The success of an endodontic treatment depends on proper diagnosis, adequate shaping and cleaning and lastly complete three-dimensional obturation of the root canal system. According to the Washington study of endodontic success and failures, incomplete obturations have led to nearly 60% of endodontic failures [1]. Introduced in 1914 by Callahan, gutta-percha has universally been accepted as the gold standard for obturating materials [2]. However, due to the shrinkage of the sealer between its interfaces with gutta-percha and dentin, there was absence of complete seal [3].
The initial version of silicon-based sealers was called RoekoSeal (Coltene/Whaledent, Altstatten, Switzerland). Guttaflow 2 is an enhanced version of RoekoSeal, which is a cold-flowable, self-curing material, composed of gutta-percha powder with particle size of less than 30 μm, polydimethylsiloxane, and nanosilver particles. It produces a better seal, good adaptability and flowability with a slight expansion of 0.2% on setting, supplementing its adaptation to root dentin walls [4].
The most recent advancement in endodontic obturating materials takes advantage of the hydrophilic polymer plastic: C-point and Smartpaste Bio (Endo Technologies, LLC, Shrewsbury, MA, USA). This system consists of obturation points made up of a polyamide core composed of two therapeutic nylon polymers: Trogamid T and Trogamid CX with an external bonded hydrophilic polymer coating and an accompanying bioceramic containing Smartpaste Bio sealer. This hydrophilic coating permits swelling up of the points sideways resulting in self sealing of the root canal. It also expands laterally by utilizing the inherent moisture present in the instrumented root canal system.
This study compared the ability of different materials to effectively seal the apical one third of the root canal since it is vulnerable to microbial leakage under scanning electron microscope [5].
Materials and Methods
Specimen Selection
This in-vitro study was done in the Department of Conservative Dentistry and Endodontics, Yerela Medical Trust and Dental college, Mumbai, Maharashtra, India, in the month of March 2015.
In this study, 60 human mandibular premolar teeth that were extracted for periodontal and orthodontic reasons were selected. With the help of software G*Power analysis version 3.1.9.2 for the power 0.95 and α error probability 0.05, sample size of 20 for each group was determined. Single rooted mandibular teeth with single root canal and apical foramen were selected for the study. Radiographs were taken in both mesiodistal and buccolingual direction to rule out any calcifications, resorptions, extra canals and curvature of the root canal, internal and external resorptions, root caries and open apices. All teeth with such variations were excluded from this study.
Sample Preparation
The samples were decoronated with a diamond disk under water and the root lengths were standardized to 15 mm. A #10 K-file (Kerr, Romulus, MI) was placed in the canal until noticeable at the apex and pulled back 1 mm to determine the working length. Cleaning and shaping till rotary Pro-Taper file (Dentsply Maillefer) size F3 using crown down technique was carried out [6].
After each instrument, the canals were irrigated with 2 ml of 5% sodium hypochlorite (NaOCl) with 27-gauge side venting needles (R.C. Tweens, Prime Dental) inserted 3 mm from the apex. RC Help (Prime Dental, India) was used as a lubricant throughout the procedure. All the samples were rinsed with 5 ml of 5% NaOCl (1 minute), and flushed with 5 ml of 17% aqueous ethylenediaminetetraacetic acid (Dent Wash, Prime Dental, India) (1 minute) after complete instrumentation. The irrigants were passively activated by EndoActivator system (Advanced Endodontics, Santa Barbara, CA). The Endo-Activator device was used with short vertical movements in an “up and down” motion for 30 seconds (25.04). Final irrigation was done with saline solution. The canals were dried with paper points size 25.06 (Meta Biomed). After root canal preparation, the specimens were divided into three groups (N = 20).
Canal Obturation
Bouillaguet S et al., stated that the use of single-cone technique allowed a comparison of all the materials under relatively standardized conditions [7]. All the specimens were obturated with ProTaper size F3 cone.
In Group A, teeth were obturated with gutta-percha size F3 and AH Plus.
In Group B, teeth were obturated with C-point size F3/Smartpaste Bio.
In Group C, teeth were obturated with gutta-percha size F3/ guttaflow 2.
In Group A, the tip of the master gutta-percha cone size F3 was coated with AH Plus sealer and slowly inserted inside the canal till the full working length. Excess gutta-percha cone was seared off with a hot hand plugger (0.5 mm diameter, Dentsply Maillefer)
In Group B, Smartpaste Bio preloaded syringe sealer (Endo Technologies, LLC, Shrewsbury, MA, USA) was inserted deeply into the root canal with an intracanal tip into the apical portion. The root canal was filled with the sealer while withdrawing the intracanal tip coronally. C-point size F3 was coated with the sealer and inserted into the canal upto the working length. Excess of C-point was trimmed using a high speed handpiece with a diamond bur.
In Group C, the tip of the prefitted master gutta-percha cone size F3 was lightly coated with guttaflow 2 sealer and inserted into the canal using up and down motion until it reached to the full working length. Excess gutta-percha was seared off till the canal orifice using a hot hand plugger.
After obturation the specimens were stored in an incubator for 48 hours at room temperature and 100% humidity to allow for the complete setting of the sealer. Later, superficial longitudinal grooves were made along the mesial and distal wall of the root using the diamond disc with slow speed hand piece. The teeth were split into two halves using chisel and mallet. Scanning Electron Microscope (500 X) was used to access the interface between obturating material and dentin at the level of 3 mm from the apex.
Statistical Analysis
The results were statistically analyzed by using one-way analysis of variance (ANOVA) and ‘t test’. All analyses were performed using SPSS software version 17.0. One-way ANOVA test revealed that the probability of this study (p value), assuming the null hypothesis is less of <0.01, indicating that the result was statistically significant.
Results
Group A (control) showed a mean difference of 8.54 as compared to 5.76 in Group C.
In Group B, the mean difference of 0.83 was observed which was the least as compared to the other groups. The standard deviation of Group B was 0.45 as compared to 1.09 as seen with Group C.
The t test showed (p<0.001) statistically significant results. The mean-wise comparison of the microgap between the three groups showed a statistical difference [Table/Fig-1].
t test showing Mean and SD values of the microgap exhibited by the specimens
| Group data | N | Mean | Std. Deviation | Std. Error Mean | p value |
|---|
| GP + AH PlusC Point + Smartpaste Bio | 2020 | 8.5385.8330 | .9434.45051 | .21097.10074 | <.001 |
| GP + Guttaflow 2 | 20 | 5.7600 | 1.09513 | .24488 | |
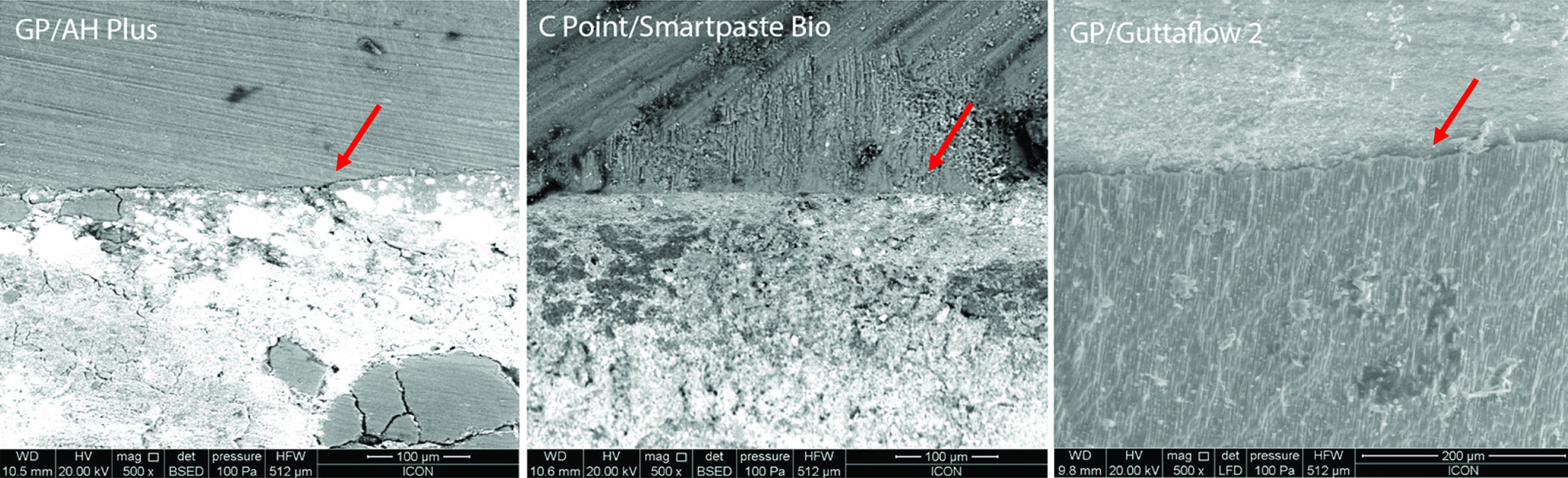
Group A (gutta-percha/AH plus) showed poor adhesion of the obturating system to the dentinal walls as well as gutta-percha to sealer in the apical third.
Group B (C-point/Smartpaste Bio) showed good adhesion to dentinal wall with a smooth contact line on the sealer-dentine interface.
Group C (gutta-percha/guttaflow 2) showed increased microgap as compared to Group B.
According to SEM findings [Table/Fig-2], the samples of Group B showed least microgap values with a maximum of 1.56 μm as compared to Group C, which resulted in a maximum of 7.38 μm microgap at the apical one third of the root canal.
SEM (500X) of the micro-gap in apical one third of the root canal. GP/AH Plus (control)-voids at the sealer-GP and sealer dentin interface. C Point/Smartpaste Bio-close adaptation and penetration of sealer into dentinal tubules. GP/Guttaflow 2-showed few voids and inability to bond to the dentin.
*GP=gutta-percha
Discussion
The conservation of the periapical tissues ensures the success of the root canal treatment [8]. Materials along with different techniques of cleaning and shaping are capable of uniformly filling the entire root canal system.
According to Gordon MP et al., single-cone obturation of root canals has recently been resuscitated with the introduction of greater taper master cones that closely match the geometry of nickel-titanium instrumentation system [9]. Tay FR et al., also stated that with the advent of contemporary root canal sealing systems that claim to create bonds along the sealer-gutta-percha interface via refinement of the sealer or the root filling material also support the use of a single-cone obturation technique[10].
The bio-acoustic effect of EndoActivator irrigation produced sonic activation that led to the disinfecting agents being transported deeper into the dentinal tubules causing bacterial death[11]. Thus, the specimens were prepared till ISO size 30/0.06 for irrigants to reach the apical portion of the root canal.
The major demerit evaluated with gutta-percha was its inability to reinforce endodontically treated teeth [12,13]. gutta-percha does not chemically bond to the dentin wall hence, does not fulfill the ideals of monoblock system. According to Teixeira FB et al., AH plus, a resin-based sealer, does not form a monoblock due to its lack of bonding to the gutta-percha [14]. Furthermore, due to the hydrophobicity of the gutta-percha cones, the sealer tends to pull away on setting [15]. For guttaflow 2, the manufacturer claims that the sealer expands 0.2% on setting. This expansion enhances the sealer flow into the dentinal tubules initiating a seal that is comparable to that of gutta-percha and AH Plus sealer. However, guttaflow 2 also showed poor wetting on the root dentin surface because of the presence of silicone, perhaps producing a high surface tension force, making the spreading of these materials more difficult [16].
To overcome the disadvantages of hydrophobic systems and to elevate the consequences of the treatment, hydrophilic obturating systems was inculcated. The C-point system imparts the points with the elasticity that allows it to easily gauge around any curvatures in the biomechanically prepared canal. The outer polymer layer is a copolymer of acryl-o-nitrile and vinyl-pyrrole, cross-linked using allyl methacrylate and a thermal initiator. The moisture and dihydrogen monoxide present within the instrumented canals form a hydrogen bond with the existing polar locations, thus causing lateral enlargement inside the polymeric chains. This expansion is well ordered as part of the manufacturing course. The C-point showed an approximately 17% expansion after 20 minutes [17,18]. Smartpaste Bio is a resin-based sealer proposed to swell up, by the addition of ground polymer. The inclusion of bioceramics into the sealer produces calcium hydroxide and hydroxyapatite as byproducts, giving it exceptional dimensional stability, biocompatibility and antibacterial properties inside the root canal. Thus, hydrophilic obturating system exhibited close compliance, penetration of sealer into the dentinal tubules and less microgap values as compared to the hydrophobic system.
Studies have illustrated that scanning electron microscope has an exorbitant depth of field, higher resolution and finer magnification at the interface [19]. The SEM uses electromagnets rather than lenses thereby, amplifying magnification and facilitating clear images. Regarding the entity of experimental groups of the present study, a tendency towards better values for C-point with Smartpaste Bio is observed as compared to guttaflow 2 automix and AH plus. This can be attributed to the hydrophilic polymeric endodontic point, which takes advantage of water-impelled, radial expansion to adapt to the canal irregularities [20].
The outcome of our study come to support those of previous authors, despite methodological variations conducted by De-Deus G et al., who found that guttaflow resulted in a few samples contaminated by human saliva than AH plus [21]. Hegde V and Arora S compared the sealing ability of a novel hydrophilic vs. conventional hydrophobic obturation systems and concluded that hydrophilic system showed better resistance to bacterial leakage as compared to Resilon/Epiphany system, and gutta-percha/AH plus in a single cone technique [22].
Limitation
The major limitations of this in-vitro study were the lack of reproducibility of in-vivo conditions. The influence of remaining moisture content in the dentinal tubules after the final irrigation and drying of the canal will have different results with respect to hydrophobic and hydrophilic obturating materials. To compare the influence of biomechanical preparation and irrigation protocol, randomized and double-blind clinical studies are needed to confirm the long term success of bioceramic materials.
Conclusion
The conception of creating mechanically homogenous units to form “ideal monoblocks” in the root canal space has been attempted with the introduction of hydrophilic materials. C point with Smartpaste Bio produced a greater dentinal adaptation with less microgap formation at the sealer-dentin interface as compared to the conventional hydrophobic systems. The study concluded a greater efficiency of this obturating material to penetrate the dentinal tubules and produce a 3D seal. Further, in vitro or in vivo studies with a follow up should help confirm the current results.