A Unique Triad of Muscular, Vascular and Nervous Variations in Upper Limb
Dharmaraj Wamanrao Tamgire1, Yogesh Ashok Sontakke2, SSSN Rajasekhar3, Karuppusamy Aravindhan4
1 Assistant Professor, Department of Anatomy, JIPMER, Pondicherry, India.
2 Assistant Professor, Department of Anatomy, JIPMER, Pondicherry, India.
3 Assistant Professor, Department of Anatomy, JIPMER, Pondicherry, India.
4 Additional Professor and Head, Department of Anatomy, JIPMER, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dharmaraj Wamanrao Tamgire, Department of Anatomy, Ground Floor, JIPMER Academic Center, JIPMER, Gorimedu-605006, Pondicherry, India.
E-mail: dtamgire@gmail.com.
Multiple muscular and neurovascular anomalies in upper limb are reported continuously in medical literature because of their clinical significance. A unique case of the triad of variations was encountered during routine dissection activity. The variations observed were: 1) Accessory third head of biceps brachii; 2) High division of Brachial Artery; 3) Communication between Musculocutaneous Nerve and Median Nerve. Taken independently these variations are common but it is rare in a single cadaver. These abnormalities were found unilaterally on the right arm of the cadaver. The third head of biceps brachii was seen to be originating from the medial border and adjacent area on the anteromedial surface of the humerus at the level of insertion of coracobrachialis fusing with main muscle belly just before it forms the tendon. Additional head of biceps brachii was supplied by a branch from the Median Nerve. This branch after supplying the additional head of biceps was seen to join the Musculocutaneous Nerve.
Further, a higher bifurcation of brachial artery was observed at the level of insertion of coracobrachialis. The medial division was traced distally as radial artery and the lateral division was traced as ulnar artery. The knowledge of these variations is of immense importance to correlate abnormal displacement of fractured bone segments, avoiding fatal injuries to vital structures, transradial angiography and diagnostic clinical neurophysiology.
Biceps brachii, Brachial artery, Communications, Median nerve, Musculocutaneous nerve
Case Report
Present anomalies were observed in the right arm of an adult male cadaver during routine dissection activities at JIPMER, Pondicherry. Each of the anomalous arteries, nerve and muscle, were carefully dissected from their origin to termination on both the limbs following the steps described in Cunningham’s Manual of Practical Anatomy [1].
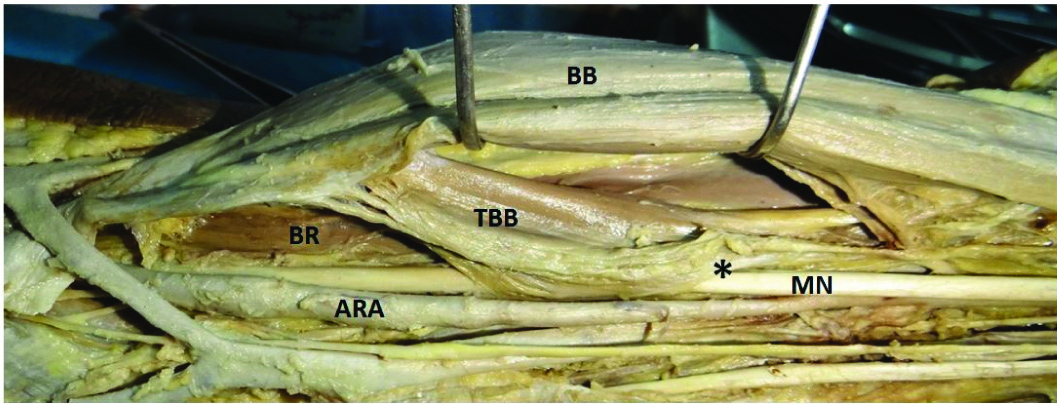
The third head of biceps brachii was seen to be originating from the medial border and adjacent area on the anteromedial surface of humerus at the level of insertion of coracobrachialis. Few fibres were also seen arising from medial intermuscular septum approximately 5 cms inferior to insertion of corachobrachialis. These two sites were connected by a fibrous arch, which in turn was giving origin to muscle fibres of anomalous third head which was seen fusing with main muscle belly just before it forms the tendon. Median nerve along with an artery (brachioulnar artery) was passing deep to the fibrous band [Table/Fig-1].
Showing Third Head of Biceps Brachii (TBB). ARA- Anomalous Radial Artery (Brachioradial Artery), BB- Biceps Brachii, BR- Brachioradialis, MN- Median Nerve, *- Fibrous Arch. Median Nerve seen passing deep to the arch.
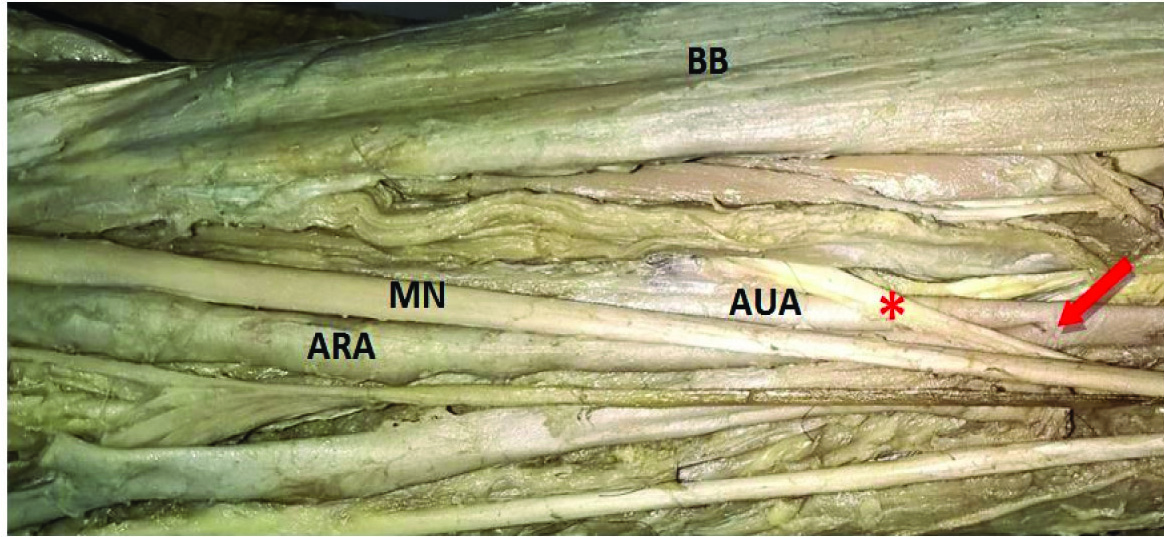
Brachial artery bifurcated into medial branch (Brachioradial Artery) and lateral branch (Brachioulnar Artery) distal to the origin of profunda brachii and nutrient artery, at the level of insertion of coracobrachialis. Lateral branch was seen passing posterolateral to median nerve deep to the fibrous arch of the anomalous third head of biceps brachii and then between biceps brachii and brachialis. Continuing posterolateral relation to median nerve at the level of cubital fossa it was observed passing deep to the ulnar head of pronator teres. This division traced distally was following the usual course, relations and branches of ulnar artery and was named likely. The medial branch at its origin was posteromedial to the median nerve. Passing downwards, it becomes medial to the nerve. At the cubital fossa, artery crossed the nerve anteriorly from medial to lateral. Traced distally it was seen accompanying superficial branch of the radial nerve and was following the normal course, relations and branches of the radial artery and was labelled likewise [Table/Fig-2] just above apex of cubital fossa the radial and the ulnar arteries crossed each other with median nerve between them.
Division of Brachial Artery (BA) (Red Arrow), ARA- Anomalous Radial Artery (Brachioradial Artery), AUA-Anomalous Ulnar Artery (Brachioulnar Artery), BB- Biceps Brachii, MN- Median Nerve, *- Communicating branch from the Median Nerve.
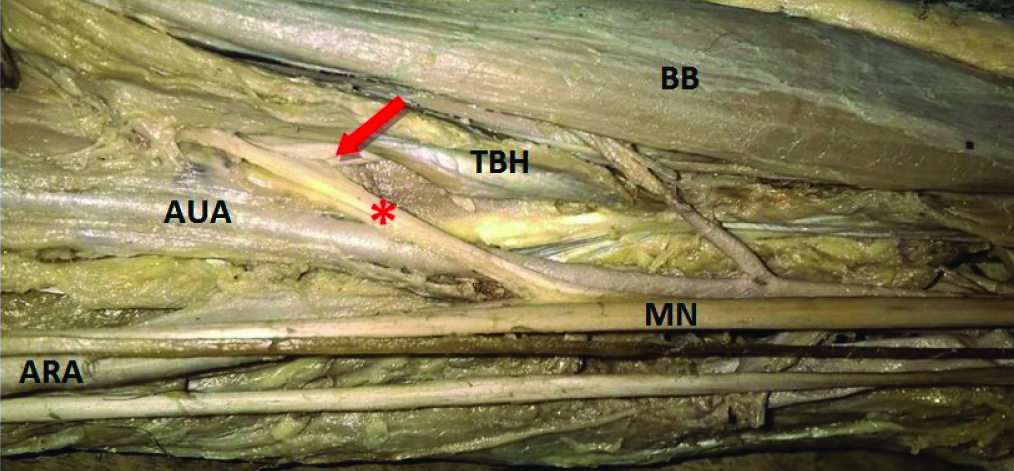
The third head of biceps brachii received nerve supply from a branch of median nerve. This branch of median nerve communicated with the musculocutaneous nerve after supplying the third head of biceps brachii [Table/Fig-3]. A very peculiar sequence of structures from lateral to medial was observed at cubital fossa [Table/Fig-4]:
Communicating branch from the Median Nerve (MN) to Musculocutaneous Nerve (Red Arrow), Third Head of Biceps Brachii (TBB). ARA- Anomalous Radial Artery (Brachioradial Artery), AUA- Anomalous Ulnar Artery (Brachioulnar Artery), BB- Biceps Brachii, MN- Median Nerve.
Structures seen at Cubital fossa from lateral to medial 1. Brachioradialis, 2. Radial Nerve, 3. Brachialis, 4. Musculocutaneous Nerve, 5. Tendon of Biceps Brachii, 6. Ulnar Artery, 7. Median Nerve, 8. Radial Artery, 9. Pronator teres.

Brachioradialis
Radial nerve
Brachialis
Musculocutaneous nerve
Tendon of biceps brachii
Ulnar artery
Median nerve
Radial artery
Pronator teres
Discussion
Reports of combination or isolated muscular, vascular and nervous anomalies in upper limb are continuously reported in medical literature [2-14]. In the present case, we report the third head of biceps brachii, the high division of brachial artery and communication between musculocutaneous nerve and median nerve. A similar type of cases of multiple anomalies involving biceps brachii, brachial artery and median nerve were also reported by Wadhwa S et al., and Vollala VR et al., [2,3] with minor differences in presentations [Table/Fig-5].
Previously reported and present studies involving muscular, vascular and neural anomalies in upper limb.
| Sr. No. | Authors | Anomalies |
|---|
| Muscular | Vascular | Nervous |
|---|
| 1. | Wadhwa S et al., [2] | Axillary Arch | Variant Superficial Brachial Artery, High anomalous origin of Common Interosseous Artery and a Superficial Ulnar artery | Absence of Musculocutaneous Nerve |
| 2. | Vollala VR et al., [3] | Third head of Biceps Brachii, Accessory head of Flexor Pollicis Longus and variant insertion of Pectoralis Major | Superficial Ulnar Artery, persistent Median Artery and variant Superficial Palmar Arch | Absence of Musculocutaneous Nerve |
| 3. | Sawant SP [5] | Third Head of Biceps Brachii | Normal Brachial Artery passing posterior to Third Head of Biceps Brachii | Normal Median Nerve piercing the Third Head of Biceps Brachii |
| 4. | Daimi SR et al., [7] | Additional Tendinous insertion of Biceps Brachii | Normal | Normal |
| 5. | Aharinejad S et al., [10] | Not commented | High bifurcation of Brachial Artery | Not commented |
| 6. | Madhyastha S et al., [11] | Not commented | High bifurcation of Brachial Artery.Abnormal course of Ulnar and Radial ArteryAbnormal origin of Profunda Brachii from Posterior Circumflex Humeral Artery | Not commented |
| 7. | Present case (2017) | Third Head of Biceps Brachii with anomalous fibrous arch. | High division of Brachial artery.Brachioulnar Artery passing deep to anomalous fibrous arch. | Communication between Musculocutaneous and Median Nerve.Median Nerve passing deep to anomalous fibrous arch. |
Multiple variations in muscles, vessels and nerves occurring simultaneously in one limb reinforce the concept that unusual development of one system of the limb frequently occurs in conjunction with another system. Upper limb myogenesis being an integrated process involving myocytes and nerves, and parallel pathways responsible for differentiation of vessels and nerves may explain such concurrence [15].
Biceps brachii is one of the flexor muscle of arm with two heads of origin and one of the commonest muscles of upper limb to present with variation in the form of an accessory head. Several studies in human beings show that the occurrence of third head of biceps brachii ranges from 0.25% to 37.5% [4,5,7,8]. Important finding in the present case is fibrous arch giving origin to third head of biceps brachii which overlie the median nerve and anomalous ulnar artery which is not reported by any other researcher earlier. Such atypical fibrous arches are common sites of abnormal nerve and arterial compression giving rise to signs and symptoms similar to Carpal Tunnel or Pronator Syndrome. Different types of fibrous arches involving anomalies of biceps brachii and capable of producing compression symptoms were also reported by Sawant SP and Mahato N [5,6]. The knowledge of such anatomical variations has gained significant attention because of newer precise imaging techniques like CT scan and MRI. It is important for orthopaedic surgeons while operating traumatic fractures of humerus involving middle third, distal extensions of anterior surgical approaches to shoulder joint and to correlate abnormal displacement of a fractured segment of bone [7]. Unusual structures encountered during surgery may confuse the surgeon that may lead to fatal injuries to vital structures.
The arterial system variations in the upper limb are common and encountered in approximately 25% of cases. Most of them are involving the brachial artery in the arm which continues in the forearm. Typical high division of brachial artery can be described as a division in the middle third of the arm where the two divisions of the vessel run parallel up to elbow joint and then proceed as normal radial and ulnar artery [8]. Present variation can be described as the same. The terminology used in naming the abnormal vessels in arm is confusing. According to Rodriguez-Niedenfuhr M et al., they can be termed as brachioradial and brachioulnar arteries in the arm [9]. Similar types of arterial variations were also noted by Aharinejad S et al., and Madhyastha S et al., [10,11]. In current case the brachioulnar artery passes deep to anomalous fibrous arch of accessory head of biceps brachii which is not reported by any earlier studies.
Knowledge of vascular anomalies of the upper limb is important for anatomists, surgeons, orthopaedic surgeons, radiologist, interventional radiologists, cardiologists and other medical and paramedical workers. Abnormal division and course of the arteries of arm and forearm can easily be misunderstood with vein leading to accidental injection of some drugs causing gangrene which may result in amputation of hand or fingers and it may be at the risk of accidental cut leading to alarming haemorrhage during surgery. Difficulties may arise while measuring the blood pressure or while preparation of free forearm flap or during trans-radial angiography where a radial artery has to be traced up to its origin. Such variations are also responsible for high failure rate or decrease the functional potency of arteriovenous fistulas.
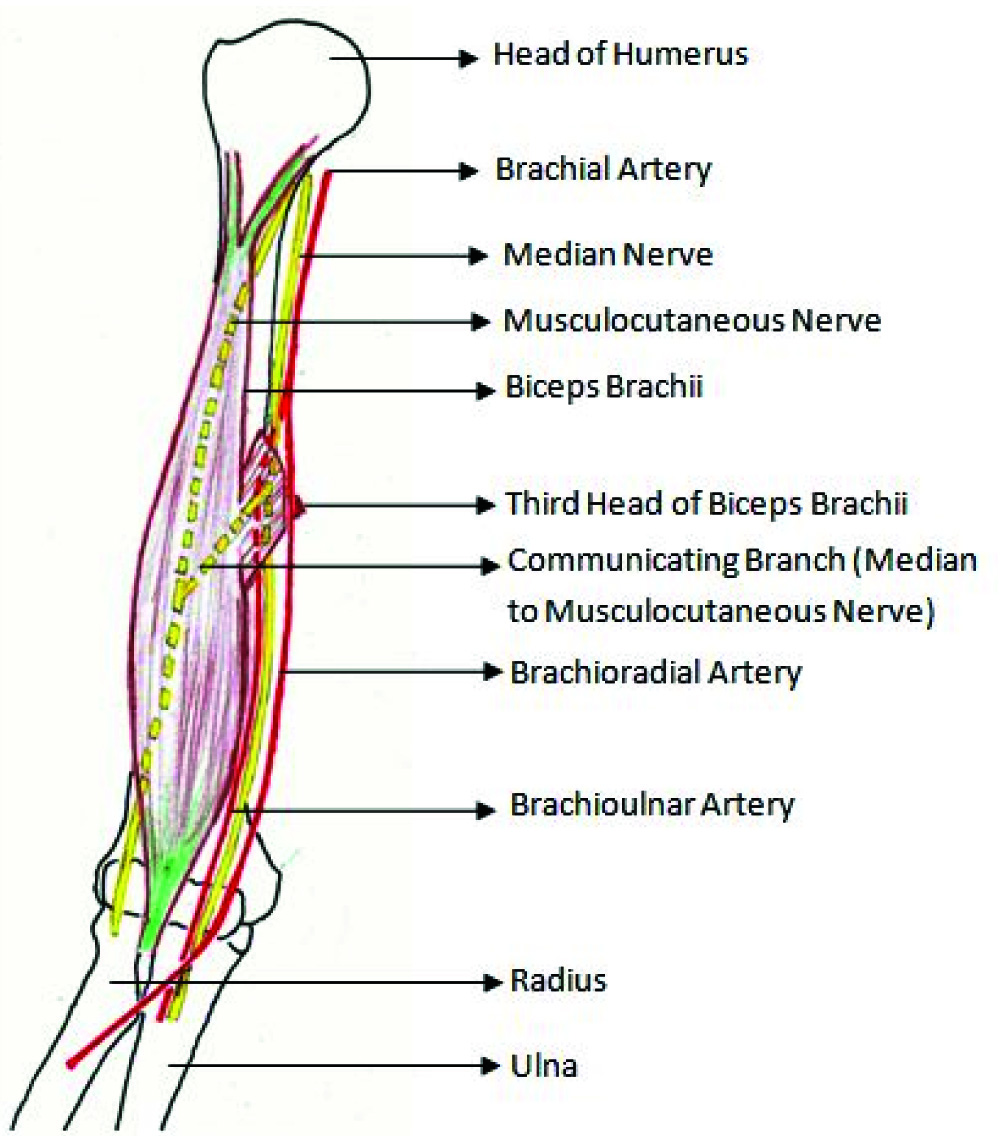
The incidence of communication between musculocutaneous and median nerve as observed by various researchers is ranging from 1.4 % to 33.3%. [12] There are countless possible scenarios of these communications which make it difficult to classify them in a comprehensive manner. Le Minor JM organised these communications in five types, Type I to Type V [13]. The current case does not fit into any type of Le Minor JM classification. Venierators D et al., classified these communications into three types in relation to coracobrachialis muscle, Type I communication is proximal to the entrance of musculocutaneous nerve into coracobrachialis, Type II is distal to the muscle and in Type III neither nerve nor its branch pierces the muscle [14]. The present case follows type II presentation of communication being distal to the muscle. Communicating branches may explain unusual presentation of nerve injury. The aberrant branch can accidently be damaged during any surgical procedure involving the arm region. Abnormal course, branches and communications of nerves of upper limb are important in diagnostic and clinical neurophysiology. Schematic representation of current case is shown in [Table/Fig-6].
Schematic representation of present case. (Note Third Head of Biceps Brachii, High bifurcation of Brachial Artery, communication branch from Median Nerve)
Conclusion
Knowledge of accessory muscles, overlying fibrous arch and anomalous vessels may be considered in differential diagnosis of neurovascular entrapment syndromes. Such variations need to be ruled out before labelling them as abnormal on CT and MRI scan. Awareness regarding such variation is valuable during preparation of free forearm flap, transradial angiography and during diagnostic and clinical neurophysiology investigations.
[1]. Romanes GJ, Cunningham’s Manual of Practical Anatomy 1986 15th EditionNew YorkOxford University Press [Google Scholar]
[2]. Wadhwa S, Vasudeva N, Kaul JM, A rare constellation of multiple upper limb anomaliesFolia Morphol 2008 67(4):236-39. [Google Scholar]
[3]. Vollala VR, Nagabhooshana S, Bhat SM, Potu BK, Rodrigues V, Pamidi N, Multiple arterial, neural and muscular variations in upper limb of a single cadaverRomanian Journal of Morphology and Embryology 2009 50(1):129-35. [Google Scholar]
[4]. Silva DA, Goke K, Savedra CMS, Pires LAS, Leite TFO, Chagas CAA, Variations of the biceps brachii muscle in BraziliansInternational Journal of Anatomy and Research 2016 4(2):2444-49. [Google Scholar]
[5]. Sawant SP, The neurovascular compression due to the third head of biceps brachii in the right arm – a case reportIJAPBS 2013 2(1):56-60. [Google Scholar]
[6]. Mahato N, Entrapment of the median nerves and brachial arteries in the lower arm bilaterally and additional origin of biceps brachii muscle. Case reportInt J Morphol 2010 28(4):1241-44. [Google Scholar]
[7]. Daimi SR, Siddiqui AU, Wabale RN, Gandhi KR, Additional tendinous insertion of Biceps Brachii: A Case ReportPravara Med Rev 2010 2(1):16-18. [Google Scholar]
[8]. Bergman RA, Thompson SA, Afifi AK, Saadeh FA, Compendium of human anatomic variation 1988 BaltimoreUrban & Schwarzenberg [Google Scholar]
[9]. Rodriguez-Niedenfuhr M, Vasquez T, Nearn L, Ferreira B, Parkin I, Sannudo JR, Variations of the arterial pattern in the upper limb revisited: a morphological and statistical study, with a review of the literatureJ Anat 2001 199:547-66. [Google Scholar]
[10]. Aharinejad S, Nourani F, Hollensteiner H, Rare case of high origin of the ulnar artery from the brachial arteryClin Anat 1997 10(4):253-58. [Google Scholar]
[11]. Madhyastha S, Nayak SR, Krishnamurthy A, D’costa S, Jose AA, Bhat MR, Case report of high origin of radial, ulnar and profundabrachii arteries, its clinical implications and review of the literatureJ Vasc Bras 2009 8(4):374-78. [Google Scholar]
[12]. Master NT, Gupta DS, Analysis of the morphological variations between musculocutaneous nerve and median nerve -a cadaveric studyIndian Journal of Clinical Anatomy and Physiology 2016 3(3):326-31. [Google Scholar]
[13]. Le Minor JM, A rare variation of the median and musculocutaneous nerves in manArch Anat Histol Embryol 1990 73:33-42. [Google Scholar]
[14]. Venieratos D, Anagnostopoulou S, Classification of communications between the musculocutaneous and median nervesClinical Anatomy 1998 11(5):327-31. [Google Scholar]
[15]. Herrena CGA, Tonkin MA, Oberge CK, Embryology and classification of congenital upper limb anomaliesLaub D, Congenital Anomalies of the Upper Extremity: Etiology and Management [Internet] 2015 [cited 27th December 2016] New YorkSpringer PublicationsPage no. 11, 14. Available from: https://books.google.co.in/books?id= [Google Scholar]