Osteoma of the Middle Turbinate Presenting with Frontal Lobe Abscess and Seizure
Ramandeep Singh Virk1, Shikhar Sawhney2
1 Associate Professor, Department of ENT and Head and Neck Surgery, PGIMER, Chandigarh, India.
2 Resident, Department of ENT and Head and Neck Surgery, PGIMER, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shikhar Sawhney, 126 Civil Lines, Friends Colony, Bareilly-243001, Uttar Pradesh, India.
E-mail: shikhar.sawhney@gmail.com
Osteomas are the most common benign tumours of the sinonasal tract. Even though their location in the sinuses is well known, turbinate osteomas are quite rare. We report one such case of a 26-year-old female who presented with neurological complaints of a seizure rather than nasal complaints. The cause of the seizure was found to be a small abscess in her frontal lobe, secondary to frontal sinusitis due to a bony hard nasal mass arising from the middle turbinate. She underwent endoscopic excision of the mass which was confirmed on histopathology as an osteoma. The case highlights an unusual presentation of a middle turbinate osteoma.
Benign tumours, Neoplasm, Sinusitis
Case Report
A 26-year-old female presented to the Department of Neurosurgery with a history of headache & fever since two weeks. She also gave history of a single episode of seizure. She further complained of recurrent episodes of nasal discharge and nasal blockade on the left side and gradually progressive protrusion of the left eye since last few years but denied any complaints of decreased visual acuity or double vision. She had undergone a surgery eight years back on the eye for the same but the details of the surgery were not known as no records were available.
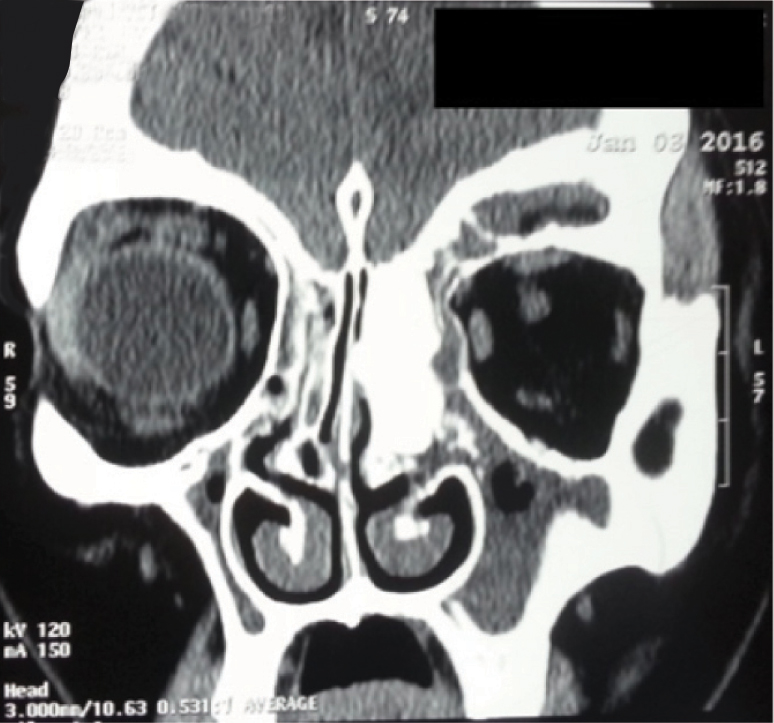
An ENT consultation was sought in view of these complaints. Nasal endoscopy revealed an enlarged left middle turbinate which was bony hard in consistency. There was mild proptosis on the left side. Visual acuity was normal. Bilateral pupils were normally reacting and there was no restriction of extra-ocular movements. MRI brain revealed breach of posterior wall of left frontal sinus with mild dural enhancement along left frontal bone and a 10 x 7 mm peripherally enhancing lesion in the left frontal lobe suggestive of an abscess. Non Contrast CT of the nose and paranasal sinuses showed a bony dense enlargement of the left middle turbinate occluding the drainage of the frontal sinus [Table/Fig-1]. There was hyperostosis of the frontal bone. Also, noted was a breach in the roof of the orbit.
Preoperative non contrast CT scan showing the osteoma causing blockage of frontal sinus drainage.
In view of the very small size of the abscess, it was decided to manage it conservatively with i.v. antibiotics and anticonvulsants only. She was started on Inj. ceftriaxone 2 gm BD, Inj. vancomycin 1gm BD and Tab levetiracetam 500 mg TDS.
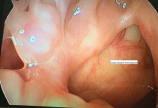
Two weeks later, she was taken up for endoscopic sinus surgery after obtaining a well informed consent for the procedure. Mucosa over the bony swelling was debrided [Table/Fig-2]. The swelling was drilled in the upper part near its attachment at the skull base using a curved frontal burr. Tumor was freed from all attachments by a periosteal elevator and cut at its superior most attachment after adequate thinning by drilling. After the specimen was delivered, adequate frontal sinusotomy was done. Within the sinus, isolated islands of ill formed bone were found which were removed using giraffe forceps.
Intraoperative endoscopic picture of the mass visualized;

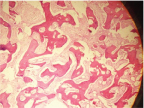
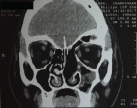
Histopathological examination of the specimen showed a bony lesion having a trabecular as well as well-formed lamellar bone with prominent osteoblastic rimming which was consistent with osteoma [Table/Fig-3]. Postoperative course was uneventful. Patient has been on a regular follow up in the OPD since then. Nasal endoscopic examination at nine months showed well mucosalized, healed cavity with wide fontal sinus opening [Table/Fig-4]. A nine month postoperative non contrast CT of Paranasal Sinus (PNS) showed clearance of the osteoma with wide drainage pathway [Table/Fig-5].
Photomicrograph of the specimen showing bony trabeculae and fibrous stroma. (H&E staining. 10X).
Nasal endoscopic picture at nine month follow-up: well healed cavity and broad frontal sinus opening;
Nine month postoperative NCCT PNS showing clearance of the osteoma with broad draining cavity.
Discussion
Osteomas are benign, slow growing osteoblastic lesions and the most common benign tumours of the sinonasal tract [1]. However, they are usually asymptomatic and are found co-incidentally in patients undergoing CT for sinus symptoms. Occasionally though, they present with symptoms of headache, nasal discharge, epiphora, forehead swelling, ocular pain etc. They are most frequently found in frontal sinus, followed by ethmoid, maxillary, and more rarely the sphenoid sinus [1]. It is highly unusual to find an osteoma in the nasal cavity per se. We have presented herein, a case of middle turbinate osteoma presenting as headache and a single episode of seizure, along with history of long standing nasal obstruction.
Osteomas are usually diagnosed between the 2nd to 5th decades [1]. According to Fu YS and Perzin KH, osteomas are histologically divided into 3 categories: ivory osteoma (lobulated, made of compact dense bone containing minimal amount of fibrous tissue), mature osteoma (consisting of spongy, mature bone with conspicuous fibrous tissue) and mixed osteoma (with findings of both ivory and mature osteoma) [2]. Association has been seen between osteomas and the occurrence of Gardner syndrome, a genetic disorder characterized by multiple polyps of the colon in association with osteomas of the skull and multiple soft tissue tumours [3].
They have a slight male preponderance according to the literature however, nasal cavity osteomas reported till date has been seen more commonly in females. Whittet HV and Quiney RE first reported an osteoma of the middle turbinate in 1988 which was removed by a lateral rhinotomy approach [4]. Till date, only nine middle turbinate, one superior turbinate and five inferior turbinate osteomas have been reported [Table/Fig-6] [4-18].
Literature review of turbinate osteomas.
| S. No. | Author | Year | Age/Sex | Presentation | Approach |
|---|
| Middle Turbinate: |
| 1 | Whittet HB & Quiney RE [4] | 1988 | 31/F | Nasal obstruction | Lateral Rhinotomy |
| 2 | Lin CJ [5] | 2003 | 73/M | Nasal obstruction, facial pain, epiphora | Modified Lynch |
| 3 | Viswanath B [6] | 2008 | 14/F | Facial pain, nasal obstruction | Lynch |
| 4 | Migirov L [7] | 2009 | 65/F | Headache, nasal obstruction | Refused treatment |
| 5 | Kutluhan A [8] | 2009 | 31/M | Headache, facial pain | Craniofacial resection |
| 6 | Daneshi A [9] | 2010 | 41/F | Nasal obstruction, epiphora | Endoscopic |
| 7 | Yadav SP [10] | 2013 | 30/M | Nasal obstruction | Lateral rhinotomy |
| 8 | Endo M [11] | 2014 | 13/M | Nasal obstruction | Gingival incision |
| 9 | Ciftci Z [12] | 2015 | 50/F | Headache, Nasal obstruction | Endoscopic |
| Inferior Turbinate: |
| 1 | Mesolella M [13] | 2005 | 54/F | Nasal obstruction | Endoscopic |
| 2 | Viswanath B [14] | 2010 | 24/F | Nasal obstruction | Endoscopic |
| 3 | Kumar KK [15] | 2010 | 54/F | Nasal obstrucyion | Endoscopic |
| 4 | Grabovac S [16] | 2012 | 50/M | Nasal obstruction | Sublabial |
| 5 | Sahamey R [17] | 2016 | 60/F | Bilateral nasal obstruction | Endoscopic |
| Superior Turbinate: |
| 1 | Ishimaru T [18] | 2005 | 61/F | Headache | Endoscopic |
Osteomas are usually asymptomatic given their slow growing nature and diagnosed co-incidentally on radiology performed for other reasons. They tend to cause symptoms like headache, nasal obstruction, discharge etc. when they start to impinge on the surrounding structures causing a mass effect. In our case, the middle turbinate osteoma was the cause for frontal sinusitis which possibly resulted in bony remodeling which in turn led to the development of proptosis. Infection breaching the posterior table of frontal sinus explained the development of frontal lobe brain abscess and seizure. Although paranasal sinus osteomas are known to cause obstructive intracranial symptoms, to our knowledge turbinate osteomas presenting with such symptomatology has not yet been reported.
Because of the slow growing nature of these tumors, there is a general consensus in favour of a “wait and watch” policy for their treatment provided, there are no symptoms and the lesion does not encroach critical structures like optic nerve/orbit. Assessment is best done by a CT scan of the nose, paranasal sinuses and the orbit to identify the site of attachment and gauge the extent of the lesion. Differential diagnosis of nasal osteoma can include other fibro-osseous lesions like fibrous dysplasia and ossifying fibroma. They may have similar radiographic appearance, but their borders are less well-defined than those of osteomas [19].
Surgical approaches can be either purely endoscopic, external approaches including fronto-ethmoidectomy using Lynch-Howarth incision, midfacial degloving, lateral rhinotomy, Caldwell-Luc or osteoplastic flap approach and combined external and endoscopic approach. Cavitation is a surgical trick where in the core of the lesion is drilled with a cutting burr, leaving a very thin shell that can be easily fractured and dissected off [20]. The mass in our case was amenable for a purely endoscopic resection so it was delivered en-bloc endoscopically itself, however, piece meal removal of osteoma in case of difficulty in gaining access has also been described. Recurrences in osteomas are rare. Patients are usually followed up with regular endoscopic examinations and imaging done in case of a clinical suspicion.
Conclusion
Turbinate osteomas are a rare entity. When left undiagnosed, they may present with intracranial complications like meningitis, brain abscess etc., as described in our case. A careful history taking and detailed otorhinolaryngological work up will help to pick up such rare presentations early and prevent complications.
[1]. Eller R, Sillers M, Common fibro-osseous lesions of the paranasal sinusesOtolaryngol Clin North Am 2006 39:585-600. [Google Scholar]
[2]. Fu YS, Perzin KH, Non-epithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx. A clinicopathologic studyCancer 1974 33:1289-305. [Google Scholar]
[3]. Alexander AA, Patel AA, Odland R, Paranasal sinus osteomas and Gardner’s syndromeAnn Otol Rhinol Laryngol 2007 116:658-62. [Google Scholar]
[4]. Whittet HB, Quiney RE, Middle turbinate osteoma; an unusual cause of nasal obstructionJ Laryngol Otol 1988 102:359-61. [Google Scholar]
[5]. Lin CJ, Lin YS, Kang BH, Middle turbinate osteoma presenting with ipsilateral facial pain, epiphora, and nasal obstructionOtolaryngo Head Neck Surg 2003 128:282-83. [Google Scholar]
[6]. Viswanatha B, Middle turbinate osteomaIndian J Otolaryngol Head Neck Surgery 2008 60:266-68. [Google Scholar]
[7]. Migirov L, Drendel M, Talmi YP, Osteoma in an aerated middle nasal turbinateIsr Med Assoc J 2009 11:120 [Google Scholar]
[8]. Kutluhan A, Salviz M, Bozdemir K, Deger HM, Culha I, Ozveren MF, Middle turbinate osteoma extending into anterior cranial fossaAuris Nasus Larynx 2009 36:702-04. [Google Scholar]
[9]. Daneshi A, Jalessi M, Heshmatzade-Behzadi A, Middle turbinate osteomaClin Exp Otorhinolaryngol 2010 3:226-28. [Google Scholar]
[10]. Yadav SP, Gulia JS, Hooda A, Khaowas AK, Giant osteoma of the middle turbinate: a case reportEar Nose Throat J 2013 92(4-5):E10-12. [Google Scholar]
[11]. Endo M, Tsukahara K, Nakamura K, Motohashi R, Suzuki M, A case of giant osteoma in the middle turbinate of a childJpn Clin Med 2014 5:15-18. [Google Scholar]
[12]. Ciftci Z, Deniz M, Celik O, Oznur M, Gultekin E, Middle turbinate osteoma causing migraine like SymptomsAustin J Otolaryngol 2015 2:1030 [Google Scholar]
[13]. Mesolella M, Galli V, Testa D, Inferior turbinate osteoma: a rare cause of nasal obstructionOtolaryngol Head Neck Surg 2005 133:989-91. [Google Scholar]
[14]. Viswanatha B, Inferior turbinate osteoma: case reportEar Nose Throat J 2010 89:227-31. [Google Scholar]
[15]. Kumar KK, Sumathi V, Sundhari V, Inferior turbinate osteoma - rare cause of nasal obstructionIndian J Otolaryngol Head Neck Surg 2010 62:332-34. [Google Scholar]
[16]. Grabovac S, Hadzibegovic AD, Markesic J, Inferior turbinate osteoma as a cause of unilateral nose obstructionColl Antropol 2012 36:189-91. [Google Scholar]
[17]. Sahemey R, Warfield AT, Ahmed S, Bilateral inferior turbinate osteomaJ Surg Case Rep 2016 8:1-3. [Google Scholar]
[18]. Ishimaru T, Superior turbinate osteoma: a case reportAuris Nasus Larynx 2005 32:291-93. [Google Scholar]
[19]. Ciniglio Appiani M, Verillaud B, Bresson D, Sauvaget E, Blancal JP, Guichard JP, Ossifying fibromas of the paranasal sinuses: diagnosis and managementActa Otorhinolaryngol Ital 2015 35:355-61. [Google Scholar]
[20]. Bignami M, Dallan I, Terranova P, Battaglia P, Miceli S, Castelnuovo P, Frontal sinus osteomas: the window of endonasal endoscopic approachRhinology 2007 45:315-20. [Google Scholar]