Clinicopathological Study of Carcinoma of the Ampulla of Vater with Special Reference to MUC1, MUC2 and MUC5AC Expression
Maithili Mandar Kulkarni1, Siddhi Gaurish Sinai Khandeparkar2, Avinash R Joshi3, Aniket Kakade4, Lokesh Fegade5, Ketan Narkhede6
1 Associate Professor, Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
2 Associate Professor, Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
3 Professor, Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
4 Postgraduate Student, Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
5 Postgraduate Student, Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
6 Postgraduate Student, Department of Pathology, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Maithili Mandar Kulkarni, E-401, Samrajya, Shivthirthnagar, Paud Road, Kothrud, Pune-411038, Maharashtra, India.
E-mail: drmaithili@rediffmail.com
Introduction
The ampulla of Vater consists of papilla, common channel, distal common bile duct and the distal main pancreatic duct. Ampullary carcinomas arise from two different types of mucosa, reflecting their broad histomorphological spectrum. Adenocarcinomas originating in the ampulla of Vater are classified as having either ‘Intestinal’ or ‘Pancreatobiliary’ type of differentiation. Pancreatobiliary type has consistently shown a worse prognosis. Various types of mucins are distributed in normal tissues and gastrointestinal tumours. MUC1, MUC2 and MUC5AC are known to be the most important amongst all.
Aim
To study clinicopathological features of different types of carcinoma of ampulla with MUC1, MUC2 and MUC5AC expression.
Materials and Methods
We included 20 cases of ampullary adenocarcinoma in this study, diagnosed after radical surgery. The histopathological slides were reviewed and the tumours were classified into intestinal type, pancreatobilliary and other types. Representative block of tumours was subjected to immunohistochemical (IHC) study with MUC1, MUC2 and MUC5AC antibodies. Results were subsequently analysed.
Results
Pancreaticobiliary type of ampullary carcinoma cases predominated (50%) over intestinal type (25%). Carcinomas of “other types” included one case each of mucinous carcinoma, adenosquamous carcinoma and undifferentiated carcinoma and well differentiated neuroendocrine tumours. Pancreatobiliary type of carcinomas was associated with higher tumour stage and grade and lymph node metastasis. All the pancreatobiliary type expressed MUC1 and all intestinal type carcinomas expressed MUC2. MUC 5AC expression was seen predominantly in pancreatobiliary type of ampullary carcinomas.
Conclusion
Mucin markers are associated with two different subtypes of ampullary carcinomas which have different prognosis. Immunohistochemical study of mucin expression can define the different types of carcinomas of ampulla of Vater with better objective criteria.
Mucin markers, Periampullary carcinoma, Pancreatobiliary type
Introduction
The ampulla of Vater is composed of ampullary papilla, common channel, distal common bile duct and the distal main pancreatic duct. The ampullary papilla is lined by intestinal mucosa while the other parts are lined by pancreaticobiliary type of simple mucinous epithelium [1]. In consequence, ampullary carcinomas may arise from two different types of mucosa, which thus reflect the broad histomorphological spectrum of these tumours [2]. Kimura W et al., classified adenocarcinomas developing in the ampulla of Vater as having either ‘intestinal’ or ‘pancreatobiliary’ type of differentiation [3]. Pancreatobiliary type has consistently associated with worse prognosis [4].
All mucosal surfaces of the human body are covered by a thick viscous layer that protects it from external insults. The class of epithelial derived glycoproteins known as the mucins, forms a major component of this defensive mechanism. Mucins are expressed by a three letter code MUC followed by a number (e.g., MUC2) [5]. Mucins are classified as membrane bound or secreted depending on their structure and function. The membrane bound mucins are MUC1, MUC4, MUC13, MUC16, MUC17 and MUC21. Secreted or gel forming mucins include MUC2, MUC5AC, MUC5B, MUC6 and MUC7 which are encoded by genes located contiguously on chromosome 11. These genetic clustering signifies a clone functional association of the relevant proteins. Secreted mucins have unique number of tandem repeats, which could help in diagnosis, prognosis, and therapeutic guidence [6]. Mucins are widely distributed in normal tissues and gastrointestinal tumours. Of these different mucins, MUC1, MUC2, MUC5AC and MUC6 are the most important [7]. Abnormal mucin expression plays an important role in tumour occurrence and development [8].
The intestinal subtype and pancreatobiliary subtype do not show immunoexpression for MUC1 and MUC2 respectively [9]. Very few studies have been done to explore the expression of mucins in relation to histopathological subtypes of carcinoma of ampulla of Vater [9-11].
Some studies have used immunoexpression of apomucin MUC2 in classifying and assessing prognosis of ampullary carcinomas. Matsubayashi H et al., differentiated intestinal type carcinomas and pancreatobiliary type carcinomas by studying the expression of apomucin MUC2 [10]. Most intestinal type carcinomas were MUC2 positive and none of the pancreatobiliary type carcinomas expressed this apomucin. Kitamura H et al., found a positive correlation of MUC2 expression and survival rate and a negative correlation for MUC1 [11]. The gastric mucin MUC5AC positively correlated with pancreatobiliary type of carcinomas and negatively correlated with intestinal type carcinomas of ampullary region. We have studied clinicopathological features of different types of carcinoma of ampulla and their MUC1, MUC2 and MUC5AC immunoexpression.
Materials and Methods
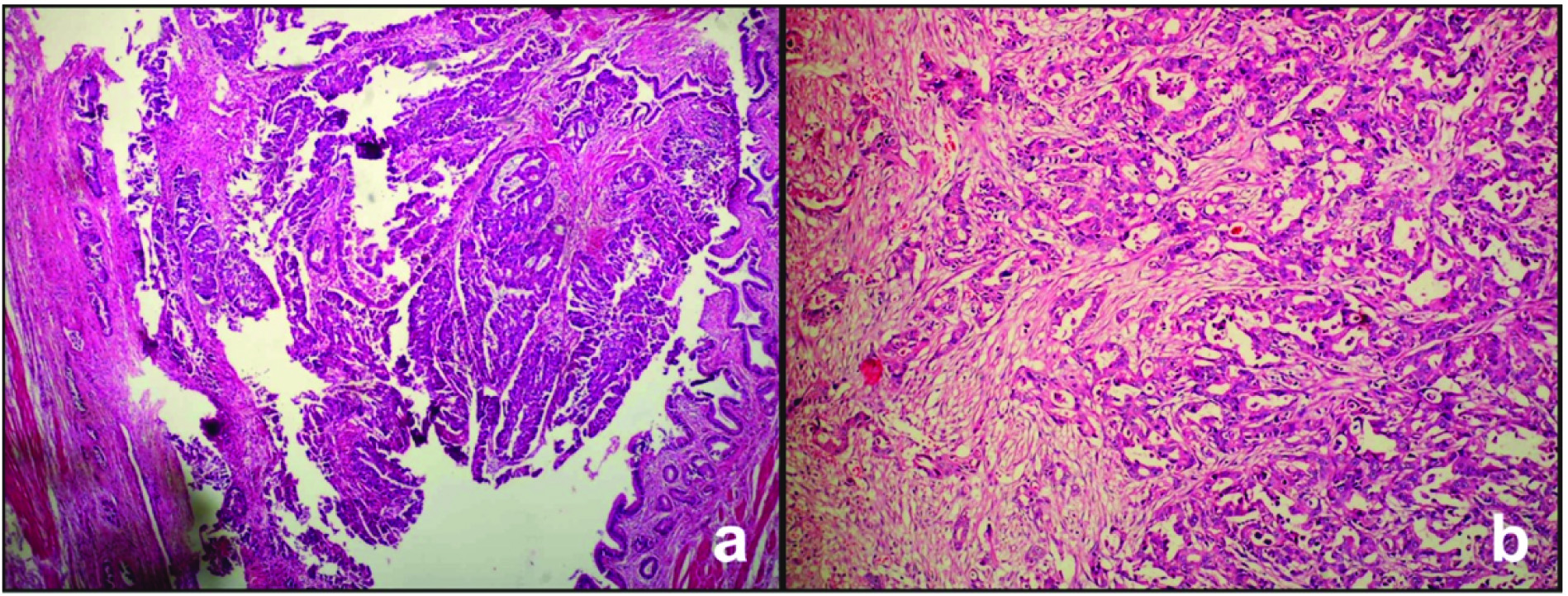
This was a cross-sectional descriptive study done in Smt Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India after approval from Institutional Ethics Committee. Our study enrolled 20 cases of patients who were histopathologically diagnosed with ampullary adenocarcinomas after surgery during a period of five years from January 2012 to December 2016. Patients informed consent was obtained. Medical records were reviewed from the files and clinical data was collected. The histopathological slides were reviewed and the tumour was classified histopathologically into intestinal type, pancreatobilliary and other types according to the criteria of Albores-Saavedra T et al., [12]. The intestinal type carcinoma [Table/Fig-1a] was composed of well formed tubules to elongated glands, complex cribriform areas and solid nests that was indistinguishable from colorectal carcinomas, whereas, the pancreato biliary type carcinomas [Table/Fig-1b] mostly consisted of simple or branching glands and solid nests of cells surrounded by a strikingly desmoplastic stroma. Representative block of tumours was subjected to IHC. IHC study was done with antibodies which included MUC1 (Clone Ma695; Novocastra), MUC2 (Clone Ccp58; Novocastra) and MUC5AC (Clone CLH2; Novocastra). The staining intensity of each IHC reaction were scored semiquantitatively: no staining reaction=0, <10% positively stained tumour cells =1, 10-50%=2, > 50-80%=3 and >80%=4. Scores 0 and 1 were regarded as negative and scores 2-4 were regarded as positive.
a) Photomicrograph showing intestinal subtype of ampullary carcinoma (H&E, 4X); b) Photomicrograph showing pancreatobiliary subtype of ampullary carcinoma (H & E, 10X).
Statistical Analysis
Data was subjected to statistical analysis using arithmetic mean and percentage.
Results
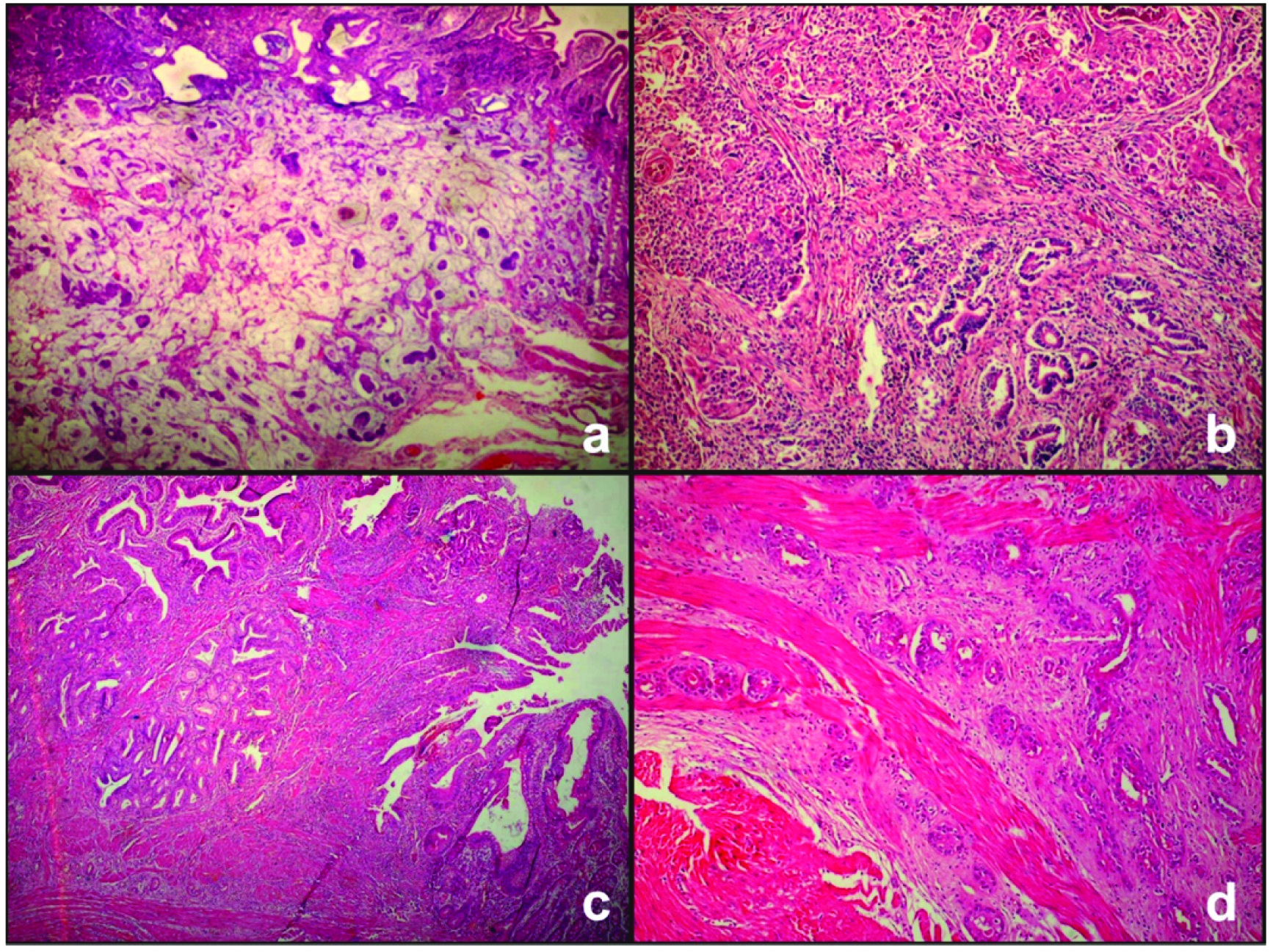
Total 20 cases were studied. Age range was from 44 to 74 year years. Mean age was 57 years. There were 12 male and eight female patients. Histomorphologically, pancreaticobiliary type of ampullary carcinoma cases predominated (10/20, 50%) over intestinal type (5/20, 25%). Carcinomas of “other types” included mucinous carcinoma [Table/Fig-2a], adenosquamous carcinoma [Table/Fig-2b], and undifferentiated carcinoma and well differentiated neuroendocrine tumours. A case with mixed pattern had features of both intestinal [Table/Fig-2c] and pancreatobiliary carcinoma [Table/Fig-2d].
a) Photomicrograph showing mucinous subtype of ampullary carcinoma (H&E, 40X); b) Photomicrograph showing adenosquamous subtype of ampullary carcinoma (H&E, 10X); c) Photomicrograph showing intestinal features of mixed type ampullary carcinoma (H&E, 10X); d) Photomicrograph showing pancreatobiliary features of mixed type ampullary carcinoma (H&E, 10X).
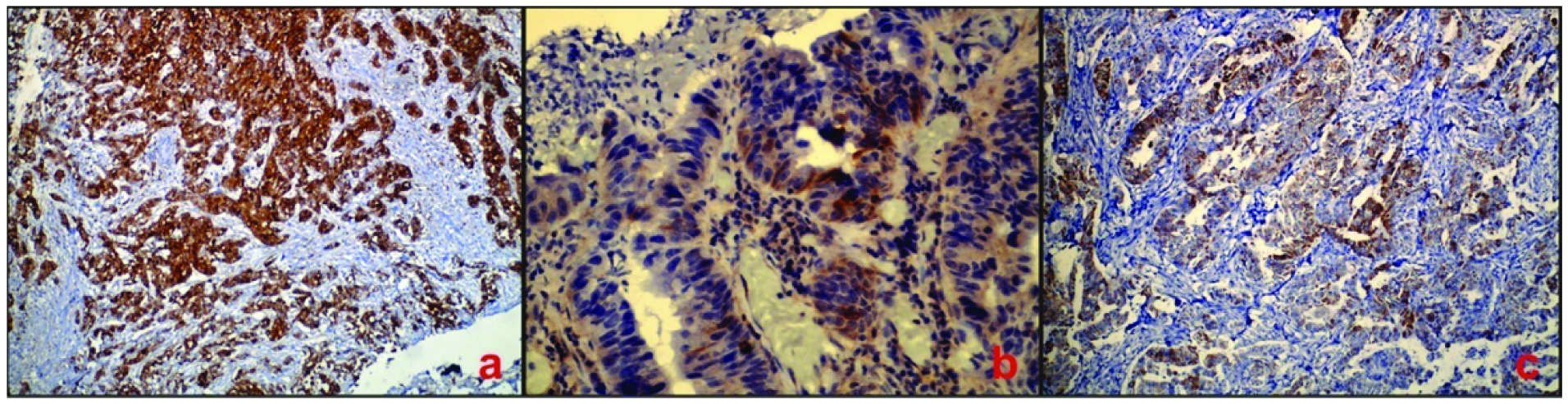
The photomicrographs showing MUC1 expression in pancreatobiliary subtype, MUC2 expression in intestinal subtype and MUC5AC in pancreatobiliary subtype is shown in [Table/Fig-3a-c] respectively.
a) Photomicrograph showing MUC1 immunoreactivity (100X) in pancreatobiliary subtype; b) Photomicrograph showing MUC2 immunoreactivity (400X) in intestinal subtype; c) Photomicrograph showing MUC5AC immunoreactivity (100X) in pancreatobiliary subtype.
Comparison of different clinical and immunohistopathological features of two main subtypes of carcinoma of ampulla of Vater is summarized in [Table/Fig-4,5].
Comparison of pancreatobiliary type and intestinal type of carcinoma of ampulla of vater.
| Parameters | Pancreaticobiliary type (n-10) | intestinal type (n-5) |
|---|
| Mean age at diagnosis (years) | 57.6 | 50.83 |
| Male: Female | 1:1 | 4:1 |
| TNM staging | Seven cases were T3, three cases were T2. two cases showed LN metastasis | All cases were T2, No cases showed LN metastasis |
| MUC 1 immunoreactivity | 10 | 0 |
| MUC 2 | 0 | 5 |
| MUC 5AC | 5 | 0 |
Expression of MUC1 in pancreatobiliary carcinoma of ampulla of vater.
| Grade of tumour (N) | MuC 1 expression |
|---|
| 0+ | 1 + | 2+ | 3+ | 4+ |
|---|
| WDT(2) | 0 | 0 | 2 | 0 | 0 |
| MDT(3) | 0 | 0 | 2 | 1 | 0 |
| PDT(5) | 0 | 0 | 1 | 2 | 2 |
WDT=Well Differentiated Tumour, MDT= Moderately Differentiated Tumour, PDT=Poorly Differentiated Tumour
MUC1 expression in pancreatobiliary carcinoma of ampulla of Vater is shown in [Table/Fig-5]. Mucin expression in other types of ampullary carcinomas is shown in [Table/Fig-6].
Mucin expression in other types of ampullary carcinomas (n-5).
| Tumour type | Stage | muc1 | muc2 | muc5ac |
|---|
| Adenosqumous carcinoma | T4N0Mx | Strong Positive (4+) | N | N |
| Neuroendocrine tumour | T2N0Mx | N | N | N |
| Mucinous adenocarcinoma | TNM | 4+ | 4+ | 4+ |
| Mixed pattern | T3N0Mx | 3+ | 1+ | 2+ |
| Undifferentiated carcinoma | T2N1Mx | N | 2+ | 1 + |
Discussion
Carcinomas of the ampulla of Vater are uncommon, but they occur more frequently than carcinomas of the small intestine outside the periampullary region [13]. The peak age incidence of sporadic carcinomas is in seventh and eighth decades of life [12]. Males appear to be more affected than females with the ratio being 1.48 to 1.12 as documented in literature [12]. In our study, age ranged from 44 to 74 years with a mean age of 57 years. There were 12 males and 8 females with the ratio of 1.5:1.
Carcinomas of ampulla of Vater usually present early with smaller tumour size and obstructive jaundice. They are usually circumscribed nodules measuring not more than 2 cm to 3 cm in diameter. They may be found within the wall of the duodenum or project into the lumen as a nodule [14]. In our study, majority of the patients presented with obstructive jaundice and pain in abdomen. The tumour size ranged from 0.5 cm to 3 cm, with mean tumour size of 1.5 cm. The distribution of various histomorphological types was in correlation with a study done by Fischer HP and Zhou H [2]. Frequency of the main histopathological types of carcinomas of ampulla of vater in different studies is shown in [Table/Fig-7].
Frequency of the main histopathological types of carcinomas of ampulla of vater in different studies.
| Author/study | Number of cases | Intestinal type (%) | Pancreat-obiliary type (%) | Other types (%) |
|---|
| Kimura W et al., [3] | 51 | 25 | 75 | - |
| Matsubayashi H et al., [10] | 52 | 58 | 42 | - |
| Fischer HP and Zhou H [2] | 55 | 23 | 44 | 24 |
| WHO classification [14] | | Unusual | | |
| Our study | 20 | 25% | 50% | 25% |
The expression pattern of MUC1 in tumours of the ampulla of Vater appears to have predictive value based on the results of the recent studies [15,16]. In particular, MUC1 positivity was associated with unfavourable behaviour of the tumour such as lymph node metastasis, vascular infiltration, infiltration of pancreas and duodenum, advanced TNM staging and worse prognosis [16]. The utility of MUC1 as a biomarker in pancreatobiliary neoplasia and its prognostic significance has exceeded that of conventional pathologic features [17]. MUC1 and mesothelin are among the most promising targets for cancer vaccine development as per the study done by National cancer institute [18]. In our study, MUC1 immunoreactivity was observed in all 10 cases of pancreatobiliary type of carcinoma of ampulla and was absent in all five cases of intestinal subtype. The immunoreactivity increased with increase in grade of the tumour. It was 40%, 61%, 64% in well differentiated, moderately differentiated and poorly differentiated pancreatobiliary carcinomas respectively. Pancreatobiliary carcinomas showed higher tumour stage and increased incidence of lymph node metastasis as compared with intestinal subtype. Thus, MUC1 immunoreactivity correlated with higher histopathological grade, higher tumour stage and lymph node metastasis.
In a study by Tao Wang et al., the expression of MUC1 was observed more frequently than the other mucins studied and was associated with a higher tumour grade of [9]. Expression of MUC1 may affect patient prognosis by inhibiting the formation of the E cadherin and beta–catenin complex, which consequently would decrease intercellular adhesion and promote the invasion and metastasis of tumours [1]. In another study, MUC1 was found to be 100% sensitive but 0% specific in the diagnosis of pancreatobiliary subtype [19].
Pancreatobiliary type adenocarcinomas predominantly express keratin 7 and lack the intestinal apomucin MUC2. This is in accordance with normal pancreatobiliary epithelium. Intestinal type adenocarcinomas mostly contain apomucin MUC2 similar to the characteristics of the intestinal epithelium [13]. In a study done on 105 adenocarcinomas of the ampulla of Vater, intestinal immunophenotype was characterized by MUC2 and CDX2 expression, while pancreatobiliary immunophenotype was characterized by MUC2 and CDX2 negativity [20]. MUC2 showed low sensitivity (39.5%) and high specificity (96.2%) for intestinal subtype [19]. MUC2 immunoreactivity in our study was noted in all intestinal subtypes, while it was absent in all pancreatobiliary subtypes. The immunoreactivity of MUC2 was of less intensity as compared to MUC1.
In other subtypes of carcinomas of ampulla of Vater, adenosquamous carcinoma had highest tumour stage (T4). It showed MUC1 immunoreactivity. Undifferentiated carcinoma showed MUC2 immunoreactivity and thus, was reclassified as intestinal subtype after immunonohistochemical studies. One case of mixed pattern showed immunoreactivity for both MUC1 (3+) and MUC2 (1+). This tumour was reclassified as pancreatobiliary because of strong MUC1 immunoreactivity.
Expression of MUC5AC in neoplasias of the ampulla of vater is associated with the histological subtype. MUC5AC immunoreactivity is associated with the pancreatobiliary phenotype and participates in subsequent stages of carcinoma extension such as invasion and metastasis [5]. It was observed that intestinal type carcinomas show weak expression. Expression of MUC5AC correlates with invasiveness of carcinoma. In our study, MUC5AC immunoreactivity was observed in four cases of pancreatobiliary subtype and was absent in all intestinal subtype. Also, it was present in a case of mixed pattern which was reclassified as pancreatobiliary after IHC study. Out of four cases of pancreatobiliary carcinomas with lymph node metastasis in the present study, two of them showed MUC5AC immunoreactivity. One case of pancreatobiliary carcinoma showed lymphovascular invasion. Only one case of undifferentiated type carcinoma which was reclassified as intestinal subtype showed MUC5AC immunoreactivity and lymph node metastasis. This tumour was of higher grade histologically.
Limitation
As sample size is small, more number of studies with large sample size is recommended for validation of the results.
Conclusion
The different types of carcinomas of ampulla of Vater can be characterized more objectively by studying the mucin expression pattern immunohistochemically. The studies found in literature are very few and show variable results. In our study, pancreatobiliary carcinomas showed higher tumour stage and increased incidence of lymph node metastasis as compared with intestinal subtype. MUC1 expression was associated with pancreatobiliary carcinoma and MUC2 was seen in intestinal subtype of carcinoma of ampulla of Vater. Thus, MUC1 immunoreactivity correlated with higher histopathological grade, higher tumour stage and lymph node metastasis. MUC5AC immunoreactivity was associated with lymph node metastasis and higher tumour grade. Thus, IHC study of mucin expression pattern may help in prognostication and hence, in management of patients of carcinoma ampulla of Vater. However, it should be studied extensively.
WDT=Well Differentiated Tumour, MDT= Moderately Differentiated Tumour, PDT=Poorly Differentiated Tumour
[1]. Zhou H, Schaefer N, Wolff M, Fischer HP, Carcinoma of the ampulla of Vater: comparative histologic/immunohistochemical classification and follow-upAm J Surg Pathol 2004 28:875-82. [Google Scholar]
[2]. Fischer HP, Zhou H, Pathogenesis and histomorphology of ampullary carcinomas and their precursor lesions. Review and individual findingsPathologe 2003 24:196-203. [Google Scholar]
[3]. Kimura W, Futakawa N, Yamagata S, Wada Y, Kuroda A, Muto T, Different clinicopathologic findings in two histologic types of carcinoma of papilla of VaterJpn J Cancer Res 1994 85:161-66. [Google Scholar]
[4]. Westgaard A, Tafjord S, Farstad IN, Cvancarova M, Eide TJ, Mathisen O, Pancreatobiliary versus intestinal histologic type of differentiation is an independent prognostic factor in resected periampullary adenocarcinomaBMC Cancer 2008 8:170 [Google Scholar]
[5]. Moschovis D, Bamias G, Delladetsima I, Mucins in neoplasms of pancreas, ampulla of Vater and biliary systemWorld J Gastrointest Oncol 2016 8:725-34. [Google Scholar]
[6]. Singh AP, Chaturvedi P, Batra SK, Emerging roles of MUC4 in cancer: a novel target for diagnosis and therapyCancer Res 2007 67:433-36. [Google Scholar]
[7]. Lee MJ, Lee HS, Kim WH, Choi Y, Yang M, Expression of mucins and cytokeratins in primary carcinomas of the digestive systemMod Pathol 2003 16:403-10. [Google Scholar]
[8]. Hollingsworth MA, Swanson BJ, Mucins in cancer: protection and control of the cell surfaceNat Rev Cancer 2004 4:45-60. [Google Scholar]
[9]. Wang T, Liang YM, Hu P, Cheng YF, Mucins differently expressed in various ampullary adenocarcinomasDiagn Pathol 2011 6:102 [Google Scholar]
[10]. Matsubayashi H, Watanabe H, Yamaguchi T, Ajioka Y, Nishikura K, Kijima H, Differences in mucus and K-ras mutation in relation to phenotypes of tumours of the papilla of vaterCancer 1999 86:596-607. [Google Scholar]
[11]. Kitamura H, Yonezawa S, Tanaka S, Kim YS, Sato E, Expression of mucin carbohydrates and core proteins in carcinomas of the ampulla of Vater: their relationship to prognosisJpn J Cancer Res 1996 87:631-40. [Google Scholar]
[12]. Albores-Saavedra J, Henson DE, Klimstra DS, Rosai J, Sobin LH, Tumours of the gallbladder, extrahepatic bile ducts, and ampulla of VaterAtlas of tumour pathology 2000 Third seriesFascicle 27. Washington DCArmed Forces Institute of Pathology:259-316. [Google Scholar]
[13]. Fischer HP, Zhou H, Pathogenesis of carcinoma of the papilla of VaterJ Hepatobiliary Pancreat Surg 2004 11:301-09. [Google Scholar]
[14]. Wright NH, Pennazio M, Howe JR, Sobin LH, Rossini FP, Carr NJ, Hamilton SR, Aaltonen LA, Carcinoma of the small intestine. WHO classification of TumoursPathologyand Genetics of the Digestive System 2000 LyonIARC Press:71-74. [Google Scholar]
[15]. Westgaard A, Schjølberg AR, Cvancarova M, Eide TJ, Clausen OP, Gladhaug IP, Differentiation markers in pancreatic head adenocarcinomas: MUC1 and MUC4 expression indicates poor prognosis in pancreatobiliary differentiated tumoursHistopathology 2009 54:337-47. [Google Scholar]
[16]. Saitou M, Goto M, Horinouchi M, Tamada S, Nagata K, Hamada T, MUC4 expression is a novel prognostic factor in patients with invasive ductal carcinoma of the pancreasJ Clin Pathol 2005 58(8):845-52. [Google Scholar]
[17]. Harsha HC, Kandasamy K, Ranganathan P, Rani S, Ramabadran S, Gollapudi S, A compendium of potential biomarkers of pancreatic cancerPLoS Med 2009 6:e1000046 [Google Scholar]
[18]. Cheever MA, Allison JP, Ferris AS, Finn OJ, Hastings BM, Hecht TT, The prioritization of cancerantigens: a national cancer institute pilot project for the acceleration of translational researchClin Cancer Res 2009 15(17):5323-37. [Google Scholar]
[19]. Kumari N, Prabha K, Singh RK, Baitha DK, Krishnani N, Intestinal and pancreatobiliary differentiation in periampullary carcinoma: the role of immunohistochemistryHum Pathol 2013 44:2213-19. [Google Scholar]
[20]. Ang DC, Shia J, Tang LH, Katabi N, Klimstra DS, The utility of immunohistochemistry in subtyping adenocarcinoma of the ampulla of vaterAm J Surg Pathol 2014 38:1371-79. [Google Scholar]