MRI Study on Spinal Canal Morphometry: An Indian Study
Maitreyee Kar1, Dipankar Bhaumik2, Kaushik Ishore3, Pallab Kumar Saha4
1 Associate Professor, Department of Anatomy, North Bengal Medical College, Siliguri, West Bengal, India.
2 Assistant Professor, Department of Anatomy, North Bengal Medical College, Siliguri, West Bengal, India.
3 Assistant Professor, Department of Community Medicine, North Bengal Medical College, Siliguri, West Bengal, India.
4 Assistant Professor, Department of Anatomy, North Bengal Medical College, Siliguri, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dipankar Bhaumik, Ambika Kundu Bye Lane, P.O. Santragachi, Howrah-711104, West Bengal, India.
E-mail: dipankarbhaumik@rediffmail.com
Introduction
A large proportion of adults suffer from neck pain at some points of their life and show altered ranges of spinal canal morphometry in various studies. The differences in values are also seen due to genetic, hormonal and other factors too. Torg’s ratio is a widely accepted measurement to eliminate such discrepancies. The measurement of Space Available for Cord (SAC) is also gaining importance as spinal stenosis is a contributor to neck pain.
Aim
(1) To examine the cervical spinal canal and spinal cord morphometric determinants in symptomatic sub-Himalayan North Bengal population and to compare the obtained data with other populations; (2) To determine whether Torg’s ratio vary with gender or not; (3) To determine SAC values in symptomatic individuals.
Materials and Methods
Magnetic Resonance Imaging (MRI) based on midsagittal diameter of vertebral body, spinal canal, spinal cord and its Torg’s ratio and SAC value of the lower cervical spine (C3-C7) from 71 symptomatic adults were recorded at the Radiology Department of North Bengal Medical College and Hospital, Bengal, India. Individuals with any evidence of trauma, infection, neoplasia or any congenital anomalies related to spinal canal and below 18 years of age were excluded from the study.
Results
The average diameter for vertebral body was significantly larger in males. The average diameter for spinal canal, spinal cord and values of Torg’s ratio and SAC has no significant gender difference. But the mean value of Torg’s ratio is greater in females is due to smaller vertebral body size in females.
Conclusion
It is interpreted from our study that sagittal spinal canal diameter, Torg’s ratio and SAC value did not show any significant gender difference. But sagittal vertebral body’s diameter showed sexual dimorphism which influenced the mean value of Torg’s ratio.
Cervical region, Space available for cord, Torg’s ratio
Introduction
Majority of adult population suffer from neck pain, frequently radiating to upper limbs, at some points of their life. Cervical spinal canal stenosis often predisposes to such problem. This condition is a narrowing of cervical spinal canal within vertebral column, which contains spinal cord and it’s covering meninges, meningeal blood vessels and spinal nerve roots [1]. This stenosis has long been considered as a predisposing factor for cervical spondylotic myelopathy related to cervical spondylosis and cervical neuropraxia related with trauma, degeneration and inflammation specially [2,3]. According to one study, 82% of people aged 54 years or above have radiologic evidence of degenerative changes in cervical spine [4].
Payne EE and Spillane JD measured anteroposterior diameter of adult cervical spinal canal in 1957 with the help of lateral radiographs [5]. Many studies were performed on different populations since then. These studies proposed different measurements of normal range of this diameter in different populations. These differences are not only due to genetic and hormonal factors, they are also due to magnification problems with plain X-ray. To overcome these discrepancies, Torg J et al., and Pavlov H et al., measured cervical spinal canal stenosis in a different way [6,7]. They used a ratio of sagittal spinal canal diameter divided by sagittal diameter of the corresponding vertebral body. This ratio became popular as Torg’s ratio or Pavlov’s ratio or canal to body ratio [8-9]. Sagittal cervical spinal canal diameter less than 13 mm and Torg’s ratio less than 0.80 are well accepted indicators of cervical spinal canal stenosis and carry the increased risk of neurologic injury [6,9-11].
Though, plain radiographs can well delineate osseous structures, they have limited abilities in delineation of soft tissue abnormalities and these abnormalities are important contributor of cervical spinal canal stenosis. In this context, MRI deserves special importance as it can detect not only abnormalities of both soft tissues and bones, it can measure spinal canal and spinal cord accurately too. Thus, MRI can accurately measure the SAC which is a product of difference between sagittal diameter of spinal canal and sagittal diameter of spinal cord (SAC = sagittal diameter of spinal canal minus sagittal diameter of spinal cord) [12,13]. The measurement of SAC has importance because spinal canal stenosis can be described as encroachment of spinal canal on the spinal cord.
To our knowledge, until recently, there has been no report or study monitoring the spinal canal morphometry in symptomatic sub-Himalayan population of Northern part of West Bengal. The first purpose of our study was aimed at establishing ranges of cervical spinal canal morphometry in symptomatic sub-Himalayan North Bengal population and to compare the acquired data with other population. Secondly, our study analyzes Torg’s ratio vary or not with gender in symptomatic subjects. Thirdly, to determine SAC values in symptomatic individuals.
Materials and Methods
A retrospective study done in North Bengal Medical College included 71 subjects aged between 18 to 70 years (average age 40.14 years, standard deviation 14.103). There were total 44 males and 27 females among these 71 subjects. All of these 71 individuals attended outpatient Department of Orthopedics with complaints of neck pain often radiating to upper limbs and few of them had paresthesia in the neck and upper limb too between May 2016 to October 2016. Individuals below the age of 18 years were excluded from this study. Individuals with any evidence of trauma, infection, neoplasia or any congenital anomalies related to spinal canal were excluded from the study. Measurements of sagittal diameter of vertebral body, spinal canal and spinal cord were taken for the study. The sagittal vertebral body was measured at the level of midpoints between superior and inferior endplates and the sagittal spinal canal diameter was measured as the distance from the midpoint of vertebral body posteriorly to the nearest point of spinolaminar line [7,14]. The sagittal spinal cord was measured at the appropriate vertebral body level transversely in the midline. The Torg’s ratio was determined by dividing the sagittal diameter of spinal canal by the sagittal diameter of vertebral body [6,7]. The SAC was determined by subtracting the sagittal cord diameter from corresponding sagittal canal diameter [Table/Fig-1] [14].
Midsagittal T2 weighted pulse sequence of cervical spine in 73-year-old man. Sagittal-diameter measurements of the spinal cord, spinal canal, and vertebral body.
3, 6, 9, 12, 15 = sagittal spinal cord diameter,
2, 5, 8, 11, 14 = sagittal spinal canal diameter;
1, 4, 7, 10, 13 = sagittal vertebral body diameter.

MRI was done with the help of 1.5 Tesla GE BRIVO 355 machine with a spinal coil and standardised neutral head position. T1-weighted and T2-weighted images were taken for MR imaging study. Sagittal T1-weighted Fast Spin Echo sequence (FSE) (repetition time m sec/echo time m sec, 539/11; section thickness, 4 mm; field of view, 240 mm x 240 mm; matrix, 320 x 256), sagittal T2- weighted turbo- spin echo sequence (2697/103; section thickness, 4 mm; insertion gap, 1 mm;) and a transverse T2-weighted Fast Recovery Fast Spin Echo (FRFSE) sequence at one or multiple levels (4597/104; section thickness, 4 mm; insertion gap, 0.5 mm; field of view, 200mm x 200 mm; matrix, 320 x224) was used for this purpose. All measurements were made in millimeters in presence of a radiologist and a mean value of three measurements was considered as the final measurement. All the measurements were made midsagittally at each spinal level from C3 to C7 vertebra.
Statistical Analysis
Student’s t-test was used as statistical test for significance. A p-value of 0.05 or less was considered as statistically significant. The statistical package IBM SPSS version 20.0 was used for all analysis.
Results
All measurements were taken at the level from C3 to C7 vertebrae in 71 individuals (44 males and 27 females) of 18 to 70 years of age (average age 40.14±14.103).
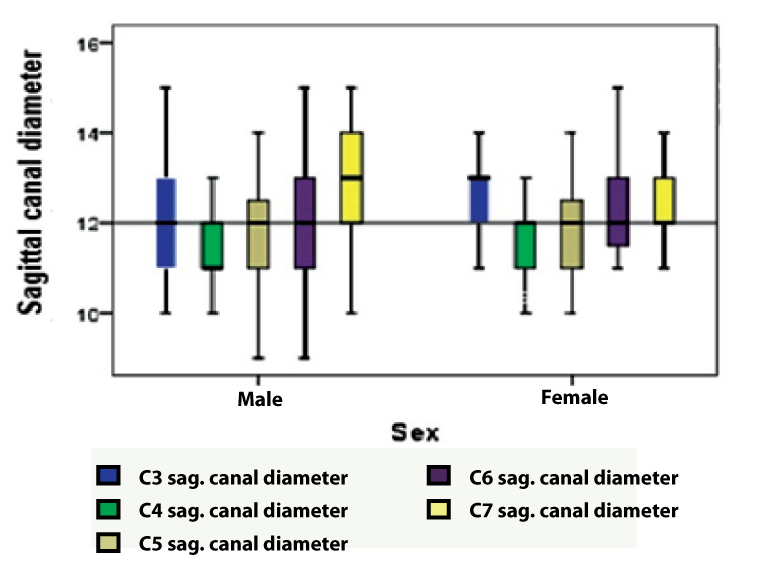
The average sagittal vertebral body diameter was 14.60±1.38 mm (average±standard deviation) in males and 13.04±1.13 mm in females. Males have a significantly larger sagittal vertebral bodies diameter than females (p<0.001). The average sagittal spinal canal diameter in males was 11.99±1.34 mm and that in females was 12.15±1.24 mm. There was no significant gender difference in sagittal spinal canal diameter (p=0.4611) [Table/Fig-2,3].
Interquartile ranges of sagittal canal diameters in males and females.
Gender wise distribution of mean values for different vertebral parameters.
| Different vertebral parameters | Gender | Student’s t-test value & p-value |
|---|
| Male (mean±SD) | Female (mean±SD) |
|---|
| Vertebral bodies diameter (mm) | 14.60±1.38 | 13.04±1.13 | t-value = 7.37p < 0.001 |
| Sagittal canal diameter (mm) | 11.99±1.34 | 12.15±1.24 | t-value = 0.74p = 0.461 |
| Sagittal spinal cord diameter (mm) | 7.15±0.80 | 6.93±0.84 | t-value = 1.60p = 0.112 |
| Torg’s ratio | 0.81±0.31 | 0.92±1.18 | t-value = 0.52p = 0.606 |
| SAC value | 4.84±1.47 | 5.22±1.38 | t-value =1.58p = 0.1169 |
The average sagittal spinal cord diameter in males was 7.15+0.80 mm and in females was 6.93+0.84 mm. Again there was no significant gender difference (p=0.1121).
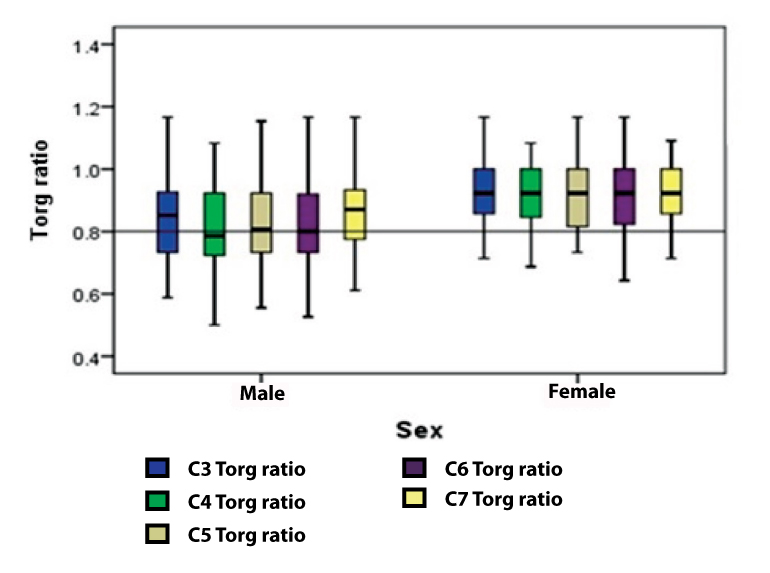
The Torg’s ratio in males ranged from 0.5 to 1.17 with a mean of 0.81+0.31. The same in females ranges from 0.64 to 1.36 with a mean of 0.92+1.18. The Torg’s ratio score shows no significant gender difference (p=0.6062). But the mean value of Torg’s ratio was greater in females due to smaller vertebral body size in females [Table/Fig-3,4].
Inter-quartile ranges of Torg ratios in males and females.
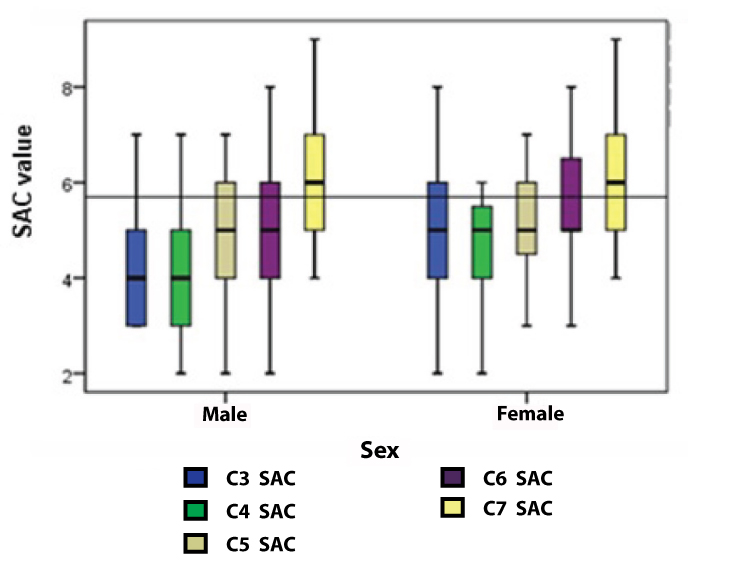
The SAC value in male ranges from 2 mm to 9 mm with a mean of 4.84+1.47 mm and in females also from 2 mm to 9 mm with a mean of 5.2+1.380 mm. There was no significant difference of SAC values between the sexes (p=0.1169) [Table/Fig-3,5].
Inter-quartile ranges of SAC values in males and females.
Discussion
Various postural, mechanical and genetic factors determine the growth of vertebral body and spinal canal in cervical region. Therefore, studies of vertebral canal shows racial and ethnic variation, apart from age and sex related differences in size. The space within spinal canal determines the movements of its contents without any jeopardy by tension and pressure. So, any abnormal reduction in the size of spinal canal, particularly in lower cervical vertebra, could predispose to neck pain. Since the work of Payne et al., on the relationship between the developing myelopathy and spinal canal size, many authors worked on diagnostic importance of sagittal spinal canal diameter, Torg’s ratio and SAC in cervical vertebral region [Table/Fig-6,7] [15-21]. Payne EE and Spillane JD have reported the normal mean midsagittal diameter of the cervical spinal canal (from C3 to C7 segments) in British population is 18.0 mm for males and 17.2 mm for females after measuring on lateral radiograph [5]. According to Boijsen E the differences of 1 mm to 4 mm in the measurement of sagittal diameter of vertebral body and spinal canal in different studies could be partly due to differences in techniques by various authors as they have used radiographs for investigation and partly due to variation in the body build of subjects (affecting the object-to-film distance or focus-to-film distance) [22]. To eliminate such discrepancies, MRI is used by different authors in recent days.
Comparison of sagittal spinal canal diameter and Torg’s ratio in different population [15-20].
| Author | Criteria | Sagittal spinal canal Diameter (in mm.) Mean±standard deviation/range | Torg’s ratio Mean±standard deviation/range |
|---|
| Macedonian study Matveeva N et al., [15] | MRI based study on asymptomatic population | 14.59±1.01 (male) 15.26±1.11 (female) | 0.89±0.09 (male) 1.1±0.11 (female) |
| Pakistanis Study Maqbool A et al., [16] | Dried specimen | 15.1±1.6 (male) 14.5±2.07 (female) | 0.95 (male) 1.08 (female) |
| Korean Study Lee HM et al., [17] | Dried specimen | 13.2 ± 1.3 (male) 13.1 ± 2.6 (female) | 0.93 ± 0.1 (male) 1.02 ± 0.09 (female) |
| USA Study Tierney TR et al., [14] | MRI based study on asymptomatic population | 13.28 ± 1.47 | 0.528-1.18 (range) |
| Turkey Study Karabulut O et al., [18] | Lateral plain radiograph based study on patients with neck pain | 13.71-15.21 (male) 12.78-14.68 (female) | 0.79-0.85 (male) 0.79-0.83 (female) |
| Nepal study Gupta M et al.,[19] | Radiograph based study on patients with neck pain | 18.19±2.09 (male) 17.41±1.47 (female) | 0.99 ± 0.09 (male) 1.01 ± 0.07 (female) |
| Indian Study Kathole MA et al., [20] | Radiograph based study on asymptomatic population | 16.06-16.93 (male range) 15.12-15.80 (female range) | 0.95-0.96 (male range) 1.06-1.08 (female range) |
| Our Study | MRI based study on patients with neck pain | 11.99±1.34 (male) 12.15±1.24 (female) | 0.81±0.31 (male) 0.92±1.18 (female) |
Comparison of SAC between different population [14,15,21].
| Author | Criteria | SAC value (in mm) Mean±standard deviation/range |
|---|
| Macedonean study Matveeva N et al., [15] | MRI based study on asymptomatic population | 6.47±0.94 (male) 7.04±1.28 (female) |
| Japan Study Oda T et al., [21] | MRI based study on myelopathy and nonmyelopathy population | 11.1 (in myelopathy group) 16.5 (in nonmyelopathy group) |
| Tierney TR et al., study [14] | MRI based study on asymptomatic population | 2.5-10.4 |
| Our study | MRI based study on patients with neck pain | 4.84±1.47 (male) 5.22±1.38 (female) |
Torg J et al., and Pavlov H et al., attempted to find a solution to these discrepancies and devised a “ratio method” that compares the sagittal diameter of the spinal canal with the anteroposterior width of the vertebral body both of which are equally affected by radiological magnification factors [6,7] and it is independent of magnification factors caused by differences in target distance, object-to-film distance, or body type [15]. Torg J et al., and Pavlov H et al., proposed a ratio of less than 0.80 is suggestive of significant spinal stenosis [6,7]. Usefulness of Torg’s ratio in the diagnosis of cervical spinal canal stenosis has also been confirmed by several other workers [7,9,23]. Lee HM et al., is of opinion that measurement of canal body ratio is superior to anteroposterior diameter of cervical spinal canal in diagnosis of spinal stenosis or predicting prognosis of cervical spinal cord injury [17]. Torg J et al., and Pavlov H et al., have reported that in American subjects studied by them, there is normally a one-to-one relationship between the sagittal diameter of the spinal canal and that of the vertebral body (i.e., Torg’s ratio = 1.00), regardless of the sex of the individual [6,7]. According to Lim’s study, Torg’s ratios in men are smaller than women as women had smaller sagittal canal diameters at all levels of the cervical spine [24], but men had larger vertebral bodies and the same is found in our study and other studies too [15,20].
The size of the cervical spinal canal and the space available for the cord are important determining factors to make decision on the therapeutic treatment in traumatic, degenerative, and inflammatory conditions of the cervical spine. A low SAC value increases risk of neurological injury and its recurrence [14]. Many research reports showed that less SAC values are associated with an increased risk of cervical-cord neuropraxia episodes [6,25]. Herzog RJ et al., recommended that SAC is of great importance if symptomatic individual had a Torg’s ratio less than 0.80 or a sagittal spinal-canal diameter value less than 12.5 mm [13].
MR imaging proved to be superior over plain X-ray radiograph, which was used by earlier research workers, for various morphometric measurements of spinal cord and canal. So plain X-ray radiograph based Torg’s ratio is a poor indicator of spinal stenosis compared to MRI based Torg’s ratio measurements. Again the Torg’s ratio depends less on spinal canal diameter than vertebral body diameter and males present more spread out sagittal canal diameters than females in some studies [15]. The SAC value has its importance here as it relies more on sagittal spinal canal diameter than sagittal vertebral body diameter. So less variability in spinal cord measurements are seen in SAC values. The head position of the subjects should be standardized as neutral because this affects the spinal cord’s size [26].
So, we hope that our findings on Indian population in this study will help all research workers and doctors to treat patients and perform different studies in future.
Limitation
Comparatively smaller number of the subjects is the main limitation of our study. We have used MRI for our study. So some soft tissue structures could have influenced these results.
Conclusion
From our study, it was found that sagittal vertebral bodies diameter shows sexual dimorphism. This diameter is significantly larger in males. Sagittal spinal canal diameter and sagittal spinal cord diameter have no significant gender difference. The mean value of sagittal spinal canal diameter was slightly smaller in our study population of sub-Himalayan West Bengal compared to most of the other studies. Again Torg’s ratio and SAC value did not show any significant gender difference but the mean value of Torg’s ratio is greater in females was due to smaller vertebral body size in females. We also determined a SAC value in this population and the mean value of SAC is also slightly smaller compared to other studies. We hope this might help to treat different clinical conditions among populations.
[1]. Standring S, Editor-in-chief, Gray's Anatomy. The Anatomical Basis of Clinical PracticeVertebral Column, Back 2016 41st Edition, International EditionElsevier Limited:714-720. [Google Scholar]
[2]. Edwards WC, LaRocca H, The developmental segmental sagittal diameter of the cervical spinal canal in patients with cervical spondylosisSpine (Phila Pa 1976) 1983 8:20-27. [Google Scholar]
[3]. Gore DR, Roentgenographic findings in the cervical spine in asymptomatic persons: a ten-year follow-upSpine (Phila Pa 1976) 2001 26:2463-66. [Google Scholar]
[4]. Jones ET, Mayer P, Turek's Orthopedics, Principles and Their Application 1994 5th edPhiladelpiaJ.B. Lippincott Company:345-6. [Google Scholar]
[5]. Payne EE, Spillane JD, The cervical spine: an anatomico-pathological study of 70 specimens (using a special technique) with particular reference to the problem ofcervical spondylosisBrain 1957 80:571-96. [Google Scholar]
[6]. Torg J, Pavlov H, Genuario S, Sennett B, Wisneski RJ, Robie BH, Neurapraxia of the cervical spinal cord with transient quadriplegiaJ Bone Joint Surg Am 1986 68(9):1354-70. [Google Scholar]
[7]. Pavlov H, Torg JS, Robie B, Jahre C, Cervical spinal stenosis: determination with vertebral body ratio methodRadiology 1987 164:771-75. [Google Scholar]
[8]. Castro FP, JrRicciardi J, Brunet ME, Busch MT, Whitecloud TS, Stingers, the Torg ratio, and the cervical spineAm J Sports Med 1997 25:603-08. [Google Scholar]
[9]. Meyer SA, Schulte KR, Callaghan JJ, Albright JP, Powell JW, Crowley ET, Cervical spinal stenosis and stingers in collegiate football playersAm J Sports Med 1994 22:158-66. [Google Scholar]
[10]. Song KJ, Choi BW, Kim SJ, Kim JH, Kim YS, Song JH, The relationship between spinal stenosis and neurological outcome in traumatic cervical spine injury: An analysis using Pavlov's ratio, spinal cord area and spinal canal areaClinics in Orthopedic Surgery 2009 1:11-18. [Google Scholar]
[11]. Torg JS, Naranja RT, JrPavlov H, Galinat BJ, Warren R, Stine RA, The relationship of developmental narrowing of the cervical spinal canal to reversible and irreversible injury of the cervical spinal cord in football playersJ Bone Joint Surg Am 1996 78(9):1308-14. [Google Scholar]
[12]. Torg JS, Corcoran TA, Thibault LE, Pavlov H, Sennett BJ, Naranja RJ, JrCervical cord neuropraxia: classification, pathomechanics, morbidity, and management guidelinesJ Neurosurgery 1997 87:843-50. [Google Scholar]
[13]. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ, Normal cervical spine morphometry and cervical spinal stenosis in asymptomatic professional football players: plain film radiography, multiplanar computed tomography, and magnetic resonance imagingSpine (Phila Pa 1976) 1991 16(suppl):178-86. [Google Scholar]
[14]. Tierney TR, Maldjian C, Mattacola GC, Straub JS, Sitler RM, Cervical spine stenosis measures in normal subjectsJ Athl Train 2002 37(2):190-93. [Google Scholar]
[15]. Matveeva N, Janevski P, Nakeva N, Zhivadinovik J, Dodevski A, Morphometric analysis of the cervical spinal canal on MRISec Med Sci 2013 XXXIV(2):97-103. [Google Scholar]
[16]. Maqbool A, Athar Z, Hussain L, Midsagittal diameter of cervical spinal canal and Torg's ratio of the cervical spine in PakistanisPak J Med Sci 2003 19(3):203-10. [Google Scholar]
[17]. Lee HM, Kim NH, Kim HJ, Chung IH, Mid-sagittal canal diameter and vertebral body/canal ratio of the cervical spine in KoreansYonsei Med J 1994 35(4):446-52. [Google Scholar]
[18]. Karabulut O, Karabulut Z, The variations of Torg ratio with gender in patients with neck painDicle Med J 2007 34(4):272-74. [Google Scholar]
[19]. Gupta M, Bharihoke V, Bhargava SK, Agarwal N, Size of vertebral canal – A correlative study of measurements in radiographs and dried bonesJ Anat Soc India 1998 47:01-06. [Google Scholar]
[20]. Kathole MA, Joshi RA, Herekar NG, Jadhav SS, Dimensions of spinal canal and vertebra and their relevance in clinical practiceInternational Journal Of Recent Trends In Science And Technology 2012 3(2):54-58. [Google Scholar]
[21]. Oda T, Yonenobu K, Fujimura Y, Ishii Y, Nakahara S, Matsunaga S, Diagnostic validity of space available for the spinal cord at C1 level for cervical myelopathy in patients with rheumatoid arthritisSpine (Phila pa 1976) 2009 34(13):1395-98. [Google Scholar]
[22]. Boijsen E, The cervical spinal canal in intraspinal expansive processesActa Radiol 1954 42(2):101-15. [Google Scholar]
[23]. Chen IH, Liao KK, Shen WY, Measurement of cervical canal sagittal diameter in Chinese males with cervical spondylotic myelopathyChung Hua I Hsueh Tsa Chih (Taipei) 1994 54(2):105-10. [Google Scholar]
[24]. Lim JK, Wong HK, Variations of the cervical spinal torg ratio with gender and ethnicityThe Spine Journal 2004 4:396-401. [Google Scholar]
[25]. Kelly JD, Aliquo D, Sitler MR, Odgers C, Moyer RA, Association of burners with cervical canal and foraminal stenosisAm J Sports Med 2000 28(2):214-17. [Google Scholar]
[26]. De Lorenzo RA, Olson JE, Boska M, Johnston R, Hamilton GC, Augustine J, Optimal positioning for cervical immobilizationAnn Emerg Med 1996 28:301-08. [Google Scholar]