An Unusual Radiographic Presentation of Aneurysmal Bone Cyst of the Zygoma: A Rare Case Report
GV Murali Gopika Manoharan1, Priyanka Khobre2, Jayaraman Balaji3, Mukesh Singh4
1 Professor, Department of Oral Medicine and Radiology, Tamil Nadu Government Dental College and Hospital, Chennai, Tamil Nadu, India.
2 Postgraduate Student, Department of Oral Medicine and Radiology, Tamil Nadu Government Dental College and Hospital, Chennai, Tamil Nadu, India.
3 Associate Professor, Department of Oral and Maxillofacial Surgery, Tamil Nadu Government Dental College and Hospital, Chennai, Tamil Nadu, India.
4 Postgraduate Student, Department of Oral and Maxillofacial Surgery, Tamil Nadu Government Dental College and Hospital, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Priyanka Khobre, Postgraduate, Department of Oral Medicine and Radiology, Tamil Nadu Government Dental College and Hospital, Chennai-600003, Tamil Nadu, India.
E-mail: priyankakhobre26@gmail.com
Aneurysmal Bone Cyst (ABC) is an uncommon benign lesion affecting mainly the long bones and vertebral column. Its occurrence in the maxillofacial skeleton is rare. So far only five cases of ABC in the zygoma have been reported in the literature. Radiographic features of ABC are not pathognomonic. There can be expansion of bone and it may manifest as cystic lesion with honeycomb or soap bubble appearance. There can be perforation or destruction of cortex of the bone as well. Therefore the differential diagnosis of ABC is quite conflicting with other types of maxillary bone lesions. Here we report a case of ABC in 30-year-old female, at the left zygoma region showing periosteal reaction with sunray effect, which according to the literature is the first case reported based on location and radiographic appearance.
Long bones, Maxillofacial skeleton, Radiograph, Sunray effect
Case Report
A 30-year-old female patient reported to the Department of Oral Medicine and Radiology with a chief complaint of swelling below the left eye for one year and pain associated with swelling for past one and a half months. The patient gave history of the swelling slowly increasing to the present size. The patient also gave history of trauma at the same region one and a half year back with no history of visual complaints. On extraoral examination, on inspection, marked facial asymmetry was present with a solitary, localized swelling of size 2×2 cm at superior aspect of the left zygoma with ill defined borders. Skin over the swelling was normal. The swelling was bony hard, fixed, moderately tender and non compressible on palpation. The patient was having normal vision. Correlating the history and clinical findings, the case was provisionally diagnosed as osteoma. The patient was subjected to radiological investigations. Paranasal Sinus (PNS) view revealed a localized radiopacity involving lower border of the left orbit and the left zygoma with distinct border. Maxillary sinus appeared normal [Table/Fig-1].
PNS view showing radiopacity involving lower border of the left orbit and the left zygoma.

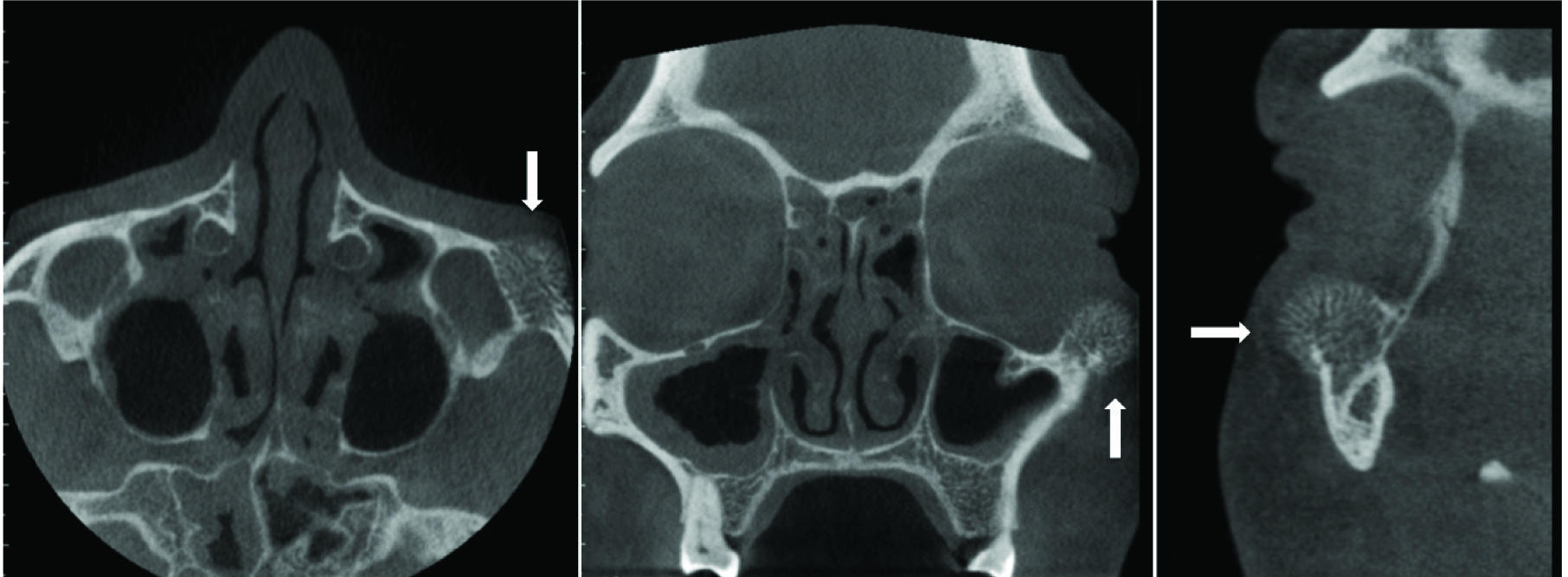
For precise evaluation, the patient was subjected to Cone Beam Computed Tomography (CBCT) with Carestream (CS 9300 of 10×10 field of view) which revealed a bony outgrowth as heterodense mass arising from superior aspect of the left zygoma lifting the infraorbital wall of the left orbit. Axial section showed expansion of the cortical plate with loss of cortical borders. Bony trabeculae perpendicular to the cortical plate were evident, suggestive of sunray pattern appearance. Coronal and sagittal sections showed expansile mass involving anterosuperior border of left zygoma. There was no extension into the maxillary sinus and infraorbital foramen [Table/Fig-2].
Axial, coronal and sagittal view of CBCT showing heterodense mass with cortical expansion and sunray pattern of periosteal reaction at the left zygoma.
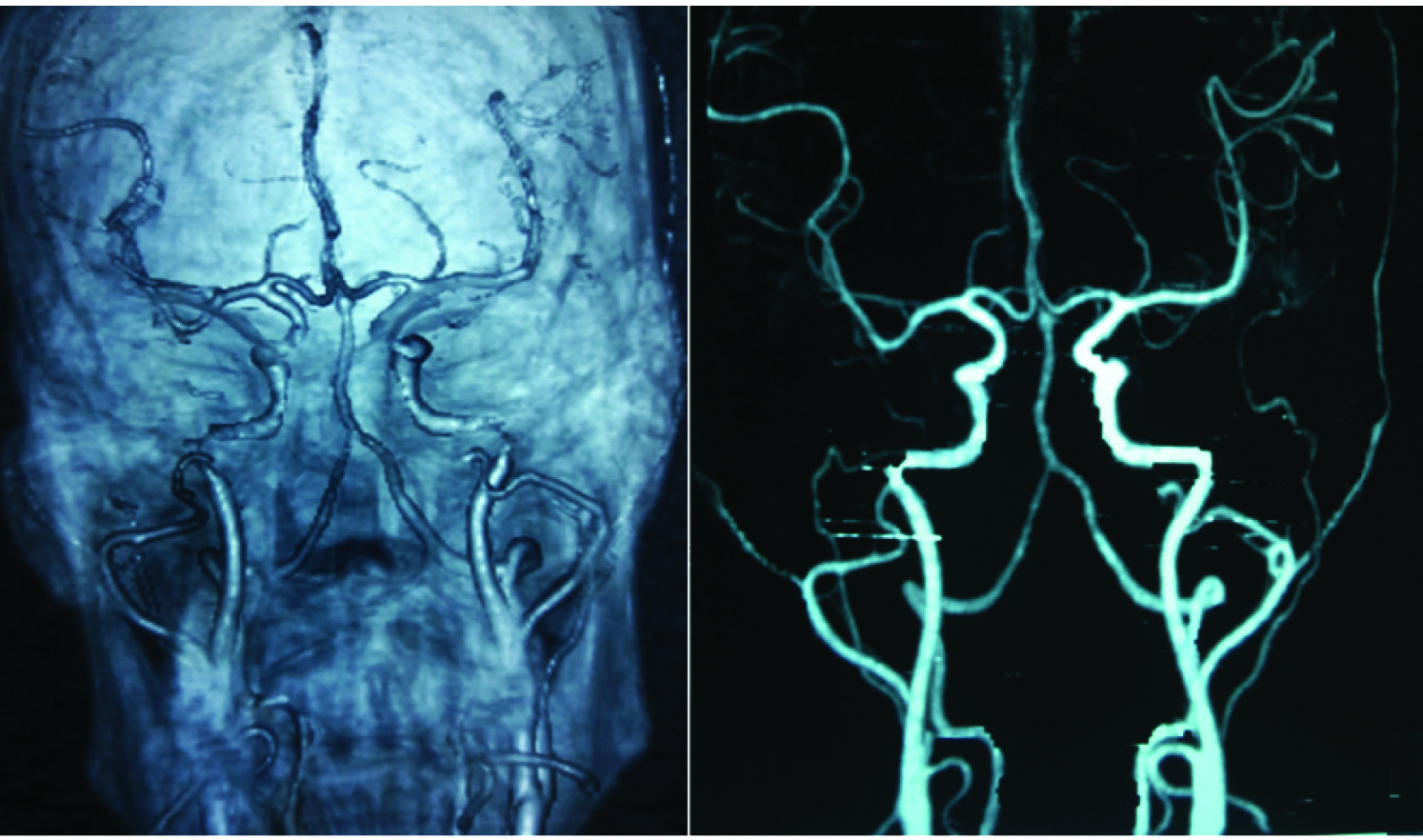
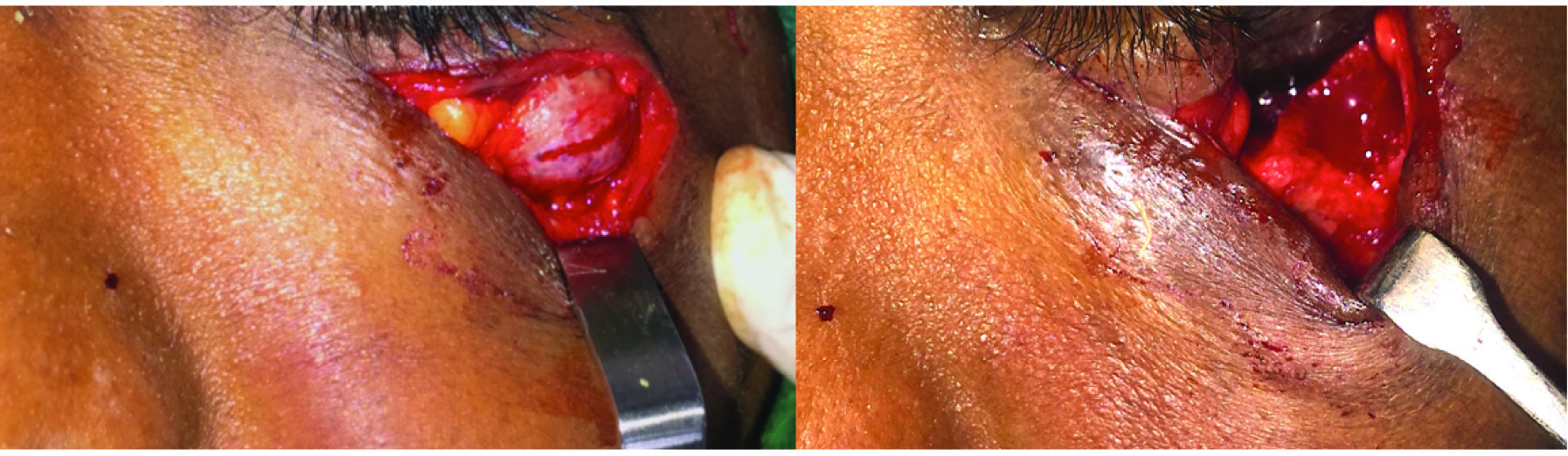
Based on radiological findings a differential diagnosis of osteoma, central haemangioma, ABC and osteosarcoma were considered. To rule out vascular malformation, Multi Detector Computed Tomography (MDCT) neck and face angiogram was done with Philips Brilliance 64 CT Scanner, which revealed no significant contrast enhancement or abnormal feeder vessels at the left zygoma region, which ruled out central haemangioma [Table/Fig-3]. Excisional biopsy of lesion was done under local anaesthesia [Table/Fig-4].
MDCT angiography with 3D reconstruction showing no abnormal feeder vessels at the left zygoma.
Intraoperative images showing exposure of the lesion (left) and bone cavity after excision of lesion (right).
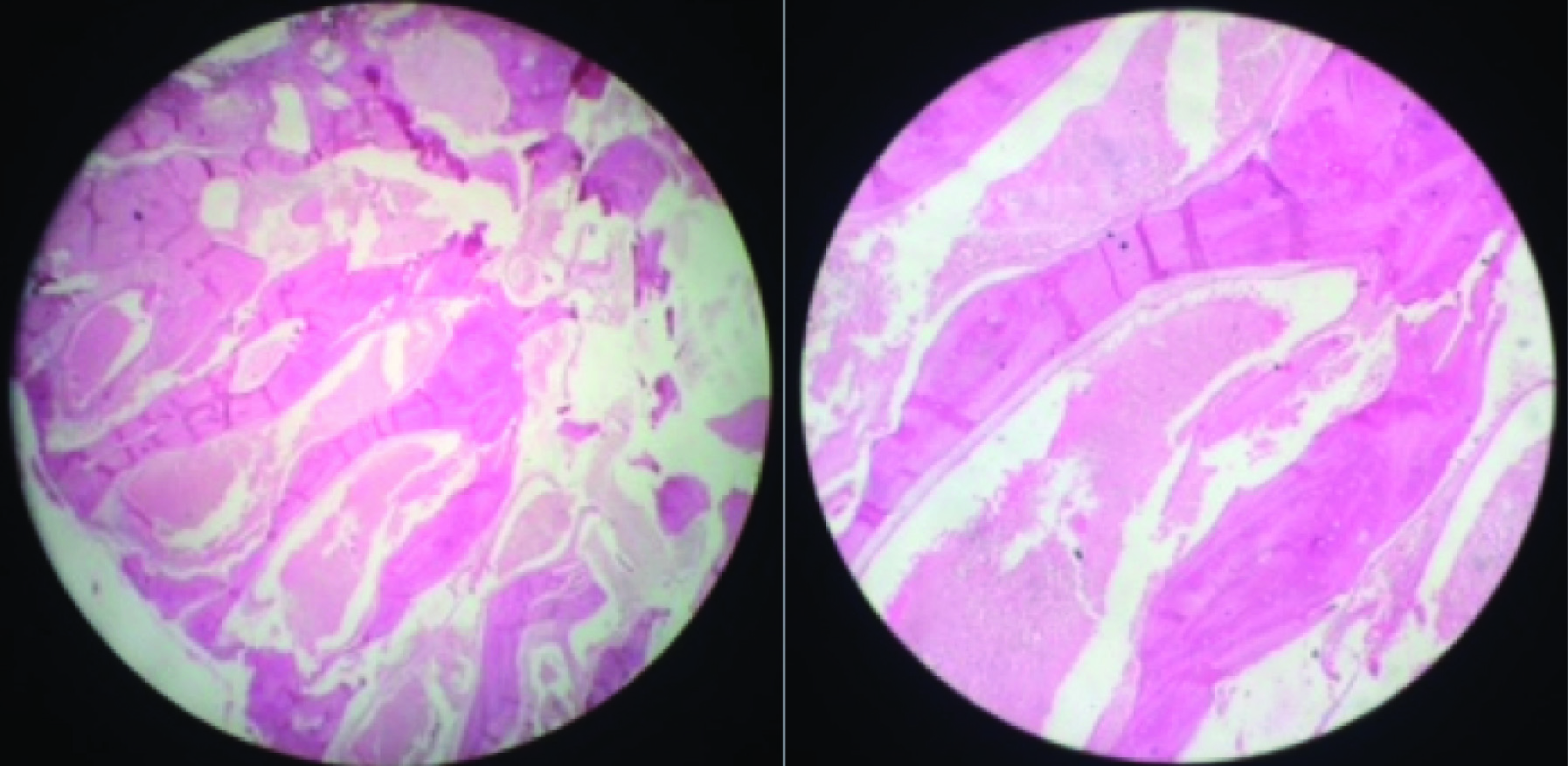
Histopathology showed sinusoidal spaces filled with numerous RBC’s. The spaces were separated by connective tissue stroma and focal areas showing bone formation. Extravasated RBC’s were also seen in some areas [Table/Fig-5]. These features were consistent with ABC.
Histopathology showing sinusoidal spaces filled with numerous RBC’s and separated by connective tissue stroma with focal areas of bone formation (left 4X, right 10X).
Discussion
The term ABC was first described in literature by Jaffe HL and Lichenstein L in 1942 [1]. In 1958 Bernier and Bhaskar reported the first case of ABC in the jaws [2]. The World Health Organization defines ABC as “a benign tumour like lesion with an expanding osteolytic lesion, consisting of blood filled spaces of varying size separated by connective tissue septae containing trabeculae or osteoid tissue and osteoclast giant cells” [3]. Occurrence of ABC in maxillofacial skeleton is rare and only 2% of ABCs appear in the jaws with mandible to maxilla involvement ratio of 3:1 [3,4]. Despite its name, ABC is not a true cyst because it lacks the epithelial lining and affects mainly the long bones and vertebral column [2,5,6]. ABC is rarely seen in craniofacial region and even rarer in the zygoma [7]. So far only five cases have been reported in this region [Table/Fig-6] [8-12].
Cases of ABC in the craniofacial region that have been reported in literature.
| Authors | Radiographic findings |
|---|
| Rasi HB et al., [8] | ABC presented as expansile radiolucent lesion on radiograph. |
| Carmichael F et al., [9] | ABC appeared as ‘hot’ on bone isotope scan. |
| Sozeri B et al., [10] | ABC was described as cystic vascular osseous tumour. |
| Lee JY et al., [11] | Computed tomography revealed intrabony expansile lesion and thinning of surrounding zygoma with no internal calcification. |
| Kumar LKS and Menon PV [12] | Computed tomography revealed bicortical expansile radiolucent lesion of the zygoma. |
| Present case | CBCT showed evidence of periosteal reaction and sunray pattern. |
Our case is unique because of its occurrence in the zygoma, which according to the literature is an extremely rare location. ABC is typically found in patients of age less than 20-year-old with an average age of 13 years with no gender predilection [6]. The age of patient in this case report was 30 years.
Its aetiopathogenesis remains unclear. Some authors suggested traumatic aetiology while others favored subperiosteal intraosseous haematoma as its cause. The lesion may have vascular origin according to some authors [2,6]. Development of ABC in this case may be because of trauma to that region.
The clinical appearance can vary from asymptomatic, small lesion to rapidly enlarging, destructive lesion with complaint of pain, deformity and cortical perforation [2].
Radiologic signs associated with ABC of the jaws are not pathognomonic [3]. Cyst manifests as expansion of bone with honeycomb or soap bubble like internal structure. There can be perforation or destruction of cortex of the bone. Sometimes periosteal reaction and sunray effect, mimicking osteosarcoma can also be seen [13,14]. Our case also shows evidence of periosteal reaction and sunray pattern, which is a very rare presentation of ABC radiographically. Goaz PW and White SC described three stages of development of ABC, which determine its radiological appearance: 1) an initial stage characterised by a defined but not corticated lytic area; 2) a growth stage, showing an enlarged area of bone destruction; and 3) a mature stage, exhibiting bony expansion, cortication and faint septa coursing through the lesion in a random pattern [15]. The appearance of sunray pattern in this case may be due to the faint septae.
Histopathology of ABC has been described into three types. Vascular type (95%) is having loose scanty stroma with large number of caverns and blood filled sinusoids. During surgery, there can be risk of active bleeding. Solid type (5%) having dense stroma and consist of few blood vessels and caverns. There will be less chance of active bleeding during surgery. Mixed type has characteristics of both variants [6]. In our case, histopathological differential diagnosis of central haemangioma and Brown tumour of hyperparathyroidism were also considered. However angiography ruled out central haemangioma. Brown tumour of hyperparathyroidism was also ruled out based on clinical, biochemical and radiographic investigations.
Treatment options includes curettage, wide en bloc resection and reconstruction, systemic calcitonin therapy, percutaneous sclerotherapy and radiation therapy. Angiography with embolisation of feeder vessels preoperatively has been advocated to avoid bleeding during surgery [6,16]. In our case, excisional biopsy was performed, because of this small size of lesion. Patient was advised regular follow up and so far no recurrence of lesion was noticed.
Conclusion
ABC represents a pseudocyst with variable clinicoradiological and histological features often posing a diagnostic dilemma. To the best of our knowledge, there is no other case reported with this unusual sunray effect in ABC of the zygoma.
[1]. Jaffe HL, Lichtenstein L, Solitary unicameral bone cyst. With emphasis on roentger picture, the pathological appearance and the pathogenesisArch Surg 1942 44:1004-25. [Google Scholar]
[2]. Bharadwaj G, Singh N, Gupta A, Anand K, Sajjan AK, Giant aneurysmal bone cyst of the mandible: A case report and review of literatureJ Maxillofac Surg 2013 4:107-10. [Google Scholar]
[3]. An SY, Aneurysmal bone cyst of the mandible managed by conservative surgical therapy with preoperative embolizationImaging Sci Dent 2012 42:35-39. [Google Scholar]
[4]. Devi P, Thimmarasa VB, Mehrotra V, Agarwal M, Aneurysmal bone cyst of the mandible: A case report and review of literatureJ Oral Maxillofac Pathol 2011 15:105-08. [Google Scholar]
[5]. Haft GF, Buckwalter JA, Aneurysmal Bone Cyst Following Tibial Fracture: A Case ReportIowa Orthop J 2003 23:100-02. [Google Scholar]
[6]. Verma RK, Kumar R, Bal A, Panda NK, Aneurysmal bone cyst of maxilla with ectopic molar tooth – A case reportOtolaryngologiapolska 2013 67:302-07. [Google Scholar]
[7]. Prasad S, Raghaviah AM, Sharma N, Einstein A, Saraswathi TR, Aneurysmal bone cyst of the mandible: Report of a case and review of the literatureJOMFP 2007 11:38-41. [Google Scholar]
[8]. Rasi HB, Swamy PT, Alpert LJ, Giovanniello J, Aneurysmal bone cyst of zygomaN Y State J Med 1978 78:1937-41. [Google Scholar]
[9]. Carmichael F, Malcolm AJ, Robert A, Aneurysmal bone cyst of the zygomatic boneOral Surg Oral Med Oral Pathol 1989 68:558-62. [Google Scholar]
[10]. Sozeri B, Sennaroglu L, Yilmaz T, Aneurysmal bone cyst of the zygoma, a case report and review of literatureActa Otorhino laryngol Belg 2000 54:483-86. [Google Scholar]
[11]. Lee JY, Ko YI, Kwon H, Jung SN, Aneurysmal bone cyst of the zygomatic boneJ Craniofacsurg 2014 25:148-49. [Google Scholar]
[12]. Kumar LKS, Menon PV, Aneurysmal bone cyst of the zygomatic boneOral Surgery 2017 10:48-51. [Google Scholar]
[13]. Capote-Moreno A, Acero J, Garcia-Recuero I, Ruiz J, Serrano R, de Paz V, Giant aneurysmal bone cyst of the mandible with unusual presentationMed Oral Patol Oral Cir Bucal 2009 14:137-40. [Google Scholar]
[14]. Lopez-Arcas-Calleja JM, Cebrian-Carretero JL, Gonzalez-Martin J, Burgueno M, Aneurysmal bone cyst of the mandible: Case presentation and review of the literatureMed Oral Patol Oral Cir Bucal 2007 12:401-03. [Google Scholar]
[15]. Goaz PW, White SC, In: Oral radiology: Principles and interpretation 1994 3rd edSt. Louis, MOCV Mosby:518-33. [Google Scholar]
[16]. Goyal A, Tyagi I, Syal R, Agrawal T, Jain M, Primary aneurysmal bone cyst of coronoid processBMC Ear, Nose and Throat Disorders 2006 6:4 [Google Scholar]