Coronary artery disease is the leading cause of morbidity and mortality across the globe [1]. It is possible to identify the severity of coronary artery disease, with the help of coronary angiography, a gold standard for evaluation of coronary artery disease. Unfortunately, coronary angiography is an invasive procedure carrying along with it definite procedural risk [2], as well as cost. Traditional, anthropometric indices like body mass index, waist circumference, waist hip ratio, which are the major indicators of obesity, vary with immediate lifestyle, diet and respiratory movements. So, neck circumference and leg length are the new anthropometric indices, which have overcome the limitations in traditional anthropometric indices mentioned above, are potential external indicators of existing coronary artery disease [3-5]. These new anthropometric indices can help provide a non invasive, patient friendly method for prediction of coronary artery disease. Therefore, these parameters promise to be more reliable anthropometric indices of central obesity and asymptomatic coronary artery disease. These simple clinical parameters, if found useful can be simple and effective measures to prevent symptomatic coronary artery disease, thereby reducing hospital stay, morbidity and mortality.
Hence, the aim of the present study was to device a patient friendly, cheap, method to predict coronary artery disease using anthropometric indices like neck circumference and leg length and testing their correlation with angiographic severity assessed by narrowing of coronary arteries due to atherosclerosis.
Materials and Methods
The present study was a cross-sectional study including 48 patients. The study was conducted at Karnataka Institute of Medical Sciences, Hubballi, Karnataka, India. Study was conducted over a period of 45 days from 1st January 2015 to 15th February 2015. The study has been carried out after obtaining the clearance of Institutional Ethical Committee of Karnataka Institute of Medical Sciences.
Inclusion criteria: Patients who have undergone elective angiography for symptomatic coronary artery disease.
Choice of subjects: The patients who after undergoing elective angiography for symptomatic coronary artery disease were willing to be a part of study without any favour or prejudice.
The subjects were the patients admitted at the institute for undergoing elective coronary angiography. A total of 48 patients who underwent coronary angiography for evaluation of coronary artery disease, and were willing to be the part of the study were included in the study. The patients were initially examined. This sample size has been arrived at by considering 5% alpha error and 90% power of the test as per results of the pilot study conducted at our institute.
Coronary angiography was performed after explaining the procedure along with all the necessary pros and cons and obtaining the written informed consent. Scoring of severity of coronary artery disease was performed by the Jenkins’ scoring system [Table/Fig-1]. Jenkins’ scoring system was used as it is simple to use and different coronary artery disease scoring systems correlate with each other regardless of complexity of scoring [6]. The coronary circulation was divided into eight proximal segments as the distal segments were difficult to be quantified, and only the lesions in the proximal segments were scored.
Angiographic scoring [7].
| S. No. | Severity of Obstruction | Score |
|---|
| 1 | Normal coronaries | 0 |
| 2 | <50% stenosis of the luminal diameter | 1 |
| 3 | 50% - 74% stenosis | 2 |
| 4 | 75% - 99% stenosis | 3 |
| 5 | 100% obstruction | 4 |
The segments scored included:
Left main coronary artery
Left Anterior Descending (LAD) artery up to the junction of mid and distal third of the vessel
Proximal third of major septal branch of LAD
Proximal third of major diagonal branch of LAD
Circumflex (CFX) coronary artery up to junction of middle and distal third of the vessel
Proximal third of major obtuse marginal branch of CFX
Right Coronary Artery (RCA) up to and including origin of Posterior Descending Coronary Artery (PDA)
Proximal third of PDA
If posterior descending coronary artery was supplied by circumflex coronary artery, circumflex coronary artery lesions till origin of posterior descending coronary artery as well as right coronary artery lesions up to origin of the middle and distal third of the vessel were included. The percentage of narrowing of each of the coronary arteries was noted by maximal narrowing of particular artery in all the projections. The severity of coronary artery narrowing was graded as shown in [Table/Fig-1].
Neck circumference: Measured in the midway of the neck, between mid-cervical spine and mid-anterior neck, to within 1 mm, with a plastic tape calibrated weekly. In men with a laryngeal prominence, it was measured just below the prominence. All circumferences were taken with the subjects standing upright, the face bent laterally and shoulders relaxed.
Leg length: Examination, included measurement of height and sitting height (from which an estimate of leg length could be derived).
Statistical Analysis
The data were analyzed using software IBM–SPSS. Mean and standard deviation for each continuous variable was calculated. Comparison of the values in males and females was tested by unpaired t-test. The correlation between Jenkins’ score, neck circumference and leg length was tested by Karl Pearson’s correlation coefficient method.
Results
Our study included a total of 48 patients of which 25 of the study subjects were males and 23 were females. [Table/Fig-2] summarizes the values of neck circumference, leg length and Jenkin’s scores. Comparison of the values in males and females was tested by unpaired t-test. Mean neck circumference was 36.87 cm (±4.37 cm) among males, 36.04 cm (±3.65 cm) among females and 36.44 cm (±3.99 cm) when combined together. There was no significant difference between males and females. Mean leg length among the study population was 88.70 cm (±2.51 cm) among males, 79.04 cm (±4.32 cm) among females and 83.66 cm (±3.26 cm) overall. The leg length was significantly more in males when compared to females. Similarly, mean Jenkin’s score was 4.43 (±2.94) in males, 4.96 (±1.81) in females and 4.70 (±2.40) overall. Jenkin’s score were not significantly different in males and females.
Comparison between males and females with respect to neck circumference, leg length and Jenkin’s score.
| Variable | Gender | n | Mean | SD | 95%CI | t-value | p-value |
|---|
| -95% | +95% |
|---|
| Neckcircumference(cm) | Male | 25 | 36.87 | 4.37 | 34.98 | 38.76 | 0.7161 | 0.4776 |
| Female | 23 | 36.04 | 3.65 | 34.54 | 37.54 |
| Leg length (cm) | Male | 25 | 88.70 | 2.51 | 87.61 | 89.78 | 9.3646 | <0.001* |
| Female | 23 | 79.04 | 4.32 | 77.26 | 80.82 |
| Jenkin’s score | Male | 25 | 4.43 | 2.94 | 3.17 | 5.70 | -0.7523 | 0.4557 |
| Female | 23 | 4.96 | 1.81 | 4.21 | 5.71 |
p<0.05, unpaired t-test
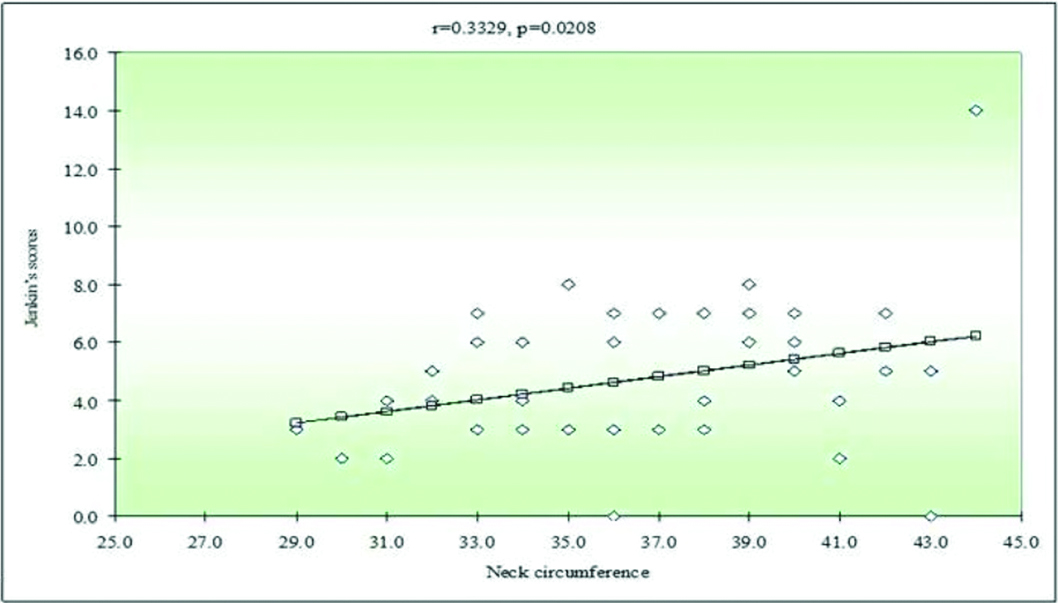
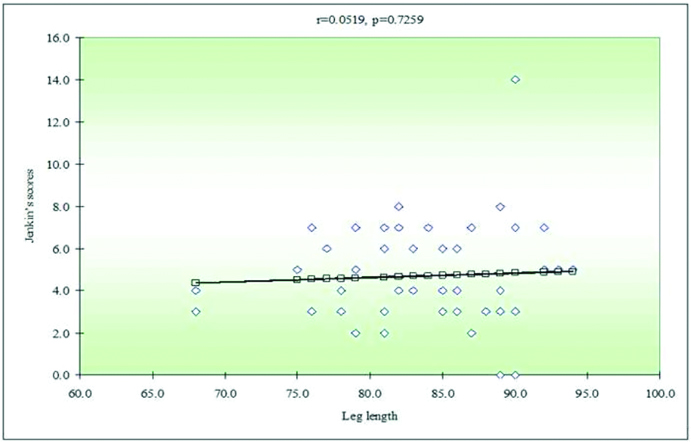
The correlation between neck circumference, leg length and Jenkin’s scores was tested by Karl Pearson’s correlation coefficient method. There was significant correlation between Jenkin’s scores and neck circumference. We can see the linear correlation in the graph [Table/Fig-3]. But, there was no correlation between Jenkin’s scores with leg length. The same has been depicted in the graph below [Table/Fig-4].
Correlation between Jenkin’s score and neck circumference.
Correlation between Jenkin’s score and leg length.
Discussion
We have found neck circumference to be correlating with coronary angiographic severity scoring in our study. Several others studies conducted in different countries have found different results. The study by Zen V et al., which was conducted on the patients who had significant coronary artery disease defined by the presence of stenosis equal to or greater than 50% in a major epicardial coronary artery (left anterior descendent, circumflex or right coronary artery), or their branches with or at least 2.5 mm of diameter presenting with Class – I and II stable angina. Control patients were those who did not present with significant coronary artery disease at coronary angiography. The study concluded that, excess of adiposity, centrally distributed or not, and accumulated in the neck that increased the neck circumference was significantly associated with coronary stenosis, even after control of body mass index; however, not associated with the extent of coronary artery disease, as measured by the number of vessels with at least 50% stenosis [8].
A study done by Silventoinen K et al., concluded that, “Risk of coronary heart disease in adulthood is inversely related to height at ages 7 to 13 years, but strongest in the youngest, and, independently here of, the risk increased by growth velocity” [9]. A study conducted by Chagas P et al., where, patients underwent coronary angiography for suspected coronary artery disease concluded that, there was no correlation between neck circumference and atherosclerotic burden. Study also mentions that none of the anthropometric indices is an independent risk factor for coronary atherosclerotic burden [10].
In a study by Preis SR et al., where sex-specific linear regression models were used to assess the association between SD increase in neck circumference and cardiovascular disease risk factors, neck circumference correlated with visceral adipose tissue. The study concluded that: neck circumference was associated with coronary vascular disease risk factors even after adjustment for visceral adipose tissue and body mass index [11].
In a cross-sectional study by Onat A et al., neck circumference correlated with numerous risk factors, viz., body mass index, waist girth and insulin resistance. Sex and age-adjusted neck circumference was associated significantly with metabolic syndrome, at a 2-3 fold increased risk at first standard deviation. Thus, concluded that neck circumference contributes to metabolic syndrome, which is an established aetiology for coronary artery disease [12].
There is a study conducted by Ben-Noun L and Laor A, which indicated indirect correlation between increase in neck circumference and coronary artery disease, where changes in neck circumference positively correlated with changes in some factors of the metabolic syndrome and, therefore, are correlated with changes in the risk of cardiovascular disease. The results indicated a significant association between changes in neck circumference and changes in body mass index, waist circumference, waist to-hip ratio. Thus, it concluded that changes in neck circumference are positively correlated with changes in some factors of the metabolic syndrome and, therefore, are correlated with changes in the risk of cardiovascular disease [13].
A study by Lawlor DA et al., concluded that shorter stature, shorter leg length, and trunk length were all associated with coronary heart disease in age adjusted analyses [14].
A prospective, population based, birth cohort study of 1472 participants, conducted by Langenberg C et al., in England, Scotland and Wales mentions, “short height and leg length are associated with increased pulse pressure and systolic blood pressure, but not diastolic blood pressure, in middle-aged men and women. Pulse pressure is a potential mediator between short height and leg length and increased risk of coronary heart disease” [15]. Other studies, conducted earlier mention that short stature not only is an important influence on the development of coronary heart disease in an asymptomatic healthy population but also an influence on the prognosis in men with prevalent coronary heart disease [5,10,14,15]. This is inconsistent with our results, where we do not find significant correlation of leg length with Jenkins’ score.
Limitation
The sample size was small. The severity of coronary atherosclerosis was assessed by Jenkin’s method, which does not take into account atherosclerosis of the distal part of coronary arteries. Hence, the total atherosclerotic burden is probably not reflected by this method.
Conclusion
Neck circumference correlates with Jenkin’s score of coronary angiographic severity and may be considered a surrogate marker of severity of atherosclerosis in an individual. It can be a simple, cheap and non invasive method for risk stratification of coronary heart disease.
*p<0.05, unpaired t-test