde, and hypochlorite. Comparison among cycles revealed that tooth surface microhardness was significantly decreased only after three cycles of microwave disinfection (p<0.001).
Discussion
The hardness of acrylic resin teeth plays a crucial impact on comfort and superior quality of mastication by aiding in the maintenance of stable occlusal relationship over time. In the present study, the effect of disinfection methods (by chemicals and microwave energy) on hardness property of conventional and cross linked acrylic resin denture teeth were evaluated.
Different disinfection methods depicted varied effects on the surface microhardness of the teeth. Glutaraldehyde and sodium hypochlorite disinfection caused a decrease in microhardness of very small value of about 1 Vickers hardness number which is not significant. The results of our study can be corroborated with the results of the studies conducted by Azevedo A et al, da Silva FC et al, Davi LR et al and Campanha NH et al., [13,17-19]. They concluded that immersion of a denture base acrylic resin in 2% alkaline glutaraldehyde and 1% sodium hypochlorite disinfectant solutions resulted in no significant effect on hardness values. In the current study, 2% glutaraldehyde and 1% sodium hypochlorite concentrations were included as part of our experiment based on the previous study [6].
The greater decrease in the surface microhardness caused by microwave irradiation than chemical disinfection in all the brands can be reasoned by the additive actions of increased temperature and the plasticising effect of water. Temperature affects the rate at which polymer based materials absorb water [6]. Hydrolysis of ester bonds interfering with entanglement of polymer chains permits the relaxation of stresses incurred during polymerization [20]. Higher the temperature, higher is the water absorption by the specimens. The entire process produces change in the physical characteristics of the acrylic resin polymer and gradual deterioration of its structure in the long run [16].
In addition, microhardness of the teeth subjected to three-cycles of microwave irradiation significantly decreased the tooth surface hardness in comparison to the first cycle of disinfection (p < 0.05). This can be due to the vibration of water molecules 2 to 3 billion times a second, resulting in friction and ensuing thermal expansion of resin and subsequent acceleration of the ageing process and degradation of its polymer matrix [16,21]. The series of reactions produce absorption facilitating the movement of polymeric chains under load and subsequently reducing the hardness values [16,22]. Thus, the null hypothesis which stated that different disinfection methods would not cause any effects on the surface hardness of acrylic resin teeth of different commercial brands was rejected.
Microwave irradiation as the third disinfection measure was taken up as it is an excellent and contemporary alternative to chemical disinfection. As suggested by, the recommended protocol was used for microwave disinfection [6, 23, 24]. The specimens were irradiated in water as microwave disinfection of acrylic resin under dry conditions produced minute dimensional changes [25]. Further, the effectiveness of microwave disinfection in deactivating potentially harmful microorganisms is considerably enhanced in the presence of water [26]. In the current study, the duration of microwave disinfection is maintained at 3 minutes as previous studies have demonstrated that 3-minute microwave irradiation promote disinfection without causing dimensional change [23,24].
In our study, Ivoclar and Newace, conventional acrylic resin teeth exhibited the lesser amount of change in microhardness than Acryrock, a crosslinked acrylic resin teeth following chemical and microwave disinfection. These effects could be possibly attributed to higher levels of cross-linking leading to brittleness and a loss of toughness [27]. The results of our study corroborated with the results of previous study by Suwannaroop P et al., and Loyaga-Rendon PG et al., [27,28]. The commercial brands of teeth studied were randomly picked based on commercial availability for the ease of the experiment.
Vickers hardness test was used in the study inspite of the plethora of methods being available to determine hardness of dental materials. This can be attributed to the ease of operation as the calculations are independent of the size of indention [29]. Further, viscoelastic recovery of the diagonals after indentation was minimal which can be ascribed to the short time interval between making and reading the indentation [16]. The study was conducted only on the first layer of teeth as relevance of second layer comes into picture only when there is wearing away of first layer and in cases, where a significant occlusal adjustment may be required. The dimensions of the PVC cylinder facilitated embedment of the entire configuration of teeth and allowed adequate leverage for finishing the resultant acrylic specimens.
The clinical implication of this study is that the dentist could prescibe the type of disinfection for each commercial tooth type. It can also be useful in determining the clinical frequency of the disinfection keeping in mind the long term security of artificial tooth. Moreover, concentrations and periods of immersion of different disinfectants that can influence the acrylic resin tooth is a valuable aid during clinical practice.
Limitation
The major limitation of this study are that the long term effect on hardness was not considered. Secondly, effect on hardness of lingual surface and internal surfaces following disinfection must be investigated. Thirdly, the limit of safe concentration and duration of disinfection maintaining unaltered hardness of artificial teeth could not be determined. Fourthly and most significantly, the study has to be verfied in a clinical scenario wherein the effect of biofilm and cyclic loads on the hardness of tooth can be analysed. Additionally, future studies based on correlation between hardness and other variables such as tooth wear as well as the effect of disinfection on the hardness of newer technology based denture teeth material such as Interpenetration of Polymer Networks (IPN) can be suggested.
Conclusion
Within the limitations of this in vitro study, it was concluded that there is no significant difference in microhardness when the teeth are subjected to glutaraldehyde (2%) and sodium hypochlorite (1%) disinfection. Further, three cycles of three minute duration microwave disinfection procedure produced decrease in the microhardness of different types of artificial teeth.
(n: sample, SD: Standard deviation)
Test applied: Two-way ANOVA and Tukey test; SD: Standard deviation, n: sample,
*p<0.05: statistically significant
Test applied: Two-way Anova and Tukey test; SD: Standard deviation, n: sample,
*p<0.05: statisti-cally significant