Concomitant Presence of Carcinoma of Breast in a Patient with Early-Onset Cataract: First Case Report of a Potential Association
Shahbaz Habib Faridi1, Kaushal Deep Singh2, Mehershree Lodhi3
1 Assistant Professor, Department of Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India.
2 Senior Resident, Department of Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India.
3 Junior Resident, Department of Microbiology, King George Medical University, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kaushal Deep Singh, Department of Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh-202002, Uttar Pradesh, India.
E-mail: drkdsm@gmail.com
A recent nation-wide population based retrospective cohort study from Taiwan in 2014 suggested a propensity of developing breast cancer in young females with early-onset cataract. We report here a case of a young non-obese female who presented to us with a large lump in the right breast with skin nodules and bilateral painless progressive diminution of vision. Patient was diagnosed to be suffering from locally advanced carcinoma of right breast with axillary metastasis (Stage III B) and bilateral early-onset nuclear cataract. Patient was started on taxane and anthracycline based neoadjuvant chemotherapy and after three cycles of chemotherapy patient showed partial response (≈50% reduction of tumour mass). Patient underwent small incision cataract surgery in left eye after the first cycle of chemotherapy. However, the patient was lost before any operative intervention could be done as she died in a road traffic accident. Possible mechanism of development of breast cancer in patients with early-onset cataract is discussed. This is the first reported case of a patient of early–onset cataract developing breast cancer as well as the first reported case of concomitant presence of early-onset bilateral cataract with breast cancer.
Adjuvant chemoradiation, Anthracycline, Early-onset cataract, Locally advanced carcinoma breast, Modified radical mastectomy
Case Report
A 36-year-old young female came to the out-patient department with complaint of a progressively increasing lump in right breast for 1.5 years. There was also an associated history of a palpable swelling in right axilla; and sudden increase in breast lump with development of redness of overlying skin, multiple skin nodules over the lump and peri-areolar skin denudation for last two months. Patient had painless progressive bilateral (left earlier than right) diminution of vision for last five years with inability to see from both eyes for last five months. Patient also complained of anorexia and weight loss for last two months.
There was no history of bone or joint pain, pain abdomen, jaundice, vomiting, melena, breathlessness, cough, haemoptysis, headache, seizures or any other swelling in the body. There was also no history of trauma to eyes, watering, glares, floaters or redness of eyes. For these complaints patient had consulted local practitioners in nearby town multiple times but due to her poor financial status could not afford the treatment costs associated with surgery. There was no history suggestive of diabetes mellitus, hypertension, tuberculosis or history of any other malignancy in any of the first or second degree relatives of the patient. Patient had neither any addiction to alcohol or tobacco nor history of any drug intake. Patient was P1+0L1 with first and only pregnancy at the age of 28 years. Patient had no menstrual complaints.
On examination, patient had a 10×8 cm diffuse mass with ill-defined margins involving whole of the right breast. The overlying skin had erythema, multiple small skin nodules, peau d’orange appearance and nipple retraction [Table/Fig-1]. The mass was fixed to the skin, breast tissue and chest wall. Multiple anterior and central group (level I) lymph nodes were enlarged in right axilla. The other breast and axilla were clinically disease-free. Patient had bilateral mature nuclear sclerosis type of cataract with only light perception in both eyes [Table/Fig-2]. Other bodily systems were clinically normal. Patient’s Body Mass Index (BMI) was 23.5. Routine laboratory parameters like haemogram, blood sugar, renal functions, liver functions were within normal limits. HbA1c of the patient was 5.3. Mammography revealed thickening of overlying skin with presence of a large dense soft-tissue mass with speculated margins involving right breast with focal areas of pleomorphic microcalcifications.
(a) Right breast mass with overlying skin denudation and peau d’orange at presentation; (b) Same breast mass after three cycles of neoadjuvant chemotherapy showing ≈50% reduction in size, disappearance of skin denudation and right axillary lymph nodes.
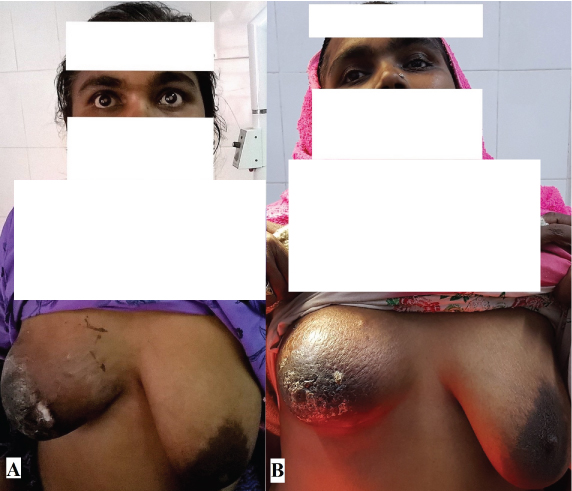
(a) Patient having bilateral early-onset nuclear sclerosis-type mature cataract at presentation; (b) Patient after small-incision cataract surgery in her left eye with good restoration of vision.

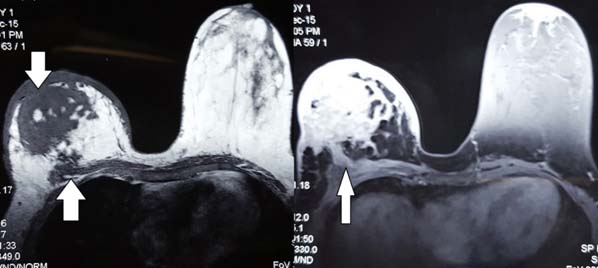
A Contrast-Enhanced Magnetic Resonance Imaging (CE-MRI) with dedicated breast coils of bilateral breast revealed presence of a large ill-defined altered signal intensity infiltrative mass lesion (7.2 × 6.7 × 7.6 cm) involving almost the entire right breast showing heterogeneous enhancement in post-contrast sequences with multiple areas of nodular enhancement with diffuse thickening of the skin with chest wall invasion with few enlarged nodes in right axilla [Table/Fig-3]. Left breast and axilla were essentially normal. A core needle biopsy was done which showed presence of infiltrating ductal carcinoma of breast with triple-negative hormone receptor status. The chest x-ray; skull x-ray; NCCT of head; x-ray of cervical, dorsal, lumbar and sacral spine; x-ray pelvis and long bones; MRI spine screening, ultrasonography of abdomen, contrast enhanced computed tomography of chest and abdomen of the patient were found to be within normal limits.
T1 and T2-weighted images of breast Magnetic Resonance Imaging (MRI) showing a large ill-defined altered signal intensity infiltrative mass lesion involving almost the entire right breast with diffuse thickening of the skin with chest wall invasion.
A bone scan or positron emission tomography of the patient could not be done due to non-availability of same at our center. Genetic testing could not be carried out in the patient due to financial constraints. Patient was diagnosed with locally advanced carcinoma of right breast T4bN2aM0 (stage IIIB) with bilateral early-onset nuclear sclerosis-type mature cataract.
Patient was started on epirubicin, cyclophosphamide and docetaxel neoadjuvant chemotherapy. She developed hyperglycaemia after second cycle of chemotherapy with fasting glucose levels of 135 mg%, postprandial levels of 190 mg% and HbA1C of 6.3 at ninth week. She was started on metformin which controlled hyperglycaemia adequately. She tolerated first three cycles of chemotherapy well with a partial clinical response in the form of ≈50% reduction in tumour size [Table/Fig-1] but complete clinical disappearance of axillary nodes (early-responder). Small-incision cataract surgery was performed in left eye after first cycle of neoadjuvant chemotherapy [Table/Fig-2] and in right eye; it was planned before the fourth cycle of chemotherapy. There was good restoration of vision (6/9) in her right eye when she reported at the time of third cycle of chemotherapy. Patient was planned for a modified radical mastectomy with adjuvant chemoradiation after achieving a complete clinico-radiological response to chemotherapy; however she died in a road traffic accident when she was returning home after the third cycle of chemotherapy.
Discussion
Cataract may be present in patients presenting with carcinoma breast especially in elderly females. This is especially true for elderly post-menopausal females. Age-related cataract usually occur in patients older than 50 years [1], but some patients experience cataracts before this age which is referred to as Early Onset Cataract (EOC). In a nation-wide population based retrospective cohort study by Chiang CC et al., in Taiwan, an increased incidence of breast, liver, and head and neck cancers was observed in patients presenting with EOC [2].
Our patient was a young non-obese female who started developing vision loss at age of around 31 years and by the time she presented to us with right sided breast lump at the age of around 36 years; she had nuclear sclerosis type bilateral mature early onset-cataract with complete loss of vision except light perception. In the absence of any form of trauma and other co-morbidities, our patient can be labelled as to be suffering from EOC. This is the first reported case of concomitant presence of EOC with breast cancer as well as first reported case of a patient of EOC developing breast cancer and may indicate a potential association.
EOC is thought to be due to insufficient anti-oxidative function [1,2]. Carcinogenesis is similarly related to oxidative stress and oxidative damage [3]. The possible mechanisms for this association can be linked to metabolic syndrome [4-6], Reactive Oxygen Species (ROS) [7,8], genetic factors [9,10] and environmental factors [11-13].
Forte et al., found that diabetes and obesity are linked closely and both in turn are associated with an increased incidence of solid tissue cancers [4]. Tan JS et al., reported in their study that metabolic syndrome is associated with all three types of cataracts (nuclear, cortical, and posterior sub-capsular cataracts) [5]. Thus, we saw that metabolic syndrome is a precursor of both cancer as well as cataract. However, our patient was neither obese nor predisposed to any metabolic abnormality so metabolic syndrome was an unlikely cause linking EOC with breast cancer in our case. Hyperglycaemia that developed in our patient after the second cycle of chemotherapy may be attributed to chemotherapy as cyclophosphamide and epirubicin have been implicated as causes of hyperglycaemia and diabetes mellitus [6].
ROS alter gene expression patterns and thus contribute to carcinogenesis through oxidative stress in fibroblasts which then proliferate uncontrollably [3]. ROS lead to lens opacification through oxidative damage to lens proteins [7]. Moreover oxidative damage associated with Ultraviolet (UV) light plays a key role in the development of cataracts [8]. So, if the anti-oxidative function is maleficent at a younger age, EOC may occur because ROS-damaged DNA cannot be repaired, leading to a higher cancer possibility in young adults. This might have been a contributory factor in our patient; however further testing was required to prove any association which was not done in our case.
Saadat I et al., found an increased incidence of cataract in subjects with the null genotype of Glutathione S-Transferase M1 subtype (GSTM1) (odds ratio-1.51; p<0.05) [9]. The polymorphisms of GSTM1, GSTT1, GSTP1 and GSTO2 have been shown to be associated with increased risk of developing breast cancer [10]. Thus, the polymorphism of GST may be a possible link between EOC and carcinogenesis. Genetic factors could have been a potential culprit in our patient in development of EOC and subsequent BC, but we could not investigate for GST polymorphism in our patient.
Wide use of chemicals in our daily lives could also be a potential link relating EOC and cancer. Glyphosate is one such herbicide which is now a major crop management strategy for pre-harvest desiccation of perennial weed control especially with Genetically Modified (GM) crops [11]. Multiple genotoxic and potentially carcinogenic metabolites of fructose are plausibly present in foods derived from glyphosate-resistant crops. These include glyoxylate, glyoxal and methylglyoxal. Methylglyoxal is implicated in cataract development by inducing endoplasmic reticulum stress in human lens epithelial cells, and activating an unfolded protein response leading to overproduction of ROS and altering the cellular redox balance toward lens oxidation [12]. A study on rats conducted by Séralini GE et al., demonstrated that female rats fed with GM maize, treated with glyphosate had very high propensity of developing mammary fibroadenomas and adenocarcinomas [13]. Glyphosate has been in use in India for a long time and our patient was also involved in agricultural activities but there is insufficient evidence which can explain its use as a cause of EOC and/or breast cancer in our patient.
Conclusion
The evidence linking early-onset cataract with cancer is new and needs to be studied in more detail. However, this potential association can improve our understanding of cancer pathogenesis.
[1]. Gupta V, Rajagopala M, Ravishankar B, Etiopathogenesis of cataract: An appraisalInd J Ophthalmol 2014 62(2):103-10. [Google Scholar]
[2]. Chiang CC, Lin CL, Peng CL, Sung FC, Tsai YY, Increased risk of cancer in patients with early-onset cataracts: a nationwide population-based studyCancer Sci 2014 105(4):431-36. [Google Scholar]
[3]. Klaunig JE, Kamendulis LM, Hocevar BA, Oxidative stress and oxidative damage in carcinogenesisToxicol Pathol 2010 38:96-109. [Google Scholar]
[4]. Forte V, Pandey A, Abdelmessih R, Forte G, Whaley-Connell A, Sowers JR, Obesity, diabetes, the cardiorenal syndrome, and risk for cancerCardiorenal Med 2012 2:143-62. [Google Scholar]
[5]. Tan JS, Wang JJ, Mitchell P, Influence of diabetes and cardiovascular disease on the long term incidence of cataract: the Blue Mountains eye studyOphthalmic Epidemiol 2008 15:317-27. [Google Scholar]
[6]. Sharma PK, Misra AK, Singh V, Gupta A, Saroha S, Singh S, Cyclophosphamide and epirubicin-induced diabetes mellitus in breast cancer: A rare occurrenceJ Pharmacol & Pharmacother 2016 7(3):146-48. [Google Scholar]
[7]. Martinez-Outschoorn UE, Balliet RM, Rivadeneira DB, Chiavarina B, Pavlides S, Wang C, Oxidative stress in cancer associated fibroblasts drives tumour-stroma co-evolution: a new paradigm for understanding tumour metabolism, the field effect and genomic instability in cancer cellsCell Cycle 2010 9:3256-76. [Google Scholar]
[8]. Augusteyn RC, Protein modification in cataract: possible oxidative mechanisms. In: Duncan G, edMechanisms of Cataract Formation in the Human Lens 1981 LondonAcademic Press:72-111. [Google Scholar]
[9]. Saadat I, Ahmadi Z, Farvardin-Jahromi M, Saadat M, Association between cataract and genetic polymorphisms of GSTM1, GSTT1, and GSTO2 with respect of work placeMol Vis 2012 18:1996-2000. [Google Scholar]
[10]. Sohail A, Kanwal N, Ali M, Sadia S, Masood AI, Ali F, Effects of glutathione-S-transferase polymorphisms on the risk of breast cancer: a population-based case-control study in PakistanEnviron Toxicol Pharmacol 2013 35:143-53. [Google Scholar]
[11]. Samsel A, Seneff S, Glyphosate, pathways to modern diseases IV: cancer and related pathologiesJ Biol Phys Chem 2015 15(3):121-59. [Google Scholar]
[12]. Palsamy P, Bidasee KR, Ayaki M, Augusteyn RC, Chan JY, Shinohara T, Methylglyoxal induces endoplasmic reticulum stress and DNA demethylation in the Keap1 promoter of human lens epithelial cells and age-related cataractsFree Radical Bio Med 2014 72:134-48. [Google Scholar]
[13]. Séralini G-E, Clair E, Mesnage R, Gress S, Defarge N, Malatesta M, Republished study: long-term toxicity of a Roundup herbicide and a Roundup-tolerant genetically modified maizeEnviron Sci Eur 2014 26(1):14 [Google Scholar]