Along with function, aesthetics plays an important role in treating partially or completely edentulous patients. Ageing, trauma, tooth loss and neuromuscular disorders have a high impact on tonicity of facial musculature, elasticity of skin as well as function of muscles. Patients affected with Bell’s palsy face functional, aesthetic as well as psychological impairment. Common problems are the partial closure of upper eyelid, sagging of lower eyelid and drooping of angle of mouth leading to facial asymmetry, along with difficulty in eating, drinking and speaking. The key to aesthetic restoration is to support and harmonize the collapsed facial musculature with the help of various prosthodontic treatment approaches. This case report attempts to focus on treating completely edentulous patient affected with Bell’s palsy with special prosthesis supporting angle of mouth and lower eyelid using novel technique.
Bell’s Palsy, Ectropion, J-Loop, Neutral Zone
Case Report
A 62-year-old male patient reported to the Department of Prosthodontics, Sudha Rustagi College of Dental Sciences and Research, Faridabad, Haryana, India with the chief complaint of difficulty in mastication from past two years. Patient also complained of inability to close his right eye along with constant irritation, redness and tears drooling down from the same side since then [Table/Fig-1].

Medical history revealed that patient was diagnosed with Bell’s palsy but did not seek any medical consultation or treatment for the condition due to financial constraints. Dental history revealed that the patient lost his teeth one year back due to periodontal problems and did not sought any treatment for the same.
Intraoral examination showed well formed edentulous maxillary and resorbed mandibular ridge with healthy oral mucosa [Table/Fig-2]. On extraoral examination, it was evident that patient had classic features of Bell’s palsy. Patient had asymmetrical face with loss of muscle bulk (droop) on the paralyzed side. He had jerky movements of the lower jaw at closure and also while speaking. Patient was unable to furrow, puff his cheeks or whistle and there was loss of nasolabial fold. Patient also presented with partial closure of upper eyelid (lagopthalmos) and sagging of lower eyelid (ectropion). Patient was graded as Grade IV i.e., moderately severe dysfunction according to House-Brackmann [1] facial nerve grading system which is used to assess the severity and recovery from facial paralysis. Informed consent was taken from the patient.
Maxillary and mandibular edentulous ridge.

Treatment Procedure
Complete denture with J-loop extension for restoring facial disfigurement: Maxillary and mandibular preliminary impressions were made using impression compound (Pinnacle, DPI, India) followed by secondary impression using zinc oxide eugenol impression paste (DPI, India). After final impressions were made, permanent heat cure maxillary and mandibular record bases were fabricated for increased stability. Maxillary and mandibular wax occlusal rims were fabricated using modelling wax (DPI, India). Maxillary occlusal rim was inserted in patient’s mouth and extra wax was added to increase buccal fullness on the affected side thereby, supporting the affected facial muscles and enhancing facial symmetry. The orientation jaw relation was done using face-bow and maxillary cast was mounted on the semi-adjustable articulator (Hanau wide-vue). The vertical jaw relation was taken and the mandibular cast was mounted in centric relation at an established vertical dimension of occlusion.
The wax occlusal rim was then removed from the mandibular record base and four occlusal stops, two anterior and two posterior were made with cold cure acrylic resin (DPI, India) to maintain the vertical dimension. For recording neutral zone, impression compound (Pinnacle, DPI India) and green stick impression compound (DPI, India) were mixed in a ratio of 3:7 [2]. The manipulated material was placed on the lower denture base into the patient’s mouth. The patient was guided to swallow, pucker, smile, grin, lick and purse his lips [Table/Fig-3]. He was also asked to talk aloud and count from 60-70. These movements were repeated to mold the impression compound in the area of neutral zone, until proper neutral zone record was made at an already established vertical dimension. The neutral zone record was placed more buccally on the affected side due to decreased activity of buccal musculature.
Neutral zone recording movements.

The neutral zone record was then placed on the mandibular cast and V-shaped notches were made on the land area of mandibular cast. Putty index was made with elastomeric impression material, contoured around the facial and lingual neutral zone space. The neutral zone record material was thus removed and replaced with modeling wax (DPI, India) to get the exact replica of neutral zone. Teeth arrangement was done using putty index as a guide and denture was processed in the conventional manner.
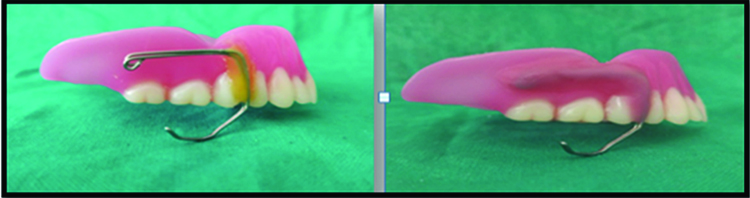
At the insertion appointment, J-loop was fabricated with 21 guaze stainless steel wire adapted on the right buccal flange of denture and secured with the help of sticky wax. The loop length was adjusted until it extended slightly outside the lip at the commissure to support the paralysed side. Adjustment was made to ensure that placement of J-loop restored the facial symmetry and aesthetics without compromising comfort and function. Once the trial of the prosthesis was done, self-cure acrylic resin (DPI, India) was used to permanently stabilize the J-loop extension [Table/Fig-4,5]. Patient’s moustache allowed camouflaging the extraoral extension of the J-loop.
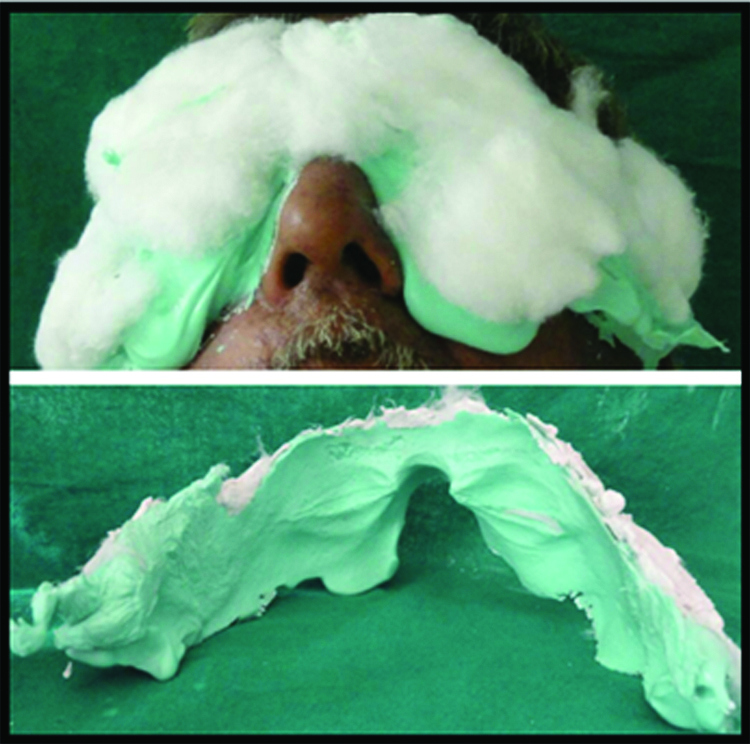
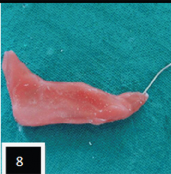
Lower eyelid support prosthesis with spectacle / Prosthodontic management of ectropion: Alginate (Neocolloid, Zhermack) was mixed following manufacturer’s instructions and was impressed upon face covering both eyes, upper part of nose and forehead [Table/Fig-6]. Impression was poured using dental stone (Kalrock, Kalabhai, India) to obtain facial moulage [Table/Fig-7]. A 21 guage stainless steel wire was adapted below the right lower eyelid extending till outer canthus of eye and wax pattern was contoured over it to support the stainless steel wire [Table/Fig-8] on lower eyelid. The other end of wire was inserted in the hole made in the right nose pad of spectacle.
Complete denture with J-Loop prosthesis.

Extraoral impression of face.

Prosthesis trial was done and care was taken while complete seating of spectacle, it supported the lower eyelid [Table/Fig-9]. Prosthesis was removed from the spectacle, flasked, dewaxed and processed using heat cure acrylic resin (DPI, India) by conventional technique [Table/Fig-10,11 and 12]. After deflasking, acrylic prosthesis was finished and polished. The final prosthesis trial was done to determine the correct position of wire attachment on to the nose pad of spectacle. The wire extending onto the nose pad was secured at the determined position using cold cure acrylic resin (DPI, India) [Table/Fig-13]. The fit of the lower lid prosthesis along with spectacle was evaluated on the patient [Table/Fig-14]. Care was taken that it supported lower eyelid without any extra pressure on lower eyelid [Table/Fig-15,16].




Lower lid prosthesis with spectacle.

Lower lid prosthesis in place.

Postoperative view with restored facial symmetry;

Postoperative view with lower lid supporting prosthesis.

Routine follow up appointments were carried out at one, three and six months to ensure patient’s comfort and satisfaction. The patient reported with decreased frequency of irritable eye and tears drooling down of the eye. The patient was also satisfied with the aesthetic enhancement done using J-loop prosthesis. No discomfort or difficulty in mouth opening and mastication were reported as a result of J-loop extension. Patient was quite happy and satisfied with the prosthesis.
Discussion
The primary concern while treating Bell’s palsy patient is to figure out the explicit problems related to the disorder which may lead to legitimate treatment plan. Drooping of angle of mouth, loss of naso-labial fold, flaccid facial musculature on affected side leading to profuse facial asymmetry have been successfully managed in past using denture modifications to provide cheek support. Fickling B and Lazzari JB fabricated spring loaded acrylic dentures and intra oral splint respectively to support the lip and cheek [3,4]. Emory L suggested increased horizontal overlap of the posterior teeth or an over-contouring of the denture base material on the affected side [5]. Larsen SJ et al., suggested and compared palliative treatment using intraoral extraoral approach, intra oral approach with no vestibular tension, intraoral approach with disto-superior tension, intraoral approach with medio-superior tension. J-loop extension is the modification of intraoral-extraoral technique as suggested by Larsen SJ et al., [6]. The prosthesis not only improved the circumoral symmetry but also enhanced facial aesthetics. No dislodging forces were exerted on the maxillary denture base as the tissues were flaccid on the paralysed side.
A successful and stable denture relies on the function and co-ordination of neuromuscular system. The debilitating features of Bell’s palsy may interfere with steps of impression making, jaw relation record, denture retention and stability. To improve the denture stability in such cases, flange contour and teeth position is of utmost importance. The basis of neutral zone helps to recognise and utilize the functional forces generated through muscular contraction to have positive influence on the stability of denture [7,8]. Therefore, in order to maintain harmony of neuromuscular system with muscle function, it is essential to record neutral zone in Bell’s palsy patients [9].
The palliative treatment options for partial closure of upper eyelid (lagopthalmos) have been documented as ophthalmic solutions that serve as lubricants, protective eye glasses help to decrease tear evaporation and exposure keratitis. Contact lenses and scleral shells provides bandage-type corneal protection. Lid loading technique using silicone bands, palpebral springs, platinum cobalt magnets, gold weight, lateral tarsorraphy and canthoplasty are surgical procedures employed in the past [10-12]. Also, several surgical techniques are available for correction of lower eyelid ectropion [13]. But conservative treatment approach to treat ectropion has never been reported. Hence, in this case report correction of paralytic ectropion has been made using lower lid supporting appliance, which is simplified and non-invasive treatment approach to help patient evade the repercussions of eye involvement in Bell’s palsy.
Conclusion
The technique described offers a simple, expedient and non-invasive approach in managing some of the sequelae related to Bell’s palsy. The neutral zone record permitted excellent stability of the dentures and J-loop extension allowed for facial re-animation by correcting facial asymmetry. Lower lid supporting appliance along with spectacle helped patient to overcome various consequences of ectropion. Therefore, the ability of dentist to understand and recognize the problems of patients and to select the proper course of treatment required and reassure them is of great clinical importance.
[1]. House JW, Brackmann DE, Facial nerve grading systemOtolaryngol Head Neck Surg 1985 93(2):146-47. [Google Scholar]
[2]. McCord JF, Tyson KW, A conservative prosthodontic option for the treatment of edentulous patients with atrophic (flat) mandibular ridgesBr Dent J 1997 182:469-72. [Google Scholar]
[3]. Fickling B, Buccal sulcus supports for facial paralysisBr Dent J 1951 90(5):115-17. [Google Scholar]
[4]. Lazzari JB, Intra oral splint for support of the lip in Bell’s PalsyJ Prosthet Dent 1955 5:579-81. [Google Scholar]
[5]. Emory L, The face in patient evaluation and diagnosisJ Prosthet Dent 1976 35(3):247-53. [Google Scholar]
[6]. Larsen SJ, Carter JF, Abrahamian HA, Prosthetic support for unilateral facial paralysisJ Prosthet Dent 1976 :192-201. [Google Scholar]
[7]. Beresin VE, Schiesser FJ, The neutral zone in complete denturesJ Prosthet Dent 1976 36(4):356-67. [Google Scholar]
[8]. Alfano SG, Leupold RJ, Using the neutral zone to obtain maxillomandibular relationship records for complete denture patientsJ Prosthet Dent 2001 85(6):621-23. [Google Scholar]
[9]. Fahmy FM, Kharat DU, A study of the importance of the neutral zone in complete denturesJ Prosthet Dent 1990 64(4):459-62. [Google Scholar]
[10]. Grisius M, Hof RL, Treatment of lagophthalmos of the eye with a custom prosthesisJ Prosthet Dent 1993 70:333-35. [Google Scholar]
[11]. Sela M, Taicher S, Restoration of movement to the upper eyelid in facial palsy by individual gold implant prosthesisJ Prosthet Dent 1984 52:88-90. [Google Scholar]
[12]. Somani P, Nayak AK, Restoration of blinking reflex and facial symmetry in a Bell’s palsy patientIndian J Dent Res 2011 22:857-59. [Google Scholar]
[13]. Miletic D, Elabjer BK, Bosnar D, Busic M, Our approach to operative treatment of lower lid ectropionActa Clin Croat 2010 49(3):283-87. [Google Scholar]