Management of an Unusual Ectopic Eruption of Maxillary Canine
Kaladhar Reddy Aileni1, Madhukar Reddy Rachala2, Chintakunta Reddy Prathima3, Pitalla Kumar Naveen4, Donthula Soujanya5
1 Professor and Head, Department of Orthodontics and Dentofcaial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
2 Professor, Department of Orthodontics and Dentofcaial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
3 Post Graduate Trainee, Department of Orthodontics and Dentofcaial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
4 Post Graduate Trainee, Department of Orthodontics and Dentofcaial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
5 Post Graduate Trainee, Department of Orthodontics and Dentofcaial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Chintakunta Reddy Prathima, Post Graduate Trainee, Department of Orthodontics and Dentofcaial Orthopedics, SVS Institute of Dental Sciences, Mahabubnagar-509002, Telangana, India.
E-mail: prathimachintakunta@gmail.com
Transposition of teeth is a rare condition, with a prevalence of 0.3-0.4% in general population. They are more commonly observed in females, and may occur unilaterally/bilaterally with greater frequency of left side occurrence in unilateral transposition cases. A 17-year-old female patient reported with the chief complaint of unaesthetic smile. On clinical examination the patient was diagnosed with Angle’s class I malocclusion with an ectopically erupted maxillary left canine labial to the left central incisor with retained deciduous canine. The treatment plan decided was to extract the retained deciduous canine, level and align the ectopic canine using an R-loop. The treatment for the patient was finished in 14 months and was retained using a fixed lingual retainer in the upper and lower arches.
Ectopic canine, R- loop, Unaesthetic, Unilateral transposition
Case Report
A 17-year-old female patient came to the Department of Orthodontics, SVS Institute of Dental Sciences with the chief complaint of unaesthetic smile. On extra oral examination, she had convex profile, competent lips with symmetric face and matching skeletal midlines. Intra oral examination revealed Angle’s class I molar relation with 2 mm of over jet and overbite; the upper dental midline was shifted to left side by 1mm. The patient had an ectopically erupted maxillary left canine labial to the left central incisor with retained deciduous canine. Panoramic and periapical radiographs showed the transmigrated canine with crown labial to central incisor and the root between the central and lateral incisor with no evidence of root resorption. The Orthopantomogram (OPG) revealed development of all the third molars in Nolla’s stage 7. Periodontal status of the ectopic canine was satisfactory. [Table/Fig-1]. The cephalometric measurements showed no abnormality in skeletal and dental parameters.
Pre-treatment extra oral and intral oral photographs with pre treatment OPG.

Proper diagnosis and treatment planning are critical while dealing with the management of such an unusual ectopic eruption of maxillary canine. The treatment options available were: 1) extraction of ectopically erupted canine and replacement with either implant/ fixed prosthesis; 2) Correcting the ectopically erupted teeth orthodontically; or 3) surgical substitution with auto-transplantation [1] may only be considered if all other treatment options cannot be implemented/had been exhausted. We decided to treat the patient orthodontically.
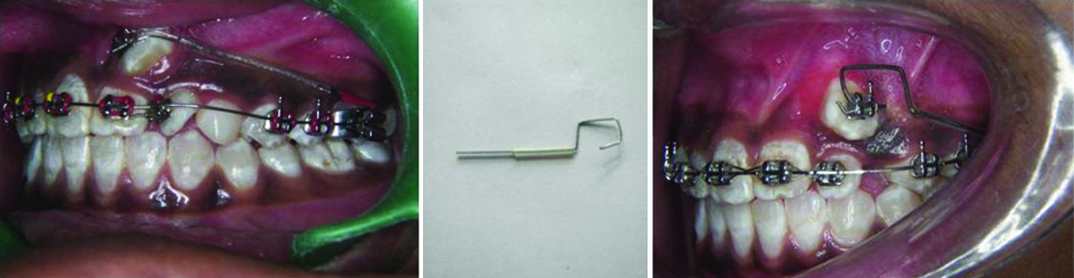
Orthodontic treatment was started with 0.022" X 0.028" Pre-adjusted edgewise system (Roth). Group A anchorage using transpalatal arch in relation to the upper was employed to facilitate only the canine movement without any counteraction on the molar tooth. Alignment and levelling were done using 0.014″, 0.018″ NiTi wires followed by 0.016 X 0.022″, 0.017 X 0.025″ & 0.019 X 0.025″ S.S wires. A light tipping force from the molar hook to canine was applied for canine derotation. After four months of treatment, the deciduous canine was extracted and the Retraction loop (R-loop) was placed on the ectopically erupted canine, when the base arch wire was 0.019X0.025″ S.S. R-loop- a type of spring, was prepared with 0.017" X 0.025" TMA wire for canine retraction, and applied from the molar auxillary tube to the bracket slot of canine for a period of six months [Table/Fig-2]. The R loop was designed such that it prevents the overriding of the root tips of canines over incisors. Once the canine was moved distal to the lateral incisor, a piggy back wire (0.016" NiTi) was placed to get the canine into the occlusion. The R-loop traction method employed for the correction of the ectopic canine facilitated in the preservation of the attached gingiva as well as the periodontal health of the tooth. A tan auxillary (0.014″ S.S) was placed for the correction of root torque of the left maxillary canine. The case was finished in 14 months including the finishing and detailing. Following debonding of the appliance, fixed lingual retainer of 0.0175″ coaxial stainless steel wire was bonded from canine to canine in both upper and lower arches.
a) with appliance; b) retraction loop; c) R-loop in place (left to right)
The gingival inflammation in relation to the canine was addressed by scaling and root planning, following which it resolved was over a period of 2-3 months. [Table/Fig-3] showing post treatment extra oral, intra oral photographs and OPG.
Post-treatment extra oral and intral oral photographs with post treatment OPG.

Discussion
Position of canine is of utmost importance as it is the corner stone of the dental arch and possesses a huge role during mandibular lateral excursion. In view of the literature available various methods for the localisation of the canine include like panoramic views, periapical view, occlusal films, posteroanterior views and lateral cephalogram. However, all these techniques help to visualise the tooth in 2-dimensions. So, 3-dimensional radiographic techniques including Computed Tomography (CT), spiral CT, Cone Beam Computed Tomography (CBCT) were introduced [2]. OPG served as a useful indicator tool for the localization of the canine and its root tip in the present case report [3,4].
The maxillary canine is the most commonly involved tooth in ectopic eruptions/ transpositions. Shapira Y and Kuftinec MM, explained this high incidence with the canine’s longest period of development and longest path of eruption [5]. Though, the mechanism for the ectopic eruption is obscure localized pathologic process, trauma, and mechanical interferences are likely the causes for the ectopic eruption and transposition. This transposition of canine can occur in the incisor, second premolar, or first molar area due to the presence of the retained deciduous canines [6]. However, according to Peck L et al., a retained deciduous tooth is a consequence of the anomaly, not its cause [7].
Peck S and Peck L examined 77 publications reporting 201 people with maxillary tooth transpositions from worldwide sources [8]. Only four cases (2%) had canine to central incisor site transposition. According to Yilmaz HH et al., the most commonly seen transposition was maxillary canine-lateral incisor than maxillary canine-first premolar [9]. Shapira Y et al., suggested that maxillary canine to central incisor site transpositions should be classified as ectopic eruptions [6]. Regardless of what the phenomenon is called, this kind of transposition is rare [10].
Curran JB and Baker CG reported a case with bilateral transposition of the maxillary canines to the central incisor area [11]. The patient reported that some teeth that were protruding labially had been removed from the central incisor area, when she was 10-year-old. A case of bilateral transpositioned maxillary canines to central incisor area was reported by Gholston R and Williams PR. The patient’s medical history comprised of two compelling episodes of traumatic injuries, where the avulsion of maxillary central incisors was reported [12]. Weeks EC and Power SM reported a case with transposed maxillary central and lateral incisors. A supernumerary tooth in the upper incisor region caused displacement of these teeth distally [13]. The case presented in this article is a rare one, where the maxillary canine was transposed labial to the existing permanent central incisor tooth. The technique of traction employed proved to be highly satisfactory, restoring patient’s aesthetics and harmonious occlusal relationships.
Conclusion
Ectopically erupting canines can result in impaction of the teeth and some potentially harmful sequelae like loss of arch length, internal and external root resorption of the impacted canine and adjacent teeth, dentigerous cyst formation, and referred pain. Extractions and surgical exposure associated with orthodontic movement of impacted canine are the main options of management. We report an orthodontic approach for repositioning an ectopically erupted maxillary canine labial to central incisor. We believe that it is possible to treat this anomaly in an efficient way via orthodontic approach. In spite of the fact that this treatment is preferred, one should dependably consider as far as possible and exclude the approaches which would harm periodontal structures or cause resorption of teeth.
[1]. Patel S, Fanshawe T, Bister D, Cobourne MT, Survival and success of maxillary canine autotransplantation: a retrospective investigationEur J Orthod 2011 33(3):298-304. [Google Scholar]
[2]. Chaushu S, Chaushu G, Becker A, The role of digital volume tomography in the imaging of impacted teethWorld J Orthod 2004 5(2):120-32. [Google Scholar]
[3]. Chaushu S, Chaushu G, Becker A, The use of panoramic radiographs to localize displaced maxillary caninesOral Surg Oral Med Oral Pathol Oral Radiol Endod 1999 88(4):511-16. [Google Scholar]
[4]. Sudhakar S, Patil K, Mahima VG, Localization of impacted permanent maxillary canine using single panoramic radiographIndian J Dent Res 2009 20(3):340-45. [Google Scholar]
[5]. Shapira Y, Kuftinec MM, Tooth transposition- a review of the literature and treatment considerationsAngle Orthod 1989 59:271-76. [Google Scholar]
[6]. Shapira Y, Kuftinec MM, Maxillary tooth transpositions: characteristic features and accompanying dental anomaliesAm J Orthod Dentofacial Orthop 2001 119:129-34. [Google Scholar]
[7]. Peck L, Peck S, Attia Y, Maxillary canine- first premolar transposition, associated dental anomalies and genetic basisAngle Orthod 1993 63:99-110. [Google Scholar]
[8]. Peck S, Peck L, Classification of maxillary tooth transpositionsAm J Orthod Dentofacial Orthop 1995 107:505-17. [Google Scholar]
[9]. Yılmaz HH, Türkkahraman H, Sayın MÖ, Prevalence of tooth transpositions and associated dental anomalies in a Turkish populationDentomaxillofacial Radiology 2005 34(1):32-35. [Google Scholar]
[10]. Shafer WG, Hine MK, Levy BM, A text book of oral pathologyPhiladephiaWB Sanders:723 [Google Scholar]
[11]. Curran JB, Baker CG, Bilateral transposition of maxillary caninesOral Surg 1973 36:905-06. [Google Scholar]
[12]. Gholston LR, Williams PR, Bilateral transposition of maxillary canines and lateral incisors. A rare conditionASDS J Dent Child 1984 51:58-63. [Google Scholar]
[13]. Weeks EC, Power SM, The presentations and management of transposed teethBr Dent J 1996 181:421-24. [Google Scholar]