How Non Consumers Differ from Consumers: A Qualitative Approach to Synthesize the Attributes of Iron Folic Acid End Users
Surya Bali1, Ankur Joshi2, Sharad Tiwari3, Daneshwar Singh4, Viswanath Arutagi5, Saket Kale6, DInesh Kumar Pal7
1 Associate Professor, Department of Community and Family Medicine, All India Institute of Medical Science, Bhopal, Madhya Pradesh, India.
2 Assistant Professor, Department of Community and Family Medicine, All India Institute of Medical Science, Rishikesh, Uttrakhand, India.
3 Resident, Department of Community Medicine, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
4 Resident, Department of Community Medicine, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
5 Resident, Department of Community Medicine, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
6 Assistant Professor, Department of Community Medicine, R D Gardi Medical College, Ujjain, Madhya Pradesh, India.
7 Professor and Head, Department of Community Medicine, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ankur Joshi, Assistant Professor, Department of Community and Family Medicine, All India Institute of Medical Science, Rishikesh-249201, Uttrakhand, India.
E-mail: drankurjoshi7@gmail.com
Introduction
Anaemia continues to be a major hurdle to achieve optimum health in Indian population context. Although government continues to promote Iron Folic Acid (IFA) supplementation as one of the key strategies to combat with burden of anaemia, the expected level of IFA consumption and subsequent anaemia reduction could not be achieved. This study tries to investigate those influences, concerns, experiences and behaviour from an end user perspective through a qualitative methodology which may affect the IFA consumption ambi-directionally.
Aim
To explore and understand the several aspects related with anaemia and IFA supplementation with special emphasis to reveal the contributory factors behind low level of IFA consumption at consumer end.
Materials and Methods
A community based qualitative study was conducted in clusters identified through multileveled stratification from a state of central India. A conceptual construct was made in priory for this study. As the research question was related with policy, this study adapted a framework technique for making interview topic guides. Two consumers and two non consumers from each identified cluster were interviewed in depth. The data obtained through 160 in depth interviews (from 80 consumers and 80 non consumers) was utilized for thematic framework, linkage association and to typify the phenomenon.
Results
Ignorance, difficult intake, meaninglessness, misconceptions and discontentment with the system were the major dimensions (sub themes) associated with discontinuation. All these sub themes were further converged into major theme of informational discontinuity. Investigators further typified the users/non users into persistent user, potential defaulters, impending defaulters and absolute non users.
Conclusion
Informational gap seems to be the fundamental factor behind sub optimum IFA consumption. On a policy perspective, all the attempts should be done to instigate arise felt need’ among target groups for IFA consumption.
Anaemia, Defaulters, Non-adherence, Perspective
Introduction
Nutritional anaemia due to IFA deficiency is not a binary phenomenon. It can be visualized as ‘continuum of deficiency’ from depletion of the iron storage in the body leading to latent iron deficiency to overt manifestation of anaemia [1]. Hence overt Iron Deficiency Anaemia (IDA) only represents the farthest inferior end of the prevalent iron deficiency in the community. This resultant spectral deficiency may be further assumed as the complex interplay of biomedical requirement of iron of an individual with social dynamics, cultural beliefs, gender equations, economic issues, awareness and penetration of health/ allied services [2]. These wide ranging manifestations are evident in all ages groups as iron is the major contributory micronutrient in various molecular structures and metabolic systems [3]. Because of this reason IFA supplementation (one of the key strategy to fight with nutritional anaemia) is now emphasising the universal coverage [4].
Intensive efforts on policy and implementation level are made by government in the past for anaemia reduction [5,6]. But the prevalence trend of nutrition anaemia among the various age groups is continuing to remain static or having a slow decline [5,6]. Viewing this issue from system’s perspective, this phenomenon may be considered as classical example of complex adaptive system where assurance of inputs (IFA supplementation) may not be essentially converted into desired output (anaemia reduction) but the outcome may depend on non linear interactions of other existing/emerging factors [7].
Hence from the policy perspective it is imperative to understand those ‘forces’ which may affect the consumption of IFA in both positive and negative direction [8]. Exploration of this phenomenon through qualitative enquiry provides an opportunity to scrutinise the issue from the perspective of one who is taking IFA supplementation (consumers) and the one who has either quitted to take IFA (defaulters) or who have not taken the IFA in spite of compelling indications (non consumers). This inquiry explores the possible answer of a vital question: what are the convergent and divergent points in behavioural traits, treatment experiences, expectations, system concerns and perceptions of a consumer and defaulter/non consumer and whether these dissimilarities can project/predict the trajectory of a beneficiary?
Materials and Methods
The question is one of the specific objective of the larger study which includes a mix of qualitative in depth inquiry with quantitative supplementation. This community based study was conducted in 10 districts of Madhya Pradesh for a period of one year (July 2014 to July 2015). In order to ensure an equal geographical representation, the state was divided into five zones-East, West, North, South and Central. Each district from corresponding zone was assigned a numerical number. Two districts from each zone were selected using RANDBETWEEN function in Microsoft Excel. A conceptual construct on IFA consumptions was in priory designed in collaboration with state program managers involved in the IFA supply chain management. This construction provided us the foundation upon which the topic guide was prepared. As the issue under investigation was nearer to applied policy research, we adapted the framework technique [9,10]. Thus, the topic guide included the both ‘priori’ issues (assumptions) with probes and a scope for addition of ‘emerging concepts’ during in-depth interview.
A ‘consumer’ for this study was defined as the female in the age group of 10-45 years who is offered IFA either for prophylactic/ preventive purposes as per programmatic requirement or for the curative purposes by any of the five persons namely physician, Auxiliary Nurse Midwife (ANM), Anganwadi Worker (AWW), Accredited Social Health Activist (ASHA) or School teacher. A ‘non consumer’ was operationally defined as the previous consumer who because of any reason has discontinued the IFA for at least 15 days before the date of interview. IFA supplementation for this study was defined as offering of IFA tablets as per programmatic guidelines to users by either physician or frontline workers (mentioned above). The quantitative arm of this study (not a part of this manuscript) adapted a stratified multistage cluster sampling for identification of 40 clusters in the quantitative arm, the investigators took this opportunity to select consumers and non consumers (for qualitative in depth interviews) from these clusters in order to capture the maximal geographical variation. Eighty consumers and 80 non consumers (two pair from each cluster) purposely selected with the aid from frontline workers for in depth were interviewed in two phases. As defined all these participants were prescribed IFA tablets for either preventive (prophylactic) or curative reasons as per programmatic guidelines.
At initial phase, 16 consumers and 16 non consumers were interviewed (from eight clusters in two districts) by using the topic guide. Theoretical memos and field observations were also made by investigators during the interview. The responses of the participants were audio recorded and were transcribed thereafter. All personal identifying information was removed during transcription process. The transcribed interviews were read several times by three investigators in parallel for identification of emerging ‘codes’ not included into topic guide. All those codes which were endorsed by at least two out of three investigators were included in the topic guides. All the investigators had a previous experience in qualitative research methodology. An extensive collaborative brain storming session was also coordinated by principle investigator before commencing this study. Validity was ensured by the research design itself (exploratory and capturing complexity) at initial phase, approach to analysis (thematic and framework analysis), inclusion of a team of researchers rather than single researchers, inclusion of ‘negative’ or deviant cases and adequate and systematic use of the original data (using quotations and not all from the same person) in the presentation of analysis.
In the next phase these improved topic guides were used in the rest of the eight districts. Each interview was assigned an alphanumerical number. Interviewees were given pseudonyms. A secure file was created that links pseudonyms and alphanumerical numbers to the original informants.
All the tape recorded interviews were transcribed with inclusion if non verbal cues (like silence or simply a pause for thought)/field observations/memos. Names and other identifiable material were removed from the transcripts. The lines/paragraph of transcripted data was numbered. The coding was done manually by using the cutting and pasting technique for a subset of the transcripts. Different colours were used to show the similarity/dissimilarity between codes. A cross referencing system (which could lead to original text from where cutting and pasting was done) was also developed by using alphanumerical codes. The researchers then started to combine the codes (conveying the similar or complimentary meaning and arguments) into several categories. The nomenclature of categories were done as per either ’priori’ conceptual framework or emergence from data itself. The end product of this stage was a detailed thematic index of the data. This thematic index was then applied systematically to rest of the data in textual form by writing numerical codes along the margin of transcripts. This process was supplemented by writing a short text descriptor for that specific index heading. The whole data was reorganized at its respective places in thematic framework. This was followed by extraction of typologies and linked association between sub themes for generating major theme. We also mapped the logical sequencing of events. The process of mapping and interpretation was influenced by the original research objectives as well as by the themes that had emerged from the data.
Study was submitted for the ethical clearance from Institutional Human Ethic Committee (IHEC) AIIMS Bhopal. IHEC AIIMS Bhopal approved the study methodology and gave ethical clearance to conduct the study.
Results
The major codes were grouped into seven major categories and further to five sub themes related with ignorance, meaninglessness, misconceptions, difficult intake and suboptimal delivery mechanism. All these sub theme further converged into a theme [Table/Fig-1] which emphasized informational discontinuity as the major factor responsible behind IFA discontinuation.
Thematic analysis showing the emerging categories, sub themes and major theme.
| Code | Categories | Sub theme | Theme |
|---|
| Lack of knowledge about anaemia | Absolute ignorance | The eyes don’t see what the mind doesn’t know | Informational discontinuity concluding into misperception and discontinuation |
| Lack of knowledge about pills |
| Lack of knowledge about consuming IFA in apparently healthy condition | Relative ignorance |
| Lack of knowledge about duration of taking pills |
| Perceived intolerable side effect (nausea/vomiting) | Perceived difficulty due to adverse event | Perceived side effects promoting discontinuation |
| Perceived intolerable side effect (others) |
| Perceived ill defined side effect/misconceptions |
| Casual attitude about IFA tablets | Self perceived meaninglessness | Imaginary lack of utility contributing to irregular intake of IFA |
| Self perceived trivial importance of IFA supplementation |
| Perceived intake of IFA at antenatal period only | Misconception about IFA for curative purpose only | Erroneous concepts for equating IFA as ’medicine’ and not as ’supplement’ |
| Restricted to sick only |
| Non availability of IFA | System delivery mechanism | Delivery mechanism perceived as suboptimum and non critical for restoring health |
| Dissatisfaction with services |
| Social taboo | Macro environmental issues |
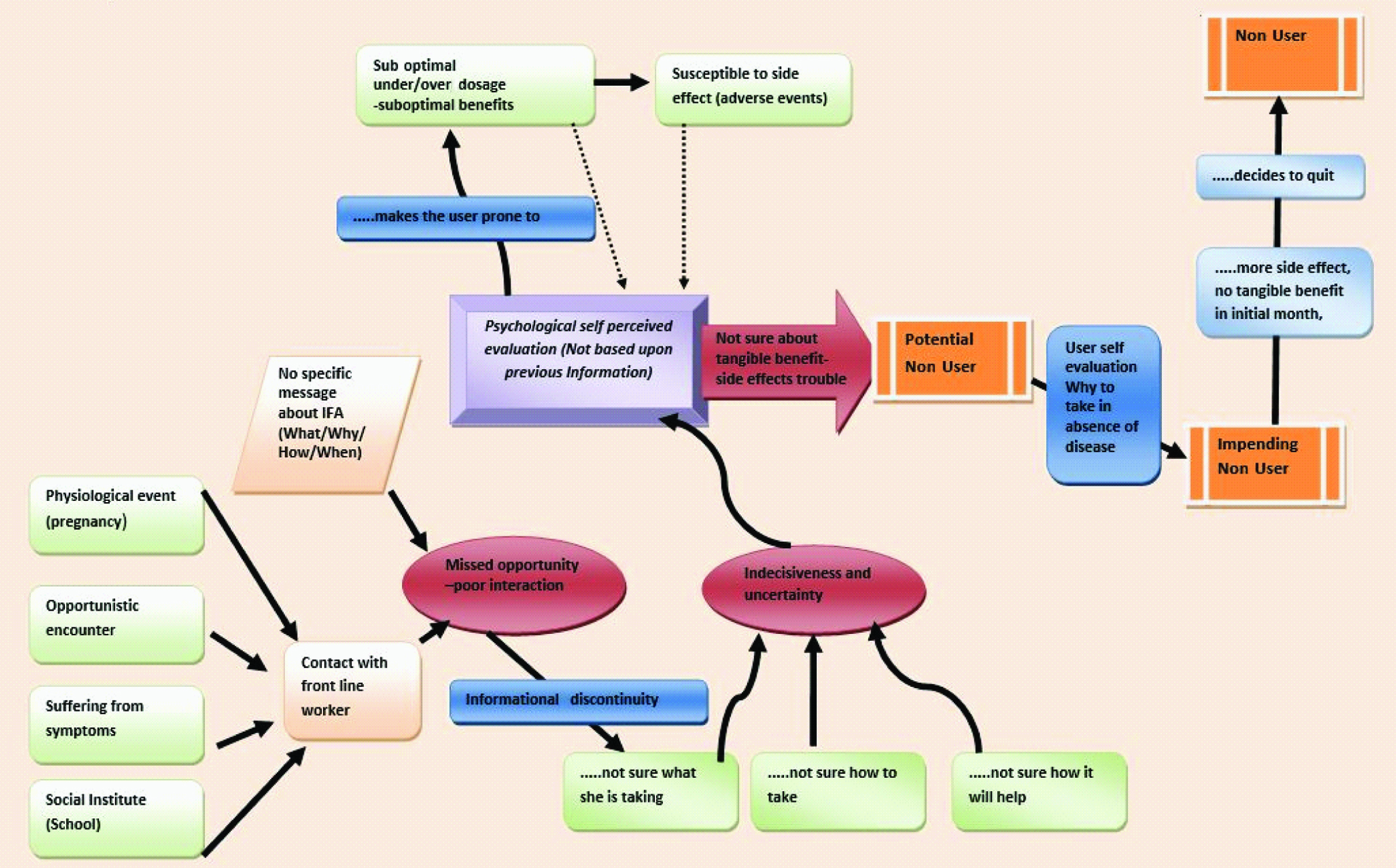
This study recognizes four types of IFA consumption patterns as per user experiences with IFA and names them persistent user, potential non user, impending non user and absolute non user as described under:
Persistent user- A persistent user is a well informed user who is able to rationalise his IFA consumption by sufficient background information. He is aware about ‘deficiency of blood’ in the body and how IFA will rectify this deficiency.
A 28-year-old pregnant lady says, “One can feel faintness andghabrahat through deficiency of blood. If I continue to take these medicines, this will not happen to me.” Interestingly, these users in initial phases also faced the similar side effect as of non users but they perceive the overall experiences more soothing and satisfactory. Another persistent IFA user (16-year-old adolescent) says-“Initially I used to feel like vomiting after taking these pills but now it seems that medicine is good. I feel weakness no longer.”
Potential non users: A person who is consuming IFA as it was suggested during the active and passive encounter with the health system, however this offering was not supplemented by adequate information about benefits, schedules and after events of medications. The user starts consuming it with an element of uncertainty and confusion and soon after begins to face the side effects.
A primigravida of 19 year says-‘I don’t know for what I am taking this medicine. Madam told me you have to take it after food.’ Another consumer (15-year-old school going girl) says-‘I feel like vomiting while taking this medicine. It feels hot at my stomach.’
Impending non user: This is considered to be the next stage towards defaulting, where with the background of patchy fragmented information and encountered side effects, the user tries to re-evaluate her decision and thinks (an Antenatal Female (ANC) with a history of missed abortion): ‘I took this medicine for one month. I have stopped it since last 15 days as it causes trouble in my stomach. Why to take it, I am fine without it. This happened to me last time as well’. Another example (a school girl of 9th standard) is,‘I don’t know from what it will prevent me. I am taking it because I was told so. I have stopped it in between…. I am not sure whether I will be taking it in future’.
Absolute non users: As side effects continue to trouble the indecisive user (in the absence of any perceptible benefits at the earlier stages of consumption) gradually decides to quit as the user perceive him/her as apparently healthy and doesn’t realize any further need to consume it.
Here is a relevant verbatim from a post partum female of 27 years: ‘I was told to take three tablets in a day. Then I started vomiting… I had to quit as I was better without them.’ A first-time pregnant lady of 20 years says, ‘I don’t know anything about anaemia. I am fine and can perform all household duties. When these tablets started troubling me I stopped them’.
All these milestones, associated events and concerns for a ‘less’ informed user are mapped in the diagram [Table/Fig-2] which tries to logically connect the non liner events for further sense making.
From adherence to defaulting: The journey of an ill informed user.
Discussion
The non consumption of IFA in this study was found to be attributed mainly to ‘informational discontinuity’. The enormous difference in between expected and actual information can be explained through several biopsychosocial models of diseases (or a condition of health). All of them take into account the active roles of individual’s belief, behaviour, coping and his social environment for determining his health status. These beliefs and behaviours around a health related phenomenon are supposed to be as decisive as of biophysical agents or biological disturbances related to particular condition/ disease [11,12].
Health belief model states that for adapting a behaviour (IFA consumption) one has to consider two things first, the disease that will be averted (anaemia) by adopting the positive behaviour which is indeed a severe disease and secondly that he himself is susceptible to disease if he does not adapt the intended behaviour [13]. Hence absence of information (or disjointed information) about anaemia and role of IFA to prevent anaemia understandably makes an individual incapable to profess the susceptibility. Similarly, social attribution theory states that if a person feels his condition as changeable and under his control, there are higher chances that he will stick on that behaviour (IFA consumption) [14].
All the major sub themes emerging from this study relate with unawareness, perceived insignificance, mistaken belief, difficulty in taking IFA tablets and discontentment with system may weaken the intentions of an individual to stick on health behaviour (IFA consumption) as his (and influencers) own assessment about the gain is not supported by real facts. He may start consuming on an experimental basis but sooner stops taking in absence of concrete background information and encountered side-effects [15-17]. This notion can further be validated by the finding of several researchers in context with stages of change which states that awareness and bridging the informational gap is a pre-requirement in order to switch from pre contemplation to contemplation phase [18,19].
A review conducted on ANC group from 22 countries showed that even though IFA was consumed at least once by 95% of the participants but compliance to the ideal regimen was as low as 8% [20]. Another study from Uttar Pradesh which was conducted among adolescent group strongly concluded that proper counselling could increase the compliance as high as 85%. They further stated that counselling is even more decisive than supervision [21]. A multileveled modelling on DLHS-2008 data from Bihar also showed the higher probability of IFA consumptions after an active contact/ persuasion by the health system [8].
This study also found the instrumental role of side effects in discontinuation of IFA consumption but interestingly side effects were found to be associated with both users and non users. However, the intensity of events and resultant indecisiveness seems more with the second group as a product of fundamental ignorance about the dosage/schedules and remedial measures after meeting with such events. Heart burn, nausea, vomiting and stomach cramping are reported as the representative side effects by this study and from other part of globe as well [22,23]. Some system related issues (non availability of medicine and dis-satisfaction from services) have also emerged as associated factors for non consumption in thematic analysis. Several studies have also reported that optimization of services, uninterrupted delivery of consumers products and delivery point at the consumer’s vicinity promotes the acceptance to product and intended behaviour [23-25].
However a point of caution is that, whether system issues can be considered among the primary reasons for IFA non consumptions or there also exists an element of projection on delivery mechanism for non consumption, in order to justify the behaviour of defaulting. Several researchers have also highlighted this ‘attribution phenomenon’ [26,27].
The strength of this study lies in the approaches adapted in order to develop the paradigm to understand social phenomena (IFA consumption) in natural community settings, giving due emphasis to the meanings, experiences and views of the participants [28,29].
Limitation
In spite of the vast and rigorous methodical attention there may still be an element of personal bias and idiosyncrasies in the present study which may be considered a natural phenomenon in a qualitative inquest. Consistency of the findings is another concern, as by default a qualitative research focuses on a central and other emerging themes rather to assign a quantitative number.
Conclusion
It may be inferred at this juncture that apart from rectifying the system related concerns there seems to be an immense requirement of ‘need generation’ among potential beneficiaries. The ‘felt need’ will stimulate motivation among targeted groups and encourage them to take the decision of IFA consumption consciously and knowingly. This conscious decision making may serve as critical positive step taken by potential IFA user for consumption as well as to adhere in long terms which seems to be imperative for the success of the program at community level.
[1]. Haas JD, Brownlie T, IVIron deficiency and reduced work capacity:a critical review of the research to determine a causal relationshipJ Nutr 2001 131(2):676-90S. [Google Scholar]
[2]. Miller JL, Iron deficiency anaemia:a common and curable diseaseCold Spring Harb Perspect Med 2013 3(7):a011866 [Google Scholar]
[3]. Abbaspour N, Hurrell R, Kelishadi R, Review on iron and its importance for human healthJ Res Med Sci 2014 19(2):164-74. [Google Scholar]
[4]. Stoltzfus RJ, Dreyfuss ML, Guidelines for the use of iron supplements to prevent and treat iron deficiency anaemia 1998 Washington DCIlsi Press [Google Scholar]
[5]. Kotecha PV, Nutritional Anaemia in Young children with focus on Asia and IndiaIndian Journal of Community Medicine 2011 36(1):8-16. [Google Scholar]
[6]. Uria GA, Naik PK, Midde M, Yalla PS, Pakam R, Prevalence and severity of anaemia stratified by age and gender in rural IndiaAnaemia 2014 2014:01-05. [Google Scholar]
[7]. Joshi A, Nahar N, Phadnnis S, Biswas R, Patient-provider reciprocity as complex adaptive systemReview of Global Medicine and Health care Research 2013 4(1):208-21. [Google Scholar]
[8]. Wendt A, Stephenson R, Young M, Girard AW, Hogue C, Ramakrishnan U, Individual and facility-level determinants of iron and folic acid receipt and adequate consumption among pregnant women in rural Bihar, IndiaPLoS One 2015 10(3):e0120404 [Google Scholar]
[9]. Gale NK, Heath G, Cameron E, Rashid S, Redwood S, Using the framework method for the analysis of qualitative data in multi-disciplinary health researchBMC Medical Research Methodology 2013 13:117 [Google Scholar]
[10]. Bradley EH, Curry LA, Devers KJ, Qualitative data analysis for health services research:developing taxonomy, themes, and theoryHealth Serv Res 2007 42(4):1758-72. [Google Scholar]
[11]. Havelka M, Lucanin JD, Lucanin D, Biopsychosocial model--the integrated approach to health and diseaseColl Antropol 2009 33(1):303-10. [Google Scholar]
[12]. Dogar IA, Biopsycosocial modelAnnual of Punjab Medical College 2007 1(1):11-13. [Google Scholar]
[13]. Orji R, Vassileva J, Mandryk R, Towards an effective health interventions design:an extension of the health belief modelOnline J Public Health Inform 2012 4(3):ojphi.v4i3.4321 [Google Scholar]
[14]. Mirsadeghi S, A Review on the attribution theory in the social psychologyJournal Of Humanities And Social Science 2013 8(6):74-76. [Google Scholar]
[15]. Hyder SM, Persson LA, Chowdhury AM, Ekstrom EC, Do side-effects reduce compliance to iron supplementation?A study of daily- and weekly-dose regimens in pregnancyJ Health Popul Nutr 2002 20:175-79. [Google Scholar]
[16]. Shukla M, Agarwal M, Tsusennaro I, Rehman HM, Yadav K, Singh S, Utilization of maternal health care services in slums of Lucknow, capital of Uttar PradeshInternational Journal of Interdisciplinary and Multidisciplinary Studies 2015 2(11):23-27. [Google Scholar]
[17]. Mithra P, Unnikrishnan B, Rekha T, Nithin K, Mohan K, Kulkarni V, Compliance with iron-folic acid (IFA) therapy among pregnant women in an urban area of south IndiaAfr Health Sci 2013 13(4):880-85. [Google Scholar]
[18]. Sniehotta FF, Aunger R, French DP, Kaptein A, Vedhara K, Weinmann J, Stage model of behaviour changeHealth Psychology 2010 2nd edUKBlackwell:135-146. [Google Scholar]
[19]. Zimmerman GL, Olsen CG, Bosworth MF, A ‘stages of change’ approach to helping patients change behaviourAm Fam Physician 2000 61(5):1409-16. [Google Scholar]
[20]. Sununtnasuk C, D'Agostino A, Fiedler JH, Iron+folic acid distribution and consumption through antenatal care:identifying barriers across countriesPublic Health Nutrition 2016 19:732-42. [Google Scholar]
[21]. Vir SC, Singh N, Nigam AK, Jain R, Weekly iron and folic acid supplementation with counseling reduces anaemia in adolescent girls:a large-scale effectiveness study in Uttar Pradesh, IndiaFood Nutr Bull 2008 29(3):186-94. [Google Scholar]
[22]. Sadore AA, Gebretsadik LA, Hussen MA, Compliance with iron-folate supplement and associated factors among antenatal care attendant mothers in Misha district, south Ethiopia:community based cross-sectional studyJournal of Environmental and Public Health 2015 1:1-7. [Google Scholar]
[23]. Nisar YB, Alam A, Aurangzeb B, Dibley MJ, Perceptions of antenatal iron-folic acid supplements in urban and rural Pakistan:a qualitative studyBMC Pregnancy and Childbirth 2014 14:344 [Google Scholar]
[24]. Pal PP, Sharma S, Sarkar TK, Mitra P, Iron and folic acid consumption by the ante-natal mothers in a rural area of India in 2010Int J Prev Med 2013 4(10):1213-16. [Google Scholar]
[25]. Alam A, Rasheed S, Khan NU, Sharmin T, Huda TM, Arifeen SE, How can formative research inform the design of an iron-folic acid supplementation intervention starting in first trimester of pregnancy in Bangladesh?BMC Public Health 2015 15:374 [Google Scholar]
[26]. Sharma S, Teijlingen EV, Belizán JM, Hundley V, Simkhada P, Sicuri E, Measuring what works:an impact evaluation of women's groups on maternal health uptake in rural NepalPLoS ONE 2016 11(5):e0155144 [Google Scholar]
[27]. Idris SH, Sambo MH, Ibrahim MS, Barriers to utilisation of maternal health services in a semi-urban community in northern Nigeria: The clients’ perspectiveNiger Med J 2013 54(1):27-32. [Google Scholar]
[28]. Khan AA, Qualitative research: a case for a multi-angle view to enhance ‘validity’International Journal of Business and Management 2014 9(9):29-40. [Google Scholar]
[29]. Brown KW, Cozby PC, Kee DW, Worden PE, Research Methods in Human Development 1999 2nd edCaliforniaMayfield Publishing Company [Google Scholar]