Choosing the correct ETT size is important in paediatric patients because an inappropriately large sized tube may cause damage to the airway, post extubation stridor, subglottic stenosis. On the other hand, a smaller tube will increase the resistance to gas flow, risk of aspiration, insufficient ventilation, poor monitoring of end tidal gases and the need to re-intubate with a different size of tracheal tube [1,2].
The cricoid cartilage being the narrowest diameter of the upper airway plays an important role for the selection of the appropriate size of ETT in paediatric patients [1,3]. Various methods based on age, weight, height and finger size have been traditionally used as prediction parameters for the selection of ETT size. However, these methods are not always suitable because the size of the airway varies considerably between patients and the smallest diameter cannot be reliably predicted by height or weight [4]. Clinically, when air leakage around the ETT occurs at 10–30 cm of water, the size of the tracheal tube is considered to be appropriate [2,5]. To know the airway diameter, especially using a bedside non-invasive tool, could be helpful in anaesthesia and intensive care [3].
USG is a reliable, safe, non-invasive, pain free and real-time modality for evaluation of the upper airway’s narrowest transverse diameter at the subglottic region and may be helpful to estimate the proper size of ETT [1,2].
Keeping this in mind, a prospective observational study was planned for a period of one year from January 2015 to December 2015 with an aim to assess the narrowest transverse diameter of the trachea at the subglottic region by USG, to estimate the ETT size and its comparison with physical indices based formulae.
Materials and Methods
Institutional ethical committee approval was obtained. Based on power of the study being 80% and confidence interval of 95%, considering a clinically meaningful difference of 0.5 and standard deviation of 1 (double of the clinically meaningful difference), sample size was 62. Adding 10%, keeping in mind the non-cooperative children and other limitations, we considered a sample size of 75.
After obtaining parental/guardian consent and applying exclusion criteria, 75 paediatric patients were enrolled in the prospective observational clinical study aged between one and 14 years. The inclusion criteria were American Society of Anaesthesiologists Physical Status (ASA) I and II patients scheduled for elective surgery under general anaesthesia with orotracheal intubation, and exclusion criteria were patients with an anticipated difficult airway, delayed milestones, pre-existing laryngeal or pharyngeal pathology, unstable cardiopulmonary conditions or presence of any neck mass.
The primary outcome was to estimate the correlation of the ETT size used clinically on the Operating Table (OT) with the ETT size estimated by USG, age-based formula and height based formula. The secondary outcome was the number of ETT predicted by USG that was exchanged for a larger or smaller ETT on the basis of the air leak test.
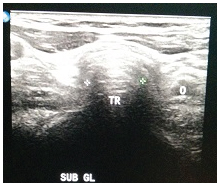
Consecutive eligible patients were evaluated for ETT size by USG, age-based and height-based formulae on the day before the planned surgery. The subglottic diameter was estimated with a high resolution B mode USG (Philips, IU-22, United States of America) with a linear probe (5-12 MHz and 7-15 MHz) positioned in the midline of the neck with the patient in sniffing position by an experienced radiologist. It began with location of true cords seen as paired hyper-echoic linear structures and then moved caudally to visualize the cricoid arch. The transverse air column diameter was measured at the cricoid cartilage and was considered as the tracheal diameter [Table/Fig-1]. The tracheal diameter corresponded to the outer diameter of the ETT and corresponding inner diameter of chosen ETT was used for comparison.
Transverse ultrasound view at the subglottic level showing the trachea (TR), oesophagus (O) and the measurement of the diameter of the trachea.
The height of the child was measured by a standard measuring tape (in cm) on a level surface against an even wall. The height based formula used was inner diameter of ETT (in mm.)= {height (in cm)/30} +2 [5].
The age based formulae used for uncuffed ETT: inner diameter (Modified Cole’s formula) = Age (in years)/4+ 4 and for cuffed ETT: inner diameter (Khine’s formula) = Age (in years)/4 + 3 [6].
On the day of surgery, all children were nil per oral according to standard guidelines. Premedication was done with injections midazolam 0.05 mg/kg, glycopyrrolate 0.01 mg/kg and fentanyl 1 mcg/kg on table before induction. All patients were pre-oxygenated with 100% oxygen for three minutes. General anaesthesia was induced with intravenous propofol 2 mg/kg and muscle relaxation achieved by intravenous succinylcholine 2 mg/kg. Patients were intubated under direct laryngoscopy by an experienced anaesthesiologist with polyvinyl chloride ETT (from the same manufacturer –Shailesh Surgical, Ahmedabad), cuffed or uncuffed ETT depending on the anaesthesiologist’s choice, and size that was pre-determined by USG. If cuffed ETT was chosen by anaesthesiologist the ETT size used was 1 mm external diameter less than that estimated by USG. If uncuffed ETT was chosen, then size used was the same as estimated by USG.
If there was resistance to ETT passage into trachea or if there was no audible leak when the lungs were inflated to a pressure of 20 cm of water which was measured on ventilator (Larsen & Toubro eV600 on anaesthesia machine Elite 615, Avarasarala Technologies Ltd. India) with head and neck in neutral position, the ETT was exchanged with one that was 0.5 mm smaller. In contrast, if on gradual reduction of pressure a leak occurred at an inflation pressure less than 10 cm of water, the ETT was exchanged for one that was 0.5 mm larger. ETT size was considered optimal when a tracheal leak was detected at an inflation pressure between 10-20 cm of water [1,7]. The final ETT that was intubated and found optimal on the OT is considered as clinically used ETT.
A comparison of ETT size estimated by USG, age-based formula, height-based formula and that used clinically were done.
Statistical Analysis
The data was analysed using International Business Machine SPSS version 20.0. Results were represented as mean±standard deviation. One-way (Analysis of Variance) ANOVA test was used for comparisons of age groups with different methods followed by post hoc Tukey’s test. Dependent t-test was used for comparisons of different methods and independent t-test was used for comparison of gender with different methods and p-value <0.05 was considered statistically significant.
Results
In our study, 36 male (48%) patients and 39 female (52%) patients were included. There were no dropouts in the study. Seven patients were ≤5 years, 28 patients were between >5 and 10 years of age and 40 patients were >10 years. The mean age in the study population was 10.19 years [Table/Fig-2]. Out of the 75 patients, cuffed ETT was used in 65 and uncuffed were used in 10 patients.
Summary of age, height and weight of patients involved in the study.
| Summary | Age (in years) | BMI (kg/m2) | Height (in cm) | Weight (in kg) |
|---|
| Minimum | 1.50 | 10.20 | 75.00 | 8.00 |
| Maximum | 14.00 | 25.00 | 168.00 | 55.00 |
| Mean | 10.19 | 16.16 | 136.47 | 31.20 |
| SD | 3.16 | 3.65 | 19.24 | 11.89 |
| SE | 0.37 | 0.43 | 2.27 | 1.40 |
BMI – Body Mass Index; cm–centimetres; kg–kilograms; kg/m2–kilogram per square metres; SD–Standard deviation; SE–Standard error
In our study, the mean ETT size for clinically used was 5.73±0.69, USG was 5.73±0.71, age based formula was 5.68±0.60 and height based formula was 6.12±0.54. Comparing the ETT size estimated by USG with the ETT used clinically did not show any significant difference (p=1.000) [Table/Fig-3]. The ETT estimated by USG predicted the optimal ETT in 67 patients (89.33%). Eight (10.6%) patients required change of ETT. Out of the eight patients, four required a cuffed 0.5 mm tube smaller, three required cuffed 0.5 mm tube larger and one required 0.5 mm uncuffed larger ETT.
Comparison of ETT size (in mm) estimated by USG, height based formula and age based formula with ETT size used clinically on the Operating table (OT) by dependent t-test.
| Techniques | Mean | SD | SE | t-value | p-value |
|---|
| ETT size estimated by USG (in mm) | 5.73 | 0.71 | 0.08 | 0.0000 | 1.0000 |
| ETT size used clinically on the OT table (in mm) | 5.73 | 0.69 | 0.08 |
| ETT size estimated by height based formula (in mm) | 6.12 | 0.54 | 0.06 | 3.8331 | 0.0002* |
| ETT size used clinically on the OT table (in mm) | 5.73 | 0.69 | 0.08 |
| ETT size derived from age based formula (in mm) | 5.68 | 0.60 | 0.07 | 0.5527 | 0.5813 |
| ETT size used clinically on the OT table (in mm) | 5.73 | 0.69 | 0.08 |
p-value <0.05 – significant; mm – millimeters, SD – Standard deviation; SE – standard error.
Comparing the ETT size estimated by age based formula with clinically used ETT size did not show any statistical difference (p= 0.5813) [Table/Fig-3]. Out of the 65 patients in whom cuffed ETT was used, the ETT size as determined by the age based formula correlated with the clinically used ETT size in 49 patients (75.38%), in 10 patients (15.38%) the age based formula estimated ETT size smaller than the clinically used ETT size and in six patients (9.23%) the age based formula determined ETT size larger than the clinically used ETT size. Out of the 10 patients in whom uncuffed ETT was used, the ETT size determined by the age based formula correlated with clinically used formula in two patients, determined smaller ETT size than used clinically in one patient and determined larger ETT size than used clinically in seven patients. Hence, our study showed that age based formula for cuffed tubes better predicted the ETT size, whereas, for uncuffed tube the formula predicted the ETT size larger than used clinically.
On comparing the ETT size estimated by height based formula with clinically used ETT size, we found a significant statistical difference (p=0.0002) [Table/Fig-3]. Out of the 65 patients in whom cuffed ETT was used, the ETT size as determined by the height based formula correlated with the clinically used ETT size in only 25 patients (38.46%); in 3 patients (4.61%) the height based formula estimated ETT size smaller than the clinically used ETT size and in 37 patients (56.92%) determined ETT size larger than the clinically used ETT size. Out of the 10 patients in whom uncuffed ETT was used, the ETT size determined by the height based formula correlated with clinically used ETT size in two patients, determined larger ETT size than clinically used ETT size in eight patients.
The ETT size estimated by USG and age based formula correlated with the clinically used ETT size, no statistical difference was noted on comparing these two methods (p=0.2196). But there was a highly significant statistical difference on comparing ETT size estimated by height based formula with age based formula (p<0.001) as well as on comparing ETT size estimated by height based formula and USG (p<0.001) [Table/Fig-4].
Comparison of ETT size (in mm) estimated by USG, height based formula and age based formula by dependent t-test.
| Techniques | Mean | SD | Mean Diff. | SD Diff. | Paired t | p-value |
|---|
| ETT size estimated by USG (in mm) | 5.73 | 0.71 | -0.39 | 0.44 | -7.6531 | <0.001* |
| ETT size estimated by height (in mm) based formula | 6.12 | 0.54 |
| ETT size estimated by USG (in mm) | 5.73 | 0.71 | 0.06 | 0.41 | 1.2380 | 0.2196 |
| ETT size derived from age based formula (in mm) | 5.68 | 0.60 |
| ETT size estimated by height based formula (in mm) | 6.12 | 0.54 | 0.45 | 0.27 | 14.4317 | <0.001* |
| ETT size derived from age based formula (in mm) | 5.68 | 0.60 |
p<0.05 – significant; mm – millimeters; SD – standard deviation.
Discussion
In paediatric anaesthesia, the selection of a properly sized ETT is critical for successful intubation. Various methods have been used to predict the appropriate size ETT. There are some studies conducted to determine the method for accurate prediction of ETT size especially in children.
Age-based formulae, such as those of modified Cole’s, Motoyoma and Khine’s have been used to estimate optimal ETT size more commonly [7]. Body length is the easiest parameter to be obtained under emergency conditions, when other parameters like age or weight are unavailable. The length-based formula internal diameter in mm = 2+ (body length in cm/30) has been shown to be accurate in predicting the appropriate ETT size according to Shih MH et al., in Chinese children [5]. Hence, we used it in our study for comparison in the Indian population. ETT size has been added to the Broselow tape to provide appropriate ETT selection based on height [8]. Only one study has compared the uncuffed ETT size and cuffed ETT size estimation by ultrasound in Japanese children [7]. Not many studies like ours have been done on Indian children with uncuffed and cuffed ETT size estimation by USG.
Gupta K and co-researchers [1] compared the size of ETT predetermined by USG and estimated by age based formula with clinically used ETT for intubation during general anaesthesia and found that there was high correlation between clinically used ETT and predetermined ETT by USG than predicted by age based formula. Their study also showed that direct measurement of the subglottic diameter by USG predicted the appropriate ETT size. Our study results were comparable with their findings. However, their study does not clearly indicate whether cuffed or uncuffed ETT was used.
Bae JY et al., in a study concluded that USG was a better means of estimation of ETT size in paediatric patients than the age based formula [2]. However, only uncuffed tubes were used in this study unlike our study. Also, USG was performed after induction of anaesthesia in this study [2]. But in our study, USG for ETT size estimation was done by an experienced radiologist and also an experienced anaesthesiologist did the assessment of appropriateness of the ETT size. All this was done to avoid operator variability.
Raphael PO et al., found that determination of cuffed ETT size by ultrasound was a good predictor of appropriate sized ETT in paediatric patients when compared with age based formula [9]. They performed USG guided estimation of tracheal diameter after induction of anaesthesia during mask ventilation of patient [9].
Our study also showed, that age based formula for cuffed tubes better predicted the ETT size, whereas, for uncuffed ETT the formula predicted the ETT size larger than used clinically. But Khine et al., found that modified Khine formula predicted 99% of cuffed ETT and that Cole’s formula predicted 77% of uncuffed tubes as appropriate in young children [6].
In our study, the height based formula was inaccurate in estimating the optimal ETT size, it overestimated the ETT size both for cuffed and uncuffed ETT sizes. This was contrary to Shih MH et al., who showed that the height based formula had high accuracy in estimating the optimal ETT size. This negative result could have been due to the difference in age group and ethnicity considered in the study [5]. Very few studies are available regarding the length based formula for ETT size estimation. In two studies, ETT size was estimated using the length based method using Broselow tape that is used in paediatric resuscitation [8,10]. But validation of Broselow tape for ETT size estimation is done for children from the United States [10].
USG does not require strict immobility, especially in infants and children, as opposed to MRI or computed tomography scan [3]; nevertheless ultrasonography depends on the skill of the operator, requires training and yet is relatively simple to learn.
Our study had some limitations. We performed USG in children pre-anaesthetically in non-sedated state as we did not have an ultrasound machine in the operating room. USG in crying and uncooperative children could lead to false subglottic tracheal diameter values. Airway USG if done with the child sedated via inhalational agents through a facemask would have probably yielded better patient cooperation and thereby more accurate results. Also, the method of assessing the optimal ETT size by air leak test is a subjective measure and is affected by many factors such as head position and degree of neuromuscular blockade. Though, we selected the ETT sizes from the same manufacturer, the ETT size used must actually be assessed on an individual basis. Also, the children chosen were randomly chosen and were not uniform in terms of height for weight which could have led to bias.
Our study thus shows the potential utility of USG for cuffed and uncuffed ETT size estimation. Hence, we recommend that USG can be used to assess the appropriate ETT size in children. As mentioned by some authors, ultrasound may be useful to evaluate patients with subglottic stenosis, a common complication in neonatal or paediatric anaesthesia [9].
Conclusion
USG is effective in estimating the appropriate sized ETT both for cuffed and uncuffed tubes. ETT size estimation by age based formula and by USG was comparable for cuffed ETT, whereas, the age based formula determined a large sized tube for uncuffed ETT. The height based formula for ETT size estimation was not effective for both cuffed and uncuffed ETT.
BMI – Body Mass Index; cm–centimetres; kg–kilograms; kg/m2–kilogram per square metres; SD–Standard deviation; SE–Standard error
*p-value <0.05 – significant; mm – millimeters, SD – Standard deviation; SE – standard error.
*p<0.05 – significant; mm – millimeters; SD – standard deviation.