Autopsy as a word means self-study of dead body. It is an important way to find out the condition of internal organs, to evaluate disease or injury that could explain the cause and manner of person’s death [1]. Examination of all the three cavities of body including cranium, thorax and abdomen are an essential part of autopsies. In thorax, lungs examination is the most important part of both the medicolegal as well as clinical autopsies. The medicolegal autopsy is carried out by forensic expert to help the law by establishing identity, cause of death, time of death, and ante-mortem or post-mortem nature of crime. The clinical autopsy or pathological autopsy is usually performed by pathologist to establish the cause of death and to study the disease process which led to death [2].
Autopsy is often followed by histopathological examination of tissues from various organs. In cases where tissue is not properly preserved in fixative or the tissue is a non-representative sample, final histopathological report is often not possible. However, despite pitfalls like delays in carrying out autopsies, improper sampling, improper preservation and transport, microscopic examination of tissues is still considered a very useful method to study the disease process in situ, thus enriching the medical knowledge [3]. Studies have reported a significant major and minor discrepancies between clinical and autopsy diagnoses [4].
Histopathological examination of autopsy samples of the lungs analysed has been presented in this study. This study describes the prevalence and pattern of lung diseases in medicolegal autopsies, confirmed by histopathological examination.
Materials and Methods
This retrospective study was carried out in the Department of Pathology, Dr BSA Hospital, New Delhi, over a period of one and half years from June 2013 to December 2014. All consecutive cases that underwent medicolegal autopsy during that period, irrespective of age and sex, were included in this study. Ethical clearance was not taken because of medicolegal nature of cases. A total of 86 cases of lung autopsy samples were received in the department. All these autopsies were performed by a forensic expert. Tissue bits from lungs were preserved in 10% formalin. These were then sent to our department along with history, clinical details and gross findings. We took 4 mm to 5 mm pieces from lung tissues in cassettes and after routine processing, paraffin embedding, blocks were prepared. All the histological sections were stained with Haematoxylin & Eosin stain and mounted. Ziehl-Neelson stain and Periodic Acid- Schiff (PAS) stain were also done, wherever required. They were then examined microscopically and findings were recorded. The findings could not be correlated with the gross findings as forensic expert did not provide gross details and sent only small portions of lung tissue.
Results
A total of 86 cases were received during the period of study along with relevant clinical details and autopsy findings. Histopathological examination was carried out in each case. Among these 86 cases, in 4 cases (4.8%) the tissue was autolysed and in another 26 cases (30.1%) histopathology was unremarkable. Significant microscopic findings were found in 56 cases (65.1%). The age ranged from 2 days to 71 years. There were 16.3% cases below 15 years of age, inclusive of three cases of normal and 11 abnormal lung tissues. The majority of the lung samples belonged to autopsies carried out in adults between 16 to 60 years age group. Among these 64 cases (74.4%), 34 were in age group of 16 to 30 years. There were only 4 cases of more than 60 years age group where autopsies were carried out. Among them two each had normal and abnormal histopathological findings [Table/Fig-1].
Status of lung tissue on histopathology (n=86).
| Parameters | New born – 15 yrs | 16-30 yrs | 31-45 yrs | 46-60 yrs | >60 yrs | Total (%) |
|---|
| Normal lung | 03 | 11 | 07 | 03 | 02 | 26 (30.1) |
| Diseased lung | 11 | 23 | 16 | 04 | 02 | 56 (65.1) |
| Lysed lung tissue | -- | 03 | 01 | -- | -- | 04 (4.8) |
| Total cases | 14 | 37 | 24 | 07 | 04 | 86 |
Wide varieties of microscopic findings were seen in lungs which included oedema and congestion, inflammation (acute, granulomatous and fungal), changes in interstitium, emphysema and Acute Respiratory Distress Syndrome (ARDS). There was one case each of HMD, MAS and ARDS in the series [Table/Fig-2].
Spectrum of histological findings (n=56).
| Lesions | New born – 15 yrs (M/F) | 16-30 yrs (M/F) | 31-45 yrs (M/F) | 46-60 yrs (M/F) | >60 yrs (M/F) | Total (M/F) |
|---|
| Congestion and oedema | 03 (1/2) | 12 (7/5) | 09 (7/2) | -- | -- | 24 (15/9) |
| Changes in interstitium | 02 (1/1) | 04 (4/0) | 02 (2/0) | 2 (2/0) | -- | 10 (9/1) |
| Inflammationi)Pneumoniaii)Granulomaiii)Fungal | 02 (2/0)---- | 02 (2/0)05 (2/3)-- | 01 (1/0)02 (1/1)01 (1/0) | --01 (1/0)-- | ------ | 05 (5/0)08 (4/4)01 (1/0) |
| Emphysematous changes | 02 (2/0) | -- | -- | 01 (1/0) | 02 (2/0) | 05 (5/0) |
| Acute respiratory distress syndrome | -- | -- | 01 (1/0) | -- | -- | 01 (1/0) |
| Hyaline membrane disease | 01 (1/0) | -- | -- | -- | -- | 01 (1/0) |
| Meconium aspiration syndrome | 01 (0/1) | -- | -- | -- | -- | 01 (0/1) |
| Total | 11 (7/4) | 23 (15/8) | 16 (13/3) | 04 (4/0) | 02 (2/0) | 56 (41/15) |
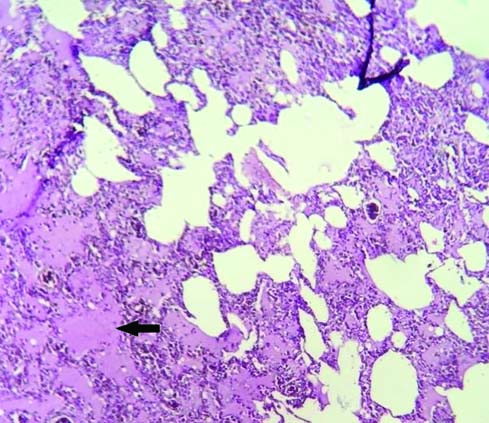
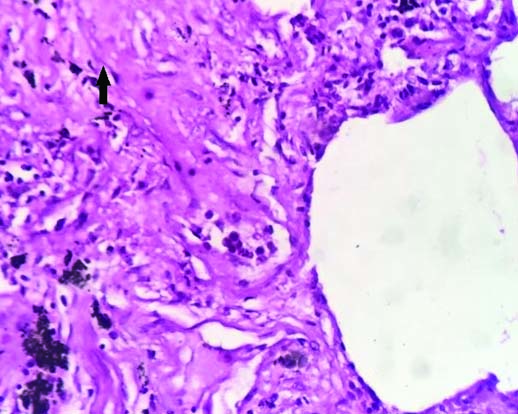
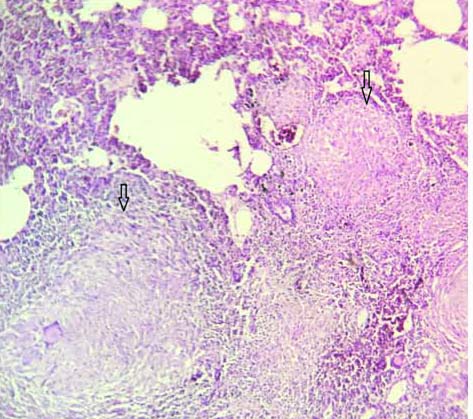
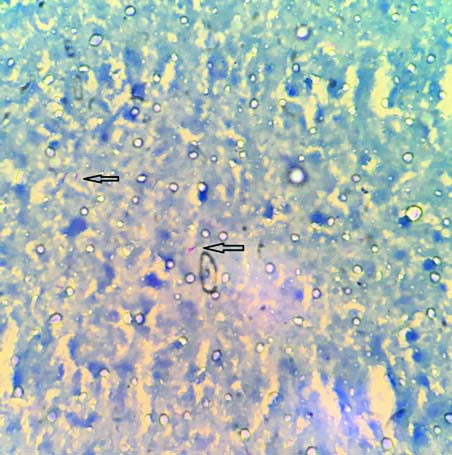
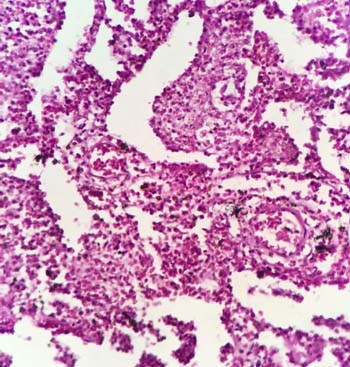
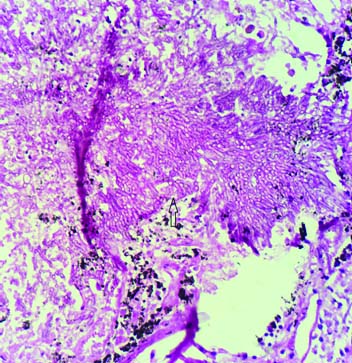
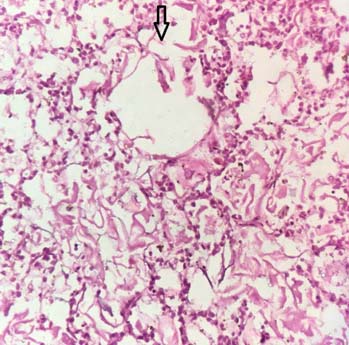
Among the pathologies detected in 56 lung autopsies, there were 41 (73.21%) males and 15 (26.79%) females. Congestion and oedema [Table/Fig-3] were the commonest pathology seen in 15 males and nine females. These cases showed congested blood vessels and intra-alveolar haemorrhages, alveoli distended with protein rich fluid. The second commonest pathology was changes in interstitium, seen in nine males and one female. There was broadening of interalveolar septae due to mononuclear infiltrate, interstitial fibrosis and increased alveolar macrophages in these cases [Table/Fig-4]. Granulomatous inflammation [Table/Fig-5] was also seen in four males and four females. Out of these eight cases three cases were ZN stain positive showing presence of Acid Fast Bacilli (AFB) [Table/Fig-6]. Caseous necrosis was present in all these eight cases and these were diagnosed to be suffering from pulmonary tuberculosis. Acute pneumonia was seen in five cases characterized by vascular engorgement, intra-alveolar fluid and neutrophilic infiltrate [Table/Fig-7]. All these patients were males with two of them under 15 years of age. Emphysematous changes were seen in five cases which showed large alveoli separated by thin septa and focal fibrosis, few showing ruptured alveoli. There was one case of young adult male having acute respiratory distress syndrome which showed congestion, intra-alveolar oedema, inflammation, fibrin deposition. Few alveoli were lined by waxy hyaline membrane. The series also had one case of young adult male having fungal colonies surrounded by necrosis and abscess formation. The colonies were of aseptate broad hyphae branching at right angles [Table/Fig-8]. Few hyphae were seen sticking to lumen of bronchioles. Possibility of mucormycosis was suggested on histopathological examination in this case.
Oedema: pinkish fluid (arrow) present in alveolar spaces and septae (H&E 10X).
Changes in interstitum-interstitial fibrosis (arrow) in the interalveolar septae (H&E 40X).
Coalescing epithelioid cell granuloma (arrow) (H&E 10X).
Microphotograph showing presence of acid fast bacilli (arrow) (ZN stain 100X).
Pneumonia- neutrophylic exudate into the alveoli (H&E 10X).
Fungal colonies of non-septate fungal hyphae branching at right angle (H&E 10X).
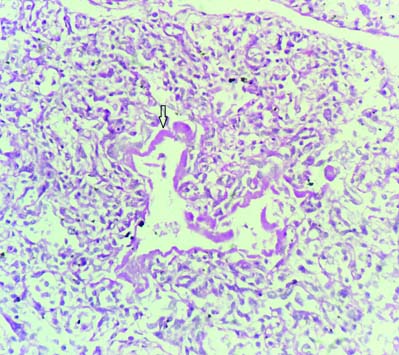
One case of hyaline membrane disease was seen in which section showed alveoli lined by eosinophilic hyaline membrane [Table/Fig-9]. One case was of meconium aspiration syndrome which showed few squames within the alveoli [Table/Fig-10].
Hyaline membrane disease: Alveolar wall lined by dense proteinaceous hyaline membrane (H&E 40X).
Meconium aspiration syndrome- squames (arrow) present in the alveolar spaces (H&E 40X).
Discussion
Medicolegal autopsies are a mandatory legal requirement in unnatural deaths to assist the law. To perform a medicolegal autopsy, consent from relatives of the deceased is not required [1]. The facilities for medicolegal autopsies are available across all districts of our country [3]. The autopsy, if combined with relevant details and histopathological examination, is of great value in establishing reasons which led to death [1].
Kandy NC et al., quoted that even in the era of high-tech medicine the autopsy remains an important tool for quality assessment of clinical diagnoses [5]. As far as lungs are concerned, these were normal in only 9.80% of the total number of autopsies in their series. In our retrospective study of 86 cases, the autopsy samples of lungs were autolysed in four cases and those cases were excluded from the study. Among the rest 82 cases, in 26 cases (31.9%) histopathological findings were unremarkable. Eighteen among these 26 cases were adults between 16 to 45 years age group, signifying the healthy status of lungs in the adults. 56 cases (68.1%) had significant microscopic finding.
Bal MS et al., in their series of 150 cases had 19 autolysed sample and 11 cases with normal lung tissue [6]. Unlike their series we had much higher percentage of cases with no remarkable pathology. The very low number of autolysed samples in our series was probably due to availability of autopsy facilities in the hospital. There was male predominance in our series with males and females accounting for 59 (72%) and 23(28%) respectively. Similar sex distribution has also been observed by many other authors [7,8].
In our study, congestion and oedema was the commonest finding and was seen in 24 cases. This was 42.86% of the total lung cases with pathological changes. Similar observations were also observed by many authors in their series [8,9]. This could be a death related change or secondary involvement of lungs in all forms of terminal events due to cardiovascular causes. The second commonest finding was changes in interstitium in our series. It was seen in 10 cases (17.9%). Such changes could be due to pollution, smoking or any restrictive lung disease leading to fibrosis.
We had 5 cases (8.75%) of emphysema in our series of 56 cases. Among those five males, two were children and rest three were in age group of more than 46 years. All of these cases had urban background. The two children were known cases of bronchial asthma. Selvam V et al., reported 54 cases (50%) of emphysematous changes in the lungs in their series of 108 cases [8]. Their study had 61.1% and 38.9% cases with urban and rural background respectively. There were a very high percentage of labourers and farmers who had risk to toxic exposure (45.3%).
In this study, we came across 5 cases (8.7%) of acute pneumonia. Two cases each were seen in children and young adults and one in middle aged male. Kandy NC et al., found 26.3% cases of pneumonia on histopathology of lung samples in their series of 51 cases [5]. Their study emphasized discordance in the diagnosis made on gross examination of lungs and final histopathological diagnosis at autopsy, particularly in cases of bronchopneumonia. Hunt CR et al., also had similar observations of discordance in the final diagnosis. However, we did not examine this aspect of findings in our study [10].
Granulomatous inflammation was seen in 8 cases (14.3%) in present series. Caseous necrosis and epithelioid cell granulomas were seen in all these cases, however only three were positive for AFB on ZN staining. Thus autopsy confirmed three cases having definitive diagnosis of pulmonary tuberculosis and another five with high probability of having pulmonary tuberculosis during their life time. Similar results were seen in studies conducted by Garg M, et al., [11]. In their study granulomatous inflammation was an incidental finding in majority of the cases (6 out of 8) not correlating with post mortem findings or history. This could have been due to ignorance on the part of doctors not investigating the possibility of tuberculosis despite suspicious symptomatology. Kandy NC et al., found tuberculous changes in lungs confirmed by histopathology in 15.78% cases in their series of 51 cases.
One case in our series where fungal colonies were seen was an incidental finding. Aseptate broad hyphae branching at right angles were present in that case. A study conducted by Uppin MS et al., also found broad non septate hyphal form in lung in only one case which they classified as zygomycetes species [12].
Only one autopsy sample showed features of ARDS in our series of 56 cases (1.8%). Retrospective study conducted by Sachdev S et al.,125 lung autopsy cases over a period of three years, also observed low prevalence of acute respiratory distress syndrome (3.15%) [13]. Other authors also reported low incidence rate of ARDS in lung autopsies [14].
One case each of hyaline membrane disease and meconium aspiration syndrome was seen in our series. The hyaline membrane disease was seen in a preterm baby having gestational age six months and 18 days. Meconium aspiration syndrome was seen in a term infant of gestational age 40 weeks. Thomas S et al., in their prospective study on spectrum of respiratory distress in 1400 consecutive new-borns in North Indian population found that 116 cases developed respiratory distress [15]. Among these 116 cases, there were 10 cases of hyaline membrane disease and 14 cases of meconium aspiration syndrome. However, the post-mortem correlation could not be done as in many cases autopsy was refused. The study established that HMD was a disease of preterm (all 10 cases were preterm) and MAS was seen mostly in term babies (11 out of 14 cases were term babies).
Limitation
The short coming of the study was non receipt of whole organ or representative sample at the time of autopsy, which if overcome will set much higher standard of autopsy reporting and would be a more useful tool in understanding cause of death.
Conclusion
Facilities of histopathological examinations of the autopsied tissues are available only in small number of institutions which often leads to delay and damages to the autopsy tissue samples. Also, factors like inadequate sampling, improper fixation and failure to send representative sections leads to contradiction between autopsy finding and histopathological examination. The histopathological examination helps in establishing the final cause of death. In addition to that it also provides additional information about prevalence of nosocomial infections in critical areas of hospital, identifying the hereditary conditions that would require genetic counselling, prevalence of chronic infective diseases like tuberculosis and diseases related to pollution and work place environment, as was found in our series.
This study highlights various lesions in lungs which were either incidental or direct cause of death. For instance the case of hyaline membrane disease in the preterm baby, autopsy was done for medical negligence. The histopathological diagnosis on autopsy correlated well with clinical cause of death in our series.