The most common practical method for assessing GFR is performed with a 24 hour/timed urine collection for creatinine clearance evaluation [4]. The 24 hour urine collection for the estimation of GFR has been shown by studies to be more reliable than serum creatinine-based eGFR formulae in subjects particularly on vegetarian diet, creatine supplementation, amputation of limbs, malnutrition and muscle wasting, because these factors are not specifically taken into account in estimating GFR by creatinine based formulae [5]. But the 24 hour creatinine clearance is inconvenient to the patient and also systematically overestimates the GFR because of tubular secretion of creatinine [6,7]. The estimation of eGFR by creatinine based formulae is known to be rapid and reliable means of approximation of creatinine clearance [8]. There are approximately 40 different equations for calculation of eGFR . The three most commonly used equations to estimate GFR are serum creatinine based Cockcroft-Gault, the MDRD 2006 and CKD-EPI 2009 creatinine equations [9].
The Cockcroft-Gault formula was one of the earliest and most widely used formulas for estimating GFR [10]. This formula takes into account age and weight of the patient and this is not corrected for body surface area. Some studies have suggested that this formulae diverges widely from true measure of GFR in certain clinical situations [10,11]. Since this formulae was derived from a population where only 4% were female and hence an arbitrary correction factor of 0.85 was recommended for females [10].
The original Study Equation, MDRD 1999 included six variables (Age, Sex, Race, Serum Urea nitrogen, Creatinine and Albumin) for estimating GFR [12]. In 2000, the MDRD formulae was simplified to a four variable formulae and in 2006, it was simplified for use with serum creatinine traceable to Isotope Dilution Mass Spectrometry (IDMS) [13,14]. The MDRD 2006 formulae was found to be more accurate when compared with Cockcroft-Gault formulae because of lesser bias and greater precision [10,11]. But the main limitation of MDRD formulae was systematic bias which underestimate GFR at higher levels and imprecision throughout the range.
The CKD-EPI 2009 creatinine formulae was developed to overcome the limitations of 2006 MDRD formulae [15]. The final formulae of CKD-EPI has the same variables as MDRD Formulae but weight, diabetes and organ transplant status were considered for developing the formulae yet this did not enhance the performance [16].
The aim of the study was to compare eGFR using three commonly used Formulae (MDRD 2006, CKD-EPI 2009 and Cockcroft-Gault Formula) with 24 hour creatinine clearance and to identify which amongst the three formulae for eGFR closely correlates with 24 hour creatinine clearance. This study was also done to conclude when and whether the use of creatinine based eGFR calculation method is a safe and accurate alternative to the inconvenient 24 hour creatinine clearance.
Materials and Methods
We retrospectively collected laboratory data requested for 24 hour creatinine clearance in the period from January 2014 to August 2016. All laboratory requests for 24 hour creatinine clearance irrespective of provisional diagnosis were included in the study except for patients less than 14 years of age. Totally 91 laboratory request for 24 hour creatinine clearance data was obtained. Out of 91 patients, 53 were female patients with age range (15-80 years) and 38 were male patients with age range (15-80 years).
Informed consent was obtained from all participants included in the study.
For creatinine clearance estimation; age, sex, height, weight, race, a serum specimen and a 24 hour urine specimen of the patient was collected and then creatinine clearance was estimated by the following formulae.
24 hour creatinine clearance= urine creatinine* Urine volume/serum creatinine *1440.
e-GFR was calculated by MDRD 2006, CKD-EPI (2009) and Cockcroft-Gault formulae.
e-GFR by MDRD 2006 formulae =175 x (SCr)-1.154 x(age)-0.203 x 0.742 (if female) x1.212 (if Black)
e-GFR by CKD-EPI 2009 formulae = 141 x min (SCr/κ, 1)α xmax (SCr/κ, 1)-1.209 x 0.993 Age x 1.018 (if female) x 1.159 (if Black)
{κ = 0.7 (females) or 0.9 (males), α = -0.329 (females) or -0.411 (males), min = indicates the minimum of SCr/κ or 1, max = indicates the maximum of SCr/κ or 1}
e-GFR by Cockcroft-Gault (CG)formulae = {((l 40–age) x weight)/(72xSCr)}x 0.85 (if female)
Creatinine was estimated by enzymatic (creatinine amidohydrolase) method using Dry Slide technology (VITROS 4600). The values assigned to the VITROS Chemistry Products Calibrator for Creatinine are traceable to a Gas Chromatography Isotope Dilution Mass Spectrometry (GC/IDMS) method and National Institute of Standards and Technology (NIST) SRM 914 creatinine standard reference material.
Statistical Analysis
The statistical analysis was performed using SPSS software version 16. The paired-t-test was used since all parameters used in the study were numerical, all patients came from same population and all had paired results.
Results
[Table/Fig-1] shows the comparison of all patients included in the study by paired-t-test, between the three eGFR methods with 24 hour creatinine clearance. A statistically significant difference (p<0.05) was observed between all eGFR methods with 24 hour creatinine clearance when all patients included in the study independent of age, sex and race were compared.
Comparison of all patients included in the study by paired-t-test, between MDRD (2006), CKD-EPI (2009), Cockcroft-Gault (C-G) with 24 hr creatinine clearance.
| Methods | Total Noparticipants | Mean | SD | SEM | p |
|---|
| Creatinine clearance 24 hour urine collection | 91 | 59.53 | 30.42 | 3.18 | - |
| MDRD (2006) | 91 | 62.93 | 35.35 | 3.70 | <0.05 |
| CKD-EPI (2009) | 91 | 64.62 | 32.85 | 3.44 | <0.05 |
| COCKCROFT-GAULT (C-G) | 91 | 64.26 | 31.32 | 3.28 | <0.05 |
[Table/Fig-2,3] shows the sex wise comparison of all patients included in the study independent of age. This showed statistically significant difference (p< 0.05) between all the eGFR methods with 24 hour creatinine clearance in both sexes. Hence no conclusion could be derived from this analysis as to which eGFR method is advantageous over the other.
Comparison of eGFR in male participants between MDRD (2006), CKD-EPI (2009), Cockcroft-Gault WITH 24 hour creatinine clearance.
| Methods | No of maleparticipants | Mean | SD | SEM | p |
|---|
| Creatinine clearance 24 hr urine collection | 38 | 53.34 | 27.89 | 5.27 | - |
| MDRD (2006) | 38 | 56.0 | 30.8 | 5.82 | <0.05 |
| CKD-EPI (2009) | 38 | 57.21 | 28.74 | 5.43 | <0.05 |
| COCKCROFT-GAULT | 38 | 53.75 | 25.56 | 4.83 | <0.05 |
Comparison of eGFR in female participants between MDRD (2006), I CKD-EPI (2009), Cockcroft-Gault with 24 hour creatinine clearance.
| Methods | No of femaleparticipants | Mean | SD | SEM | p |
|---|
| Creatinine clearance 24 hr urine collection | 53 | 62.27 | 31.29 | 3.94 | - |
| MDRD (2006) | 53 | 66.01 | 37 | 4.66 | <0.05 |
| CKD-EPI (2009) | 53 | 67.92 | 34.23 | 4.31 | <0.05 |
| COCKCROFT- GAULT | 53 | 68.93 | 32.67 | 4.11 | <0.05 |
[Table/Fig-4] shows the comparison of eGFR in five stages of CKD (Stage I >90 ml/min, Stage II 60-89 ml/min, Stage III 30-59 ml/min, Stage IV 15-29 ml/min and Stage V <15 ml/min) between MDRD (2006), CKD-EPI (2009) and Cockcroft-Gault Formula with 24 hour creatinine clearance. The eGFR by MDRD formulae had a statistically insignificant p-value (p > 0.05) i.e., good approximation in the IInd, IIIrd, IVth and Vth stages of CKD on comparison with 24 hour creatinine clearance. The eGFR by CKD-EPI formulae had a statistically insignificant p-value (p > 0.05) in the IInd, IVth and Vth stages of CKD. The eGFR by Cockcroft-Gault Formulae had a statistically insignificant p-value (p > 0.05) in the Ist, IInd and Vth stages of CKD. This showed that MDRD formulae had good approximation of 24 creatinine clearance in four stages of CKD.
Comparison of eGFR in different stages of CKD between MDRD (2006), CKD-EPI (2009), Cockcroft-Gault with 24 hour creatinine clearance.
| CKD stages | No. Of partici- pants | Crea- tinine clearance 24 hour urine collection | MDRD (2006) | p-value | CKD- EPI (2009) | p-value | COCK- CROFT- GAULT | p - value |
|---|
| I | 21 | 103.58 | 116.33 | <0.05 | 111.14 | <0.05 | 111.3 | <0.05 |
| II | 16 | 75.96 | 74.56 | 0.5 | 81.56 | 0.09 | 75.13 | 0.7 |
| III | 38 | 43.80 | 45.21 | 0.2 | 48.68 | <0.05 | 49.01 | <0.05 |
| IV | 13 | 25.39 | 26.30 | 0.4 | 27.76 | 0.1 | 31.25 | <0.05 |
| V | 3 | 10.66 | 10.33 | 0.8 | 10.33 | 0.8 | 13.26 | 0.3 |
| ALL | 91 | 59.53 | 62.93 | <0.05 | 64.62 | <0.05 | 64.26 | <0.05 |
[Table/Fig-5] shows the comparison of 24 hour creatinine clearance in four subgroups <90, <60, <30 and <15 with eGFR by MDRD (2006), CKD-EPI (2009), Cockcroft-Gault (C-G) formulae independent of age and sex. The eGFR by MDRD showed good approximation of creatinine clearance in all sub-groups. The eGFR by CKD-EPI showed good approximation of creatinine clearance in two sub groups (<30 and <15). But Cockcroft-Gault Formulae gave disappointing results in all sub-groups except in sub-group of creatinine clearance <15.
Comparison of 24 hour creatinine clearance in four subgroups <90, <60, <30 and <15 with eGFR by MDRD (2006), CKD-EPI (2009), Cockcroft-Gault formulae independent of age and sex
| 24 hour creatinine clearance | No. Of participants | Creatinine clearance 24 hour urine collection | MDRD (2006) | p-value | CKD-EPI (2009) | p-value | Cockcroft-Gault | p-value |
|---|
| <90 | 70 | 46.31 | 46.91 | 0.4 | 50.67 | <0.05 | 50.15 | <0.05 |
| <60 | 53 | 37.09 | 38.39 | 0.1 | 41.15 | <0.05 | 42.37 | <0.05 |
| <30 | 16 | 22.63 | 23.31 | 0.5 | 24.5 | 0.1 | 27.88 | <0.05 |
| <15 | 3 | 10.66 | 10.66 | 0.8 | 10.33 | 0.8 | 13.26 | 0.3 |
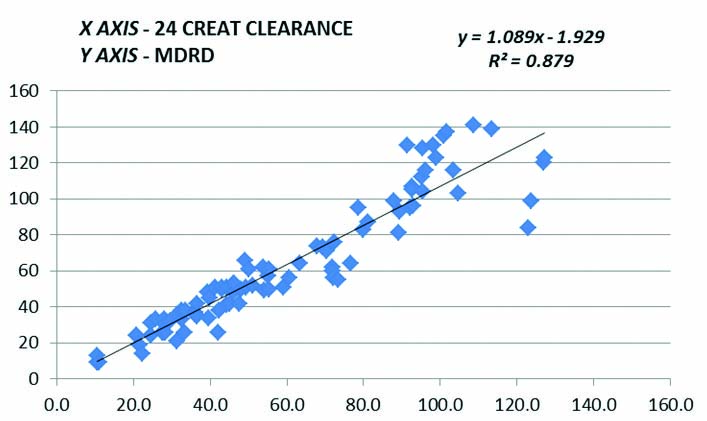
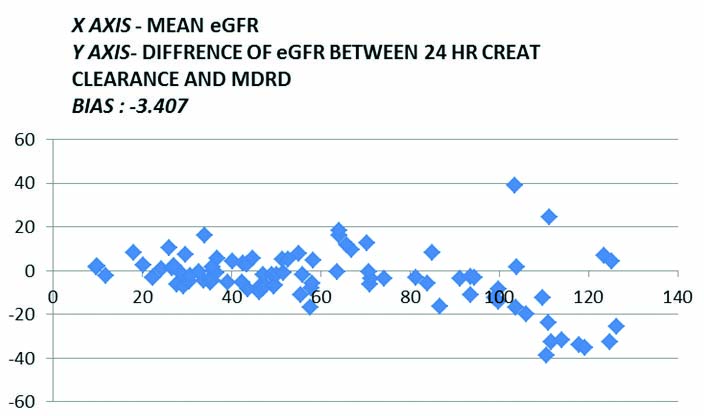
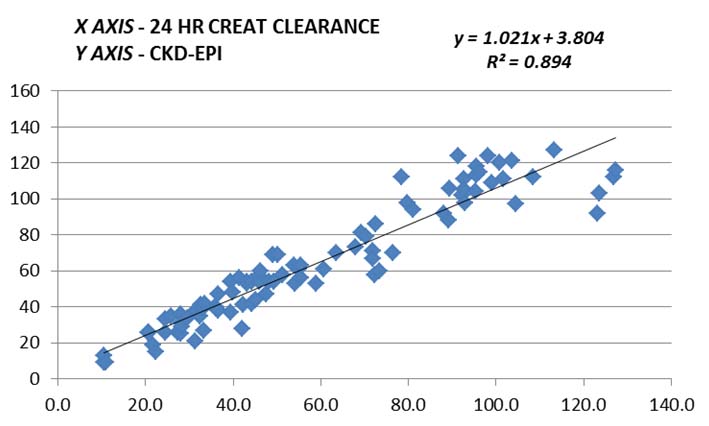
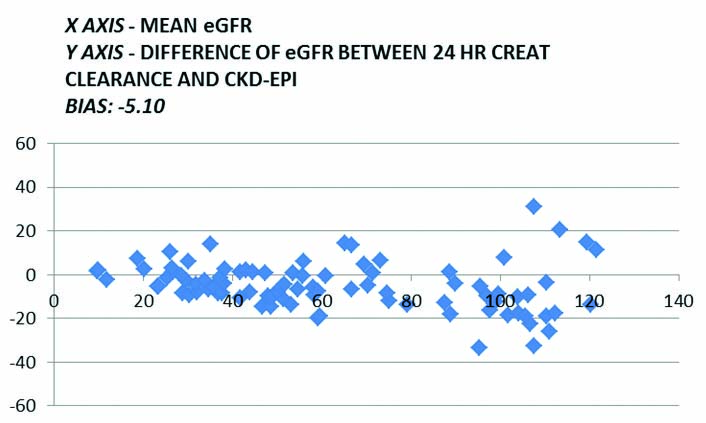
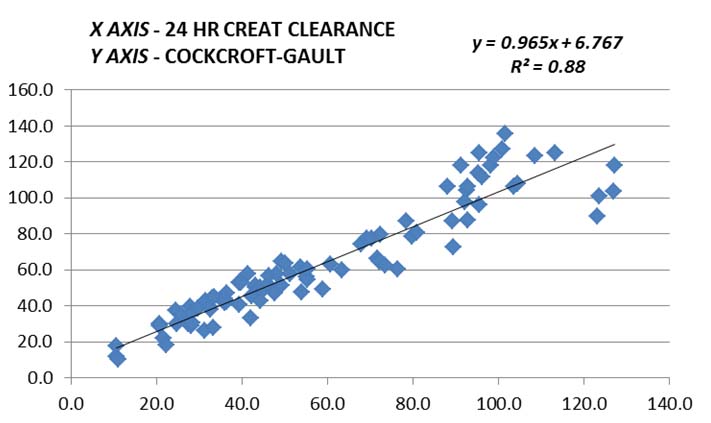
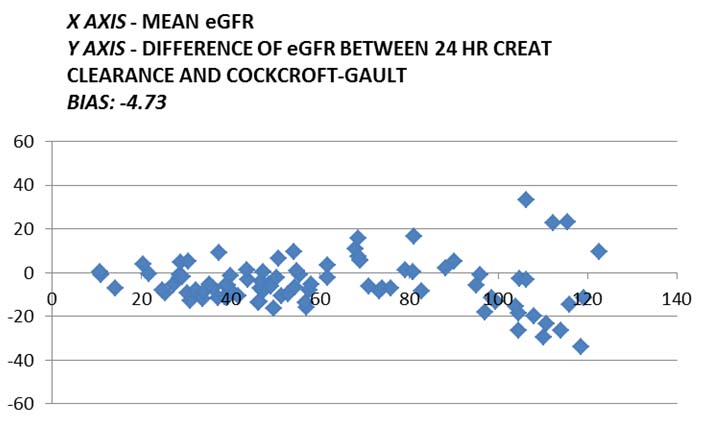
[Table/Fig-6,7,8,9,10 and 11] show the graphical comparison by Linear regression and Bland-altman plot between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by MDRD, CKD-EPI and Cockcroft Gault formulae.
Graphical comparison by linear regression between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by MDRD formulae.
Graphical comparison by bland-altman plot between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by MDRD formulae.
Graphical comparison by linear regression between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by CKD-EPI formulae.
Graphical comparison by bland-altman plot between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by CKD-EPI formulae.
Graphical comparison by linear regression between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by Cockcroft-Gault formulae.
Graphical comparison by b) Bland-Altman plot between clearance in ml/min calculated from 24 hour creatinine clearance and eGFR as calculated by Cockcroft-Gault formulae.
Discussion
The ideal marker for estimation of GFR is Inulin or 125I-iothalamate clearance methods. Since these methods are expensive, time consuming and technically complicated, either 24 hour creatinine clearance or creatinine based formulae is used for estimating GFR. Although, some studies have found that Cystatin C to be more accurate marker of GFR, other studies have suggested that it does not outmatch creatinine based formulae [17,18]. One study suggested that GFR estimation for drug dosage adjustment was unsatisfactory from creatinine based formulae while other study suggested that creatinine measurement itself might be biased due to laboratory variability [19]. Hence, physicians around the world have adjusted the eGFR equations to their population.
The importance of GFR measurement is to make a decision whether or when the patient must begin dialysis. In cases other than factors indicating immediate initiation of dialysis (i.e., uremic symtoms, pericarditis etc.,) the time to initiate chronic dialysis is when GFR drops below 15 ml/min. Since no single formulae for estimating GFR is optimal for all population, we undertook a study to compare estimated GFR using three commonly used Formulae (MDRD 2006, CKD-EPI 2009 and Cockcroft-Gault Formula) with 24 hour creatinine clearance. The objective was to identify which among the three formulae for eGFR closely correlates with 24 hour creatinine clearance.
Sex wise comparison of all patients included in our study independent of age showed statistically significant difference (p<0.05) between all eGFR methods with 24 hour creatinine clearance. It would be easy to suggest that we could use different formulae for men and women, different levels of plasma creatinine and/or different age groups but such an assumption would make the eGFR approach more complicated.
The ideal method of eGFR has to fulfil certain requirements. First of all it has to be accurate enough to place the patient in its correct CKD stage, second, it has to be easy to calculate and, third, it has to demand as little data as possible. All the three formulae used in our study to estimate GFR fulfilled second and third criteria but MDRD 2006 formulae showed good approximation (p >0.05) of creatinine clearance in the IInd, IIIrd, IVth and Vth stages of CKD. The CKD-EPI 2009 formulae showed good approximation (p >0.05) of creatinine clearance in the IInd, IVth and Vth stages of CKD but the Cockcroft-Gault formulae showed good approximation (p >0.05) of creatinine clearance only in the IInd and Vth stages of CKD.
The evaluation of GFR in the validation population showed lesser bias for the CKD-EPI 2009 than MDRD 2006 formulae, but there was only moderate improvement in overall accuracy and in drug dosage adjustment [20]. Another study also showed that CKD-EPI 2009 equation to have a lower bias, especially at estimated GFR greater than 60 ml/min/1.73 m and hence they recommend CKD-EPI 2009 equation for reporting eGFR replacing MDRD 2006 Study equation. But to contrary, in our study MDRD 2006 formulae showed a good approximation of 24 hour creatinine clearance at values greater than 60 ml/min/1.73 m in comparison with CKD-EPI 2009 equation.
Limitation
This study has certain limitations. Ideally, we would have measured the plasma creatinine on the same day the GFR measurement was performed in all patients. A plasma creatinine measurement on the same day as the GFR measurement was available for 72 (79.12%) patients. Another limitation of this study is the relatively limited numbers of patients in the subgroups to make a valid comparison. However, we were able to include a relevant number of patients, sufficient to allow stratification.
Conclusion
The creatinine based GFR estimation provides a more accurate assessment of 24 hour creatinine clearance and kidney function than measuring serum creatinine alone but have certain limitations in few clinical circumstances. No single equation will be optimal for all populations. The result of our study showed MDRD 2006 formulae to be more accurate than CKD-EPI 2009 and Cockcroft-Gault formulae in estimating GFR, drug dosing, detection of CKD, and estimating prognosis.