Dental caries is a commonly occurring dental disease. The primary causative microorganisms responsible are Streptococcus mutans, Streptococcus salivarius, Streptococcus sobrinus, Lactobacillus etc. Research shows that the reduction in microorganisms causes a significant decrease in dental caries [1].
Mouth rinses are popularly used antimicrobial and anticariogenic solutions in dentistry for prophylactic and therapeutic purposes. Presently, a wide range of mouthrinses are available commercially, such as, CHX, sodium fluoride, etc. Mouth rinses should be able to differentiate the pathogenic microbes from the normal commensals of the oral cavity and selectively eliminate them [2].
CHX is a broad spectrum antimicrobial mouthrinse as a result of which it is widely preferred. However, according to Addy and Moran, CHX is associated with few side effects such as discoloration of teeth, irritation of mucosa, altered taste sensation, swelling of parotid, and increased supragingival calculus formation which limits its use as a therapeutic agent [3].
Recently, alternative medicine has gained popularity due to its herbal properties with no adverse effects. Amongst them, green coffee bean extract is receiving greater attention due to its antibacterial effect against both gram negative and positive bacteria [4]. Green coffee bean is the unroasted mature or immature robust coffee bean. It mainly comprises of Chlorogenic Acids (CGA), caffeine, trigonelline and the diterpenes cafestol and kahweol. Naturally, green coffee is a major source of Chlorogenic acid (CGA), 5–12 grams/100 grams [5]. Chlorogenic acids are naturally occurring polyphenolic compound. They possesses many health benefits like antibacterial, antifungal effect etc., [6].
To our knowledge limited studies on the anticariogenic effect of coffee are found in literature [7]. Thus the aim of the current study was evaluation of efficacy of green coffee bean extract against salivary Streptococcus mutans.
Materials and Methods
Study Subjects
According to the results of pilot study, 15 subjects in each group were required to provide 80% power of the study at 5% level of significance.
Thus sample size of 45 subjects, in the age group, ranging from 18-22 years was selected among the students of a dental institute.
Preparation of Mouth Rinses
The 2% Green coffee bean extract (S Therapeutics, An ISO: 9001-2008 and WHO GMP Certified Co.) was freshly prepared by dissolving 2 grams of the powder in 100 ml of distilled water. Commercially available 0.2% CHX (Rexidine, Warren, Indoco Remedies Ltd., India) was used as positive control, and Sterile water as negative control.
Study Design
A randomized parallel controlled clinical trial was conducted at Army College of Dental Sciences, Secunderabad, Telangana, India for a period of two weeks in the year 2016. The study protocol was reviewed and clearance was obtained by the Institutional Ethical Committee.
Before commencing the study, a preliminary examination was conducted using Decayed, Missing, and Filled Teeth (DMFT) index.
On the basis of simple random sampling, subjects who scored between 1.2 and 2.6 (low prevalence) were included into the study by obtaining written informed consent. Subjects who didn’t meet the criteria were excluded from the study. Inclusion and exclusion criteria used were as follows.
Inclusion Criteria
DMFT scores between 1.2 and 2.6
Should not have used mouth rinse for the last one month
Free from systemic diseases
Exclusion Criteria
History of antibiotic therapy in the previous one month till the start of the study
Currently using any mouth rinse or history of use of mouth rinse in the past one month
History of fluoride treatment in the past two weeks
The selected subjects were randomly divided into three groups of 15 each by lottery method, i.e., the name of the mouth rinse was written on the chits and subjects were asked to pick up the chits. The groups were as follows:
Group A - Study group: 2% Green coffee bean extract (Coffea Robusta) (S Therapeutics, An ISO: 9001-2008 and WHO GMP Certified Co.)
Group B - Positive control: 0.2 % CHX mouthwash
Group C - Negative control: Sterile water
Saliva Samples
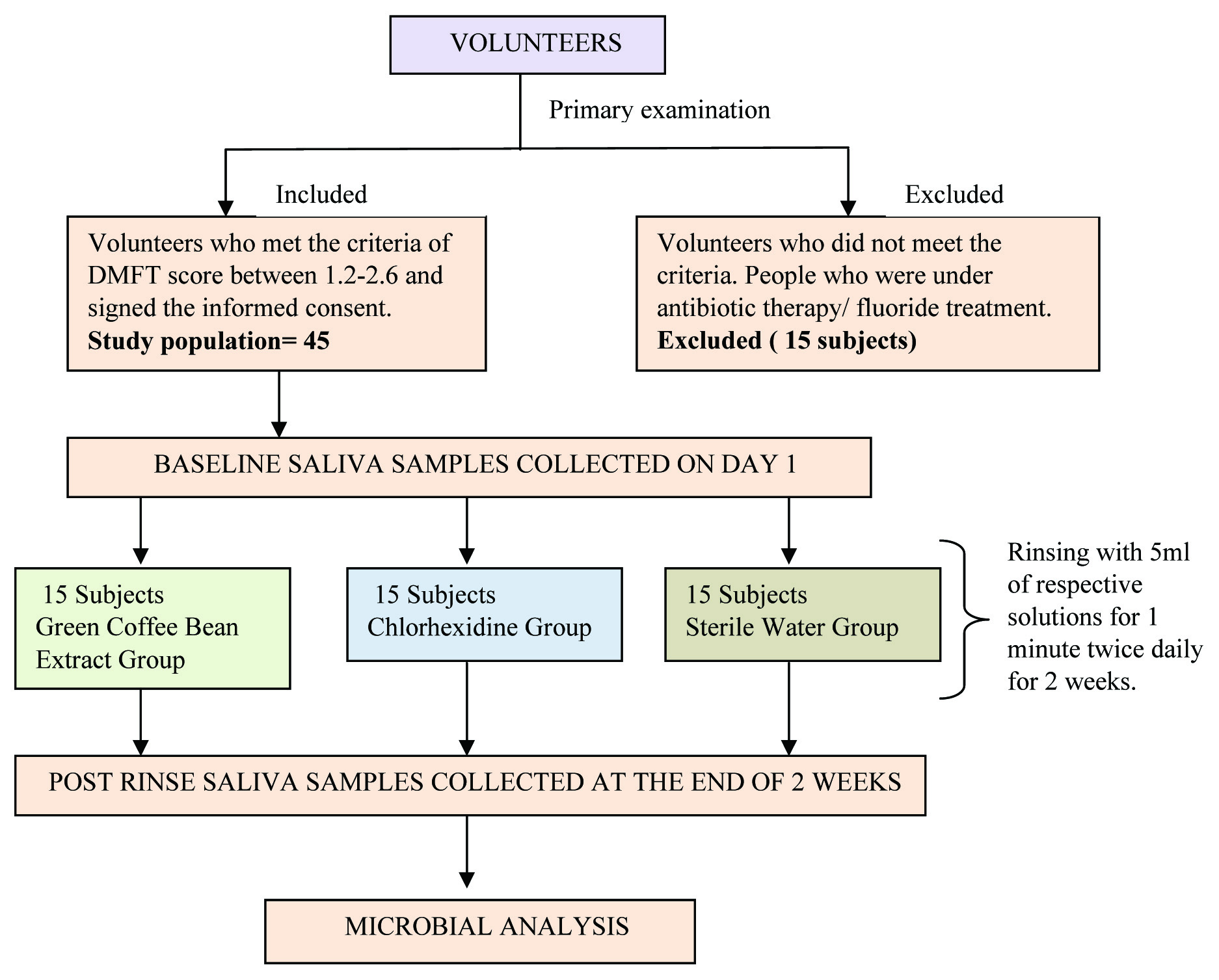
1 ml of baseline salivary sample from each subject was collected on day 1. Saliva was collected in the morning between 7 am and 9.30 am to eliminate any bias in the concentration of saliva due to circadian rhythm. The subjects were informed not to consume anything, except water, two hours prior to the collection of saliva. All subjects were asked to collect saliva in their mouth for one minute and then the subjects were asked to drool their saliva into sterile eppendorf tubes for 1-5 minutes. A 5 ml of the study solutions was dispensed in sterile disposable cups for each group and were given to the subjects as per their respective groups. The subjects were made to rinse their mouth twice daily for one minute for a period of 14 days and were also restrained from using fluoridated toothpaste throughout this trial period. At the end of two weeks, the post rinse saliva samples were collected as described previously. The saliva samples were immediately transferred to a vial containing a transport medium [Table/Fig-1].
Flowchart of methodology.
Selective Agents
The saliva samples were cultured on Mitis Salivarius Agar enriched with bacitracin which is a selective media for Streptococcusmutans. The mitis-salivarius agar was modified by adding 0.2 units/ ml bacitracin and by increasing the sucrose concentration to 20 percent. The selective agents allowed the growth of Streptococcusmutans with maximum inhibition of the balance of the streptococcal flora normally encountered on this medium.
Microbial Evaluation
The samples were transported to the laboratory within 45 minutes after sample collection and the process of microbial analysis was commenced. A 2 fold serial dilution was performed for all the saliva samples using physiological saline, from which a volume of 0.1 ml saliva sample was spread on the mitis salivarius agar plates using spread plate culture technique with a sterile glass spreader. The plates were incubated for 48 hours at 37°C in the incubation chamber (MAC, INDIA) to obtain maximum growth of microbial colonies. On the basis of morphology and size, the counting was performed using a hand held digital colony counter (DBK Coloney Counter, 5003/4, Birla Institute of Technology and Science (BITS) Pilani, Hyderabad) by the same observer under similar conditions and at the same time of the day, in order to avoid any intra observer variability in the results. Counts of Streptococcus mutans were expressed as number of colony forming units/ml.
Statistical Analysis
An intra group comparison of colony count from baseline to 14th day was performed with a paired t-test. One-way variance ANOVA test was used to compare the mean of differential colony counts in the three groups. Post-Hoc test was used to assess the comparative analysis of three mouth rinses. A p-value of < 0.05 was considered statistically significant.
Results
A total of 45 subjects completed the trial. Microbial analysis of saliva samples showed that there was reduction in Streptococcusmutans colony count after rinsing with green coffee bean extract (p≤0.001) and chlorhexidine (p≤0.001) compared to baseline, which was statistically significant. No significant differences were seen in Streptococcus mutans levels among the sterile water group [Table/Fig-2].
Comparison of before rinse and after rinse Streptococcus mutans colony counts within the three groups (Green coffee, Chlorhexidine, Sterile water) using paired t- test.
| Group | Mean | Std. Deviation | Std. rror Mean | t | df | Sig. (2-tailed) |
|---|
| A. Green coffee | Pair 1 | pre-post rinse | 51.53333 | 32.98672 | 8.51713 | 6.051 | 14 | <0.001* |
| B. Chlorhexidine | Pair 1 | pre- post rinse | 55.60000 | 27.56499 | 7.11725 | 7.812 | 14 | <0.001* |
| C. Sterile water | Pair 1 | pre- post rinse | 6.86667 | 16.31768 | 4.21321 | 1.630 | 14 | 0.125 |
Statistically significant.
When pair wise comparison was done among the three groups with Post-Hoc test, no statistical significant difference between green coffee bean extract and CHX (p=1.000) was observed, where as green coffee bean extract and chlorhexidine were found to be more effective when compared to sterile water (p=0.003, p≤ 0.001) which was statistically significant [Table/Fig-3].
Pair wise comparison of three groups (Green coffee, Chlorhexidine, Sterile water) by Post-Hoc test.
| Dependent Variable | (I) Group | (J) Group | Mean Difference (I-J) | Std. Error | p- value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Post rinse | A. Green coffee | Chlorhexidine | 4.26667 | 12.23732 | 1.000 | -26.2491 | 34.7825 |
| Sterile water | -43.26667 | 12.23732 | 0.003* | -73.7825 | -12.7509 |
| B. Chlorhexidine | Green coffee | -4.26667 | 12.23732 | 1.000 | -34.7825 | 26.2491 |
| Sterile water | -47.53333 | 12.23732 | <0.001* | -78.0491 | -17.0175 |
| C. Sterile water | Green coffee | 43.26667 | 12.23732 | 0.003* | 12.7509 | 73.7825 |
| Chlorhexidine | 47.53333 | 12.23732 | <0.001* | 17.0175 | 78.0491 |
The mean difference is significant at the 0.05 level.
[Table/Fig-4] show ANOVA test for comparison of mean differential colony counts at pre rinsing and post rinsing stage between the three groups. There was no significant difference between colony counts of the three groups at pre rinsing stage (p=0.997), however, at post rinsing stage, a statistical significant difference (p≤0.001) between the colony counts of the three groups was observed.
Comparison of mean differential colony counts in the three groups at pre-rinsing and post rinsing stage by ANOVA.
| Source of variation | Sum of squares | Degree of freedom | Mean sum of squares | F-value | p |
|---|
| Pre rinse | Between Groups | 17.200 | 2 | 8.600 | 0.003 | 0.997 |
| Within Groups | 106510.800 | 42 | 2535.971 | | |
| Total | 106528.000 | 44 | | | |
| Post rinse | Between Groups | 20748.133 | 2 | 10374.067 | 9.237 | <0.001* |
| Within Groups | 47171.867 | 42 | 1123.140 | | |
| Total | 67920.000 | 44 | | | |
Statistically significant
Discussion
At present, dental caries is the most frequently occurring multifactorial oral infectious disease. Clarke JK et al., in 1924 first reported the involvement of streptococci in the aetiology of dental caries [8]. Axelsson P and Lindhe J found CHX mouth wash to be very effective in reducing plaque and gingivitis [9]. According to Menendez A, CHX was potent against Streptococcus mutans in dental plaque, hence it was considered as a positive control in the present study to evaluate the effect of green coffee bean extract on salivary Streptococcus mutans count [10]. Sterile water was used as the negative control in the study.
Herbal extracts for tooth cleansing and as an antimicrobial plaque agent have been successfully used in dentistry [11]. Herbal mouth rinses are gaining special attention in the recent times because they are non chemical and non synthetic. Studies on the antimicrobial and anticariogenic properties of coffee species are scarce in literature despite it being the best known and one of the most popular drinks in the world. In the current study, the green coffee bean extract was chosen as it is an herbal product which has shown several health benefits including antibacterial, antifungal, antiviral, antiphlogistic, antioxidant, chemopreventive, and other biological activities [12-17].
Saliva samples were collected in preference to plaque samples as a result of more constant salivary microbial count than plaque, and the possible fluctuation in saliva microbial counts were controlled by sampling saliva at the same hour everyday [18].
The reason for significant reduction in the Streptococcus mutans count in the green coffee group can be attributed to the chlorogenic acid (an active component) and polyphenols, the primary constituents of green coffee bean extract. Chlorogenic acid is structurally composed of, an ester of caffeic acid with the 3-hydroxyl group of a quinic acid. Its level is high in the green coffee as compared to the roasted form of coffee. According to Zhang L et al., the interaction between polyphenols and organic matrices lead to inhibition of the demineralization process [19]. As per the authors, this interaction involves covalent, ionic, hydrogen bonding or hydrophobic processes, which results in alteration of enamel organic matrix. The altered organic matrix is precipitated in the enamel, resulting in reduced mineral ions loss, and as a result, demineralization of enamel is inhibited. Kashket S et al., found that polyphenols inhibit formation of glucosyltransferase by cariogenic bacteria [20]. Antonio AG et al., suggested that Caffeic acid and 5 caffeoylquine, along with polyphenols, show some activity against Streptococcus mutans [21].
In this study, the mean of the chlorhexidine group showed a slightly greater reduction of Streptococcus mutans count in saliva than green coffee mouth rinse. However, this difference was not significant statistically. The green coffee bean extract has some advantages over chlorhexidine as it caused no staining, no altered taste or any allergy reported by the subjects. Moreover, it can be considered as a good preventive home therapy in developing countries as it has added health benefits over the human body [22-25].
Limitation
This study was carried out on a small sample size which could be the limitation of this study and it can be further carried out by more specific microbiological tests and larger sample size to establish the efficacy of green coffee bean extract as a mouth rinse.
Conclusion
Green coffee bean extract shows a statistical significant reduction in Streptococcus mutans count and hence should be considered an alternative mouth rinse due to its herbal and additional health benefits over the human body.
*Statistically significant.
*The mean difference is significant at the 0.05 level.
*Statistically significant