Diet is known to have profound influence on overall growth and development of an individual. It also influences development and maintenance of teeth, periodontium, oral mucosa and thus, the oral cavity as a whole. Thus the oral health, like general health is dependent on food that individuals select and consume. It is therefore important that variable dietary choices among individuals and causes for this variation be fully understood [1,2].
Choice of food selected by an individual varies and there are multiple motives behind selection of particular types of food. Dietary patterns and motives for food choice can be reviewed by asking individuals about factors that guide them in their food choices. However, this information may not always be accurate. Moreover, food selection involves consideration of several factors which vary among individuals [1]. Hence, food choice motives among individuals can be appraised only if all the variable factors are taken into consideration simultaneously.
The Food Choice Questionnaire (FCQ) was thus designed to assess a range of factors that affect dietary choice and food selection among individuals [1,3,4]. FCQ consists of a total of 36 items that were designed to evaluate the importance of nine factors that were reported to shape food selection among individuals. These factors or domains were health, convenience, price, sensory appeal, natural content, mood, familiarity, ethical concern and weight control. These domains have been proven to be reliable and consistent over time [1,4].
Types of food selected by parents have an influence on general as well as oral health status of their children. Young children do not have a particular choice of their own in food selection and are usually dependant on their parents for choosing the food they eat. Parents influence children’s eating behaviours by making some foods more available than others and by acting as models of eating behaviour [5]. Thus, it is crucial to evaluate relation between parents’ motives for food choice and its effect on oral health status of their children. Correlation between motives for food choice by parents and the actual consumption of food by parents and their children might also reveal crucial information.
Records on assessment of motives for food choice and its effect on oral health are scarce and need further investigation [5-9]. There are no studies reported in literature which appraise relationship between oral health parameters of primary school children and motives for food choice among parents. Hence, the present study was conceptualized to assess oral health status of primary school children and their possible relationship with different motives for food choice among their parents in Mangalore city, India.
Materials and Methods
Ethical approval was obtained from the Institutional Ethics Committee of Manipal College of Dental Sciences, Mangalore. Thereafter, a pilot survey was conducted prior to conduction of the main study among 30 parents and their children. List of schools in Mangalore was acquired from the Block Education Officer (BEO) and simple random sampling technique was employed to select schools for present study, which has been highlighted in the flowchart [Table/Fig-1]. A list of all schools in Mangalore was obtained from BEO which eliminated the need for dividing city into blocks and hence, table of random numbers was used to select schools. Permission to conduct study at schools was obtained from Principals of participating schools.
Flow chart explaining the sampling design.
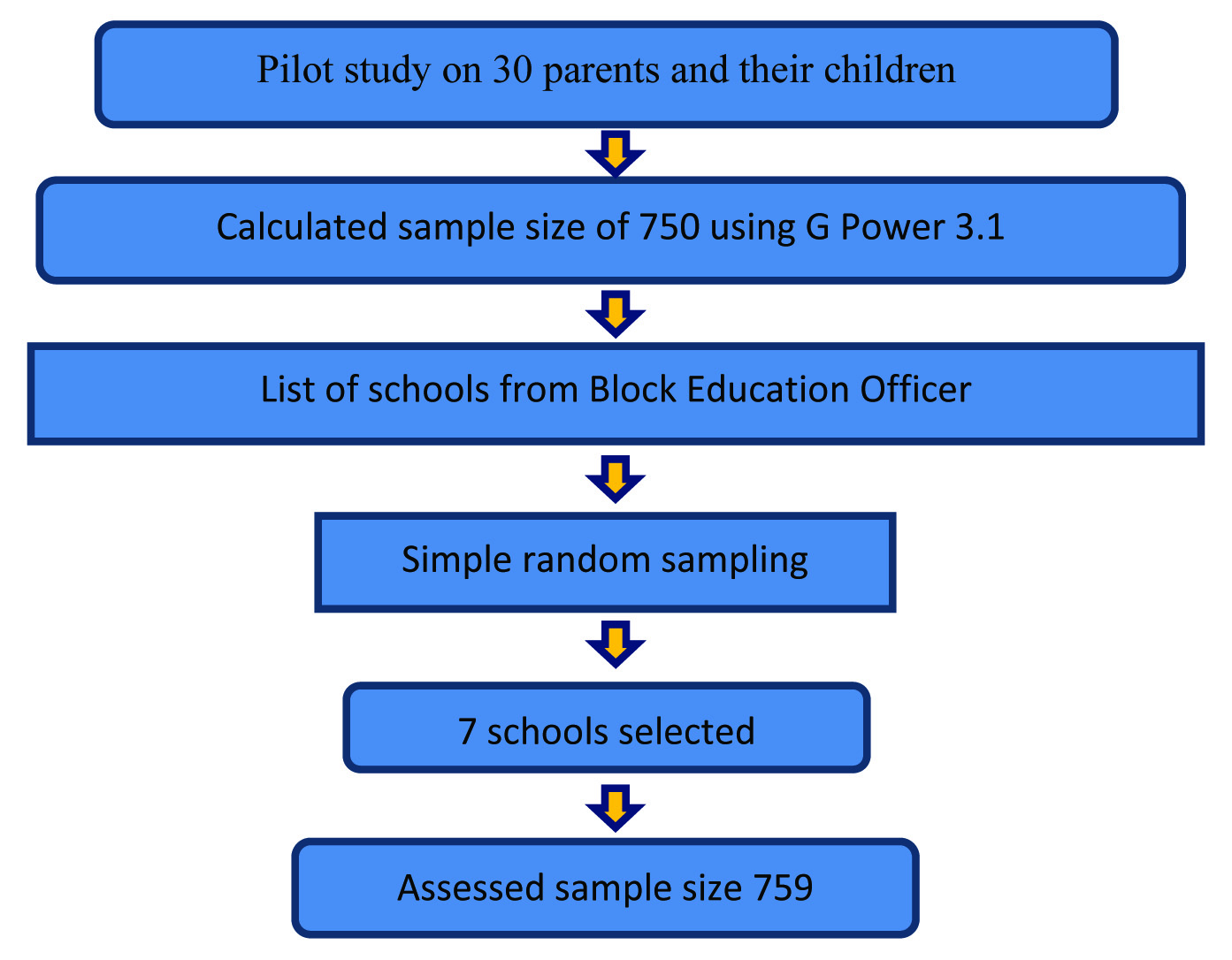
Examiner calibration was undertaken to establish intra-examiner reliability and measured using Cronbach’s alpha (α = 0.81). Sample size for present study was determined using data from pilot survey. Values from Pearson correlations between sweet scores, caries prevalence and FCQ factors were applied in the software G Power 3.1 and a sample size of 750 was obtained. Power of the study was calculated using software SPSS. Considering total FCQ scores as the dependant variable and DMFT scores in permanent dentition as fixed factor, Type II error was estimated to be 0.22 while maintaining the Type I error at 0.05 and sample size at 759. Therefore, power of the study was 78%.
Thereafter, a cross-sectional study was carried out between July 2014 and February 2015 in the coastal city of Mangalore. Inclusion criteria for current study were primary school students aged 5-10 years in Mangalore city. Parents had to be literate to provide written informed consent and to understand FCQ in English language. Children who were diagnosed or being treated for systemic diseases with known oral manifestations were excluded from present study. Confidentiality of participants as well as schools were maintained at every stage of the study.
Demographic details, oral hygiene practices of child, dietary histories of parents and their child, decay promoting potential of consumed foodstuffs and medical history of the child were obtained from parents using questionnaire method [10]. Data pertaining to motives for food choice was collected from parents of primary school children by using an FCQ. As proposed by Steptoe A et al., 36 questions of FCQ were subdivided into nine domains for valuation [4]. A four point Likert scale was used for obtaining answers and number of questions in each domain ranged from 3-6. Highest and lowest scores for a domain were not same among different domains as it was dependent on the number of questions in a particular domain. Final FCQ scores ranged from 36 to 144 [1,4].
Evaluation of oral health status of students was done by using WHO Basic Oral Health Assessment Form [11]. Oral examination of study participants was carried out by a single examiner and a trained recorder accompanied the investigator to help in recording data. Clinical examination of primary school children was done using natural light in school settings with the subject sitting on a chair. Examination was carried out beginning from maxillary right quadrant and proceeding in a clockwise direction to mandibular right quadrant.
Statistical Analysis
Data was coded and analysed using the Statistical Package of Social Sciences (SPSS) version 16.0. Comparison of questionnaire findings with oral health status was done using chi-square test and independent t-test and level of significance was fixed at p<0.05. Pearson’s correlation and binary logistic regression were used to review the factors influencing dental caries experience among primary school children. Mann Whitney U test was used for non-parametric data and Independent t-test was used for parametric data. Since our data was parametric, as suggested by Shapiro-Wilk test of normality, we used Independent t-test.
Results
Total study population for present study was 759 primary school children which consisted of 432 (56.9%) males and 327 (43.1%) females. Participants were in the age group of 5-10 years with majority of them (91.4%) belonging to Hindu religion.
Caries prevalence was found to be 10.8% and 68.9% in permanent and primary dentitions, respectively. Major part of DMFT and decayed, extracted, filled (def) was ‘decayed’ component, indicating the amount of disease burden and lack of utilization of dental treatment [Table/Fig-2]. Highest scores in FCQ were observed for the domains of ‘health’, ‘mood’ and ‘convenience’. Dental caries experience in primary as well as permanent dentition confirmed significant association with the overall FCQ scores (p<0.05) [Table/Fig-3]. Subjects with higher dental caries experience had significantly lower scores among different domains of FCQ as well as total FCQ scores (p<0.05). Relatively higher scores for FCQ were noticed among female study subjects.
Dental caries experience of the study subjects.
| DMFT scores | Total study subjects (Mean ± SD) | Male study subjects (Mean ± SD) | Female study subjects (Mean ± SD) |
|---|
| DT | 0.20 ± 0.67 | 0.18 ± 0.61 | 0.23 ± 0.75 |
| DMFT | 0.21 ± 0.72 | 0.19 ± 0.66 | 0.24 ± 0.78 |
| dt | 2.67 ± 2.85 | 2.80 ± 2.94 | 2.48 ± 2.72 |
| def | 3.08 ± 3.11 | 3.28 ± 3.28 | 2.82 ± 2.84 |
* SD: Standard Deviation
† DT - Decayed tooth index in permanent dentition
‡ DMFT - Decayed, Missing, Filled tooth index in permanent dentition
§ dt - decayed tooth index in primary dentition
||def - decayed, missing, filled tooth index in primary dentition
Food Choice Questionnaire (FCQ) scores among study subjects and association between dental caries experience and the FCQ scores.
| Domains | Total study subjects (Mean ± SD) | DMF = 0 (Mean ± SD) | DMF ≥1 (Mean ± SD) | def = 0 (Mean ± SD) | def ≥1 (Mean ± SD) |
|---|
| Health | 20.75 ± 2.75 | 21.53 ± 3.11* | 20.21 ± 3.49* | 21.77 ± 2.82* | 21.22 ± 3.30* |
| Mood | 18.49 ± 4.01 | 18.56 ± 4.05 | 17.94 ± 3.66 | 19.16 ± 3.92* | 18.22 ± 4.02* |
| Convenience | 13.55 ± 3.70 | 13.52 ± 3.72 | 13.84 ± 3.51 | 14.19 ± 3.67* | 13.29 ± 3.68* |
| Sensory appeal | 12.28 ± 2.68 | 12.24 ± 2.74 | 12.60 ± 2.19 | 12.78 ± 2.69* | 12.07 ± 2.66* |
| Natural content | 9.67 ± 2.07 | 9.78 ± 2.08* | 8.81 ± 1.79* | 9.90 ± 2.11 | 9.57 ± 2.04 |
| Price | 7.88 ± 2.26 | 7.92 ± 2.30 | 7.61 ± 1.94 | 8.14 ± 2.34* | 7.78 ± 2.23* |
| Weight control | 8.96 ± 2.24 | 9.04 ± 2.22* | 8.29 ± 2.27* | 9.18 ± 2.33 | 8.87 ± 2.19 |
| Familiarity | 8.13 ± 2.26 | 8.13 ± 2.28 | 8.12 ± 2.08 | 8.48 ± 2.32* | 7.99 ± 2.22* |
| Ethical concern | 8.00 ± 2.52 | 8.06 ± 2.52* | 7.47 ± 2.49* | 8.36 ± 2.41* | 7.84 ± 2.55* |
| Total | 104.75 ± 16.84 | 108.82 ± 17.32* | 104.91 ± 15.59* | 112.01 ± 17.69* | 106.88 ± 16.74* |
Unpaired t-test was used for this table along with descriptive statistics
Significance, p < 0.05
†FCQ: Food Choice Questionnaire
‡ SD: Standard Deviation
§ DMFT - Decayed, Missing, Filled tooth index in permanent dentition
|| def - decayed, missing, filled tooth index in primary dentition
Significantly higher mean scores for dental caries were observed in primary dentition of younger age group (p<0.05). While religion showed significant association with dental caries experience, gender was not associated with dental caries experience in either dentition. It was notable that though the highest income group demonstrated lower dental caries experience than the lowest income group, it was significantly higher as compared to other income groups (p<0.05) [Table/Fig-4].
Association between dental caries experience of study subjects and demographic variables and annual family income.
| Caries experience | Age groups | Religion | Annual family income (in lacs) |
|---|
| 5-7 | 8-10 | Hindus | Others | < 2 | 2 - 5 | 5 – 10 | ≥10 |
|---|
| DMFT (Mean ± SD++) | 0.03 ± 0.18 | 0.35 ± 0.91 | 0.18 ± 0.66* | 0.55 ± 1.10* | 0.31 ± 0.93 | 0.17 ± 0.63 | 0.11 ± 0.42 | 0.15 ± 0.36 |
| def (Mean ± SD++) | 3.51 ± 3.56 | 2.76 ± 2.67 | 3.04 ± 3.13 | 3.52 ± 2.81 | 3.46 ± 3.15* | 2.69 ± 2.77* | 2.28 ± 3.13* | 3.10 ± 4.14* |
| DT (Mean ± SD++) | 0.03 ± 0.18 | 0.33 ± 0.86 | 0.17 ± 0.61* | 0.55 ± 1.10* | 0.30 ± 0.89 | 0.15 ± 0.56 | 0.11 ± 0.42 | 0.15 ± 0.36 |
| dt (Mean ± SD++) | 3.11 ± 3.29* | 2.33 ± 2.42* | 2.60 ± 2.86* | 3.35 ± 2.74* | 3.00 ± 2.91* | 2.33 ± 2.54* | 1.96 ± 2.78* | 2.65 ± 3.58* |
Unpaired t-test and Analysis of Variance (ANOVA) were used along with descriptive statistics
Significance, p < 0.05
†† SD: Standard Deviation
‡ DT - Decayed tooth index in permanent dentition
§DMFT - Decayed, Missing, Filled tooth index in permanent dentition
|| dt - decayed tooth index in primary dentition
** def - decayed, missing, filled tooth index in primary dentition
Significant negative correlation was observed between dental caries experience in permanent dentition and the domains of ‘health’, ‘natural content’ and ‘weight control’. Similarly, significant negative correlation was detected between dental caries experience in primary dentition and the domains of ‘mood’ and ‘ethical concern’ (p<0.05) [Table/Fig-5]. Binary logistic regression was used to evaluate dental caries experience in relation to FCQ scores, sex, socio-economic variables and dietary patterns. Study subjects with mothers undertaking small-scale jobs had significantly lesser caries experience in primary dentition (p=0.04). Also, an increase in annual family income significantly increased caries experience among study subjects (p=0.01) [Table/Fig-6].
Correlation between dental caries experience and the Food Choice Questionnaire (FCQ).
| Caries experience | Health | Mood | Convenience | Sensory appeal | Natural content | Price | Weight control | Familiarity | Ethical concern |
|---|
| DMFT | -0.09* | -0.03 | 0.00 | 0.05 | -0.11* | -0.1 | -0.08* | 0.02 | -0.04 |
| def | 0.00 | -0.04* | -0.02 | -0.03 | -0.02 | 0.02 | 0.00 | -0.01 | -0.07* |
| DT | -0.09* | -0.03 | 0.00 | 0.06 | -0.12* | -0.02 | -0.10* | 0.01 | -0.04 |
| dt | -0.03 | -0.07* | -0.05 | -0.02 | -0.04 | -0.00 | -0.01 | -0.03 | -0.09* |
Pearson’s correlation analysis was used for this table
Significance, p < 0.05
†FCQ: Food Choice Questionnaire
‡ DT - Decayed tooth index in permanent dentition
§DMFT - Decayed, Missing, Filled tooth index in permanent dentition
|| dt - decayed tooth index in primary dentition
** def - decayed, missing, filled tooth index in primary dentition
Binary logistic regression analysis for primary dentition of study subjects.
| Variables | Regression coefficient | Wald test | Significance | Odd’s Ratio | 95 % Confidence Intervals |
|---|
| Lower | Upper |
|---|
| Total FCQ score | -0.02 | 9.09 | 0.00* | 0.98 | 0.96 | 0.99 |
| Sex | -0.11 | 0.31 | 0.57 | 0.89 | 0.60 | 1.32 |
| Education of mother | -0.34 | 2.06 | 0.15 | 0.70 | 0.44 | 1.13 |
| Occupation of mother | -0.39 | 2.84 | 0.04* | 0.67 | 0.42 | 0.96 |
| Education of father | 0.36 | 2.23 | 0.13 | 1.43 | 0.89 | 2.31 |
| Occupation of father | 0.02 | 0.01 | 0.92 | 1.02 | 0.68 | 1.52 |
| Annual family income | 0.53 | 5.81 | 0.01* | 1.70 | 1.10 | 2.62 |
| Type of diet for child | -0.08 | 0.17 | 0.67 | 0.91 | 0.61 | 1.37 |
| Sweet score of child | -0.31 | 2.30 | 0.12 | 0.73 | 0.48 | 1.09 |
Binary logistic regression was used for this table
Significance, p < 0.05
Discussion
Present study was an attempt to assess motives for food choice among parents and its impact on oral health status of their children aged 5-10 years, attending primary schools in Mangalore city. The present study measured impact of environmental factors like demographics and also, parental economic and occupational status on oral health status of their children.
Dental caries experience of study subjects were considered separately for primary and permanent dentitions. Prevalence of dental caries in primary dentition was 68.9%. This was in accordance to findings reported by Joshi N et al., Mittal M et al., and Saravanan S et al., in Indian primary school children [12-14]. Mean scores for def and decayed component of def were 3.08±3.11 and 2.67±2.85 respectively, which indicated the high proportion of untreated decayed primary teeth among study subjects. Dental caries prevalence in permanent dentition was noted at 11.2 %. These findings were in contrast to the findings of Saravanan S et al., and Das D et al., among primary school children in coastal Indian cities [14,15]. As literature alludes that caries experience in permanent dentition escalates significantly with an increase in age, lower caries experience in the present study might be credited to lower duration of exposure of permanent teeth in oral cavity. However, it was notable that mean DMFT scores of 0.21±0.72 were comparable to mean DMFT scores of 0.16±0.59, as reported by Sakeenabi B et al. [16].
Dental caries experience in primary and permanent dentitions were found to be inversely related to annual family income. These findings were similar to the ones reported by Moimaz SA et al., among children attending public institutions of Southern Brazil [17]. Ravera E et al., and Sufia S et al., also expressed significant decrease in caries experience among urban primary school children with an increase in family income [18,19]. Conversely, Cortellazzi KL et al., reported no significant association between dental caries experience in preschool children and their family income [20]. Investigators have reported significant association between dental caries and annual family income despite the differences in study designs and socio-demographic factors. Thus, the difference in findings of Cortellazzi KL et al., could be attributed to caries assessment in a preschool population rather than the school going population [20].
Increase in number of decayed teeth among study subjects was significantly associated with a decrease in FCQ scores and thus, with the feebler food choice of parents. This could be based on the hypothesis that a motivated parent may choose foods that are less cariogenic and eventually result in better dental health of their children. Correlation analysis between dental caries and total FCQ scores was observed to be non-significant. Nevertheless, domains such as ‘health’, ‘natural content’ and ‘weight control’ showed statistically significant inverse correlation with dental caries experience. This was comparable to findings of Oellingrath IM et al., and Russel CG et al., who independently evaluated parental motives for food choice with children’s eating patterns and food preferences, respectively [21,22]. However, while evaluating individual differences in everyday food choice motives, Pula K et al. did not find significant correlation for the above mentioned domains [23]. This could be due to different motives for food choice among individuals as consumers and, as parents.
Binary logistic regression was used to evaluate dental caries experience in relation to FCQ scores, sex, socio-economic variables and dietary patterns. An increase in total FCQ score and mothers having small-scale jobs had a positive impact on primary teeth decay. It could be formulated that mothers having small-scale jobs might have more time for food selection and supervision of the dietary patterns of their children. Also, increase in annual family income displayed negative influence on decay of primary teeth among the study subjects. This might be in part due to increased consumption of insoluble carbohydrates’ rich processed and canned foods, with an increase in the family income.
An inherent limitation of present study was the cross-sectional design which does not give any insight into causality. Study population consisted of only school children and thus, these findings could not be extrapolated to other populations and/or other contexts. Social desirability bias and lack of thorough understanding might alter answering patterns of parents of study subjects.
Findings of present study have important implications pertaining to diet and dental caries. In a developing economy like India, people take several factors into account while selecting food. Parents belonging to lower socio-economic status may be unaware about the impact of diet on oral health. Despite some parents having adequate knowledge about dietary benefits and its impact on oral and general health, they might not be able to choose foods that would be considered as ‘healthy’. It is responsibility of public health professionals to understand barriers, identify risk factors for poor food choices, target interventions and formulate ways by which the desired behaviour can be achieved. It is important to motivate parents and help them realize dietary value of the foods they select. Moreover, oral health is influenced by a variety of factors like diet, hygiene, habits, stress, trauma etc. Since a number of other chronic diseases are also affected by these factors, accepting a collective approach over disease specific approach seems judicious. Hence, the implementation of common-risk factor approach appears to be more suitable as it might help to counter the effects of risk factors that are common to several conditions [24,25].
Primary school children are dependent on their parents for their food choices. It is essential that parents inculcate the behaviour of healthy eating in their children at a young age in order to reap the benefits of a healthy life at a later stage. Thus, it is important for parents to be determined to select foods that do not hamper oral and general health of their children. Appropriate diet counselling and oral health education might help to motivate and guide parents about future implications of their food choices. Dental practitioners and public health dentists must be willing not only to provide dental care to patients but also to educate them regarding the importance of regular dental care, and promote attitudinal changes towards a positive health-seeking behaviour. Mobile dental clinics, dental camps, and dental outreach programs might help to spread awareness about diet and its impact on oral health, apart from disseminating treatment among the population.
The present study was a cross-sectional study and hence, assessment of the population might not be precise and accurate. A longitudinal study is essential in order to comprehend the findings of correlation and regression analysis. Since the present study involves use of questionnaire surveys, it might involve bias like social desirability bias and memory bias.
Conclusion
Overall, dental caries experience was found to be high among the study population. Parental food choice motives had positive influence on dietary patterns and dental status of their children. Understanding the barriers, identification of risk factors for poor food choices and targeting interventions might formulate ways by which desired behaviour can be achieved.
* SD: Standard Deviation† DT - Decayed tooth index in permanent dentition‡ DMFT - Decayed, Missing, Filled tooth index in permanent dentition§ dt - decayed tooth index in primary dentition||def - decayed, missing, filled tooth index in primary dentition
Unpaired t-test was used for this table along with descriptive statistics
*Significance, p < 0.05
†FCQ: Food Choice Questionnaire‡ SD: Standard Deviation§ DMFT - Decayed, Missing, Filled tooth index in permanent dentition|| def - decayed, missing, filled tooth index in primary dentition
Unpaired t-test and Analysis of Variance (ANOVA) were used along with descriptive statistics
*Significance, p < 0.05
†† SD: Standard Deviation‡ DT - Decayed tooth index in permanent dentition§DMFT - Decayed, Missing, Filled tooth index in permanent dentition|| dt - decayed tooth index in primary dentition** def - decayed, missing, filled tooth index in primary dentition
Pearson’s correlation analysis was used for this table
*Significance, p < 0.05
†FCQ: Food Choice Questionnaire‡ DT - Decayed tooth index in permanent dentition§DMFT - Decayed, Missing, Filled tooth index in permanent dentition|| dt - decayed tooth index in primary dentition** def - decayed, missing, filled tooth index in primary dentition
Binary logistic regression was used for this table
*Significance, p < 0.05