Antenatal corticosteroids are recommended in pregnant mothers between 24-34 weeks gestation deemed at risk for preterm delivery for decreasing the incidence of RDS in neonates [1,2]. The benefits of betamethasone administration between 24 hours and seven days on preterm delivery have been established [3,4].
However, there are very less studies on effects of a single course corticosteroids when delivery occurs within 24 hours or seven days after injection [5]. The aim of this study was to observe the effect of single dose betamethasone administration on haematological parameters in mothers and incidence of RDS in neonates born to them.
Materials and Methods
This was a prospective study of mothers at risk of preterm delivery and their newborns from August 2013 to July 2014. Pregnant mothers in age group of 18-45 years visiting the obstetrics and gynaecology (OBS and GYN) department of a Pramukhswami Medical College and Teaching Hospital, Karamsad, Gujarat, India at less than 37 completed weeks of gestation diagnosed with preterm labour were included in the study. They were administered single dose of intramuscular injection of 24 mg betamethasone as per treating obstetrician’s decision. Written informed consent was obtained from all mothers who agreed to participate in the study. Ethical approval was taken from Institutional Human Research Ethics Committee prior to undertaking the study.
Mothers with diabetes mellitus, those on prolonged steroid therapy and maternal medical illness (e.g., serious systemic infections, renal disease, systemic lupus erythematosus, trauma etc.,) were excluded. Baseline demographic data of the recruited mothers like age, diagnosis, gravid status, weeks of gestation at the time of presentation, betamethasone administration, etc., were recorded from case file. Investigations like Random Blood Sugar (RBS), serum haemoglobin (Hb), TC, PC, RBC count were carried out twice in each patient i.e., before and 48 hours after administration of betamethasone injection and the values recorded. They were then followed up till delivery. Newborns of the enrolled mothers were observed for parameters like birth weight, scores for respiratory distress viz., Downe’s score and Silverman Anderson score, diagnosis, need of ventilation, oxygen therapy, NICU admission and outcome at the time of discharge.
Statistical Analysis
Baseline data of the mothers and neonates was analysed using descriptive statistics, including mean, standard deviation and frequencies. Paired t-test was applied for maternal parameters like RBS, RBC, Hb, TC and PC to measure change from baseline after betamethasone administration. Independent sample t-test was applied in order to compare the difference between the mean Downe’s and the mean Silverman Anderson scores in neonates born within and after 24 hours of injectable betamethasone administration. The p-value of less than 0.05 was taken as statistically significant. A multivariable logistic regression model (with backward LR method) was generated in order to understand the individual contribution of each variable on the need for ventilation in neonates admitted into the NICU.
Results
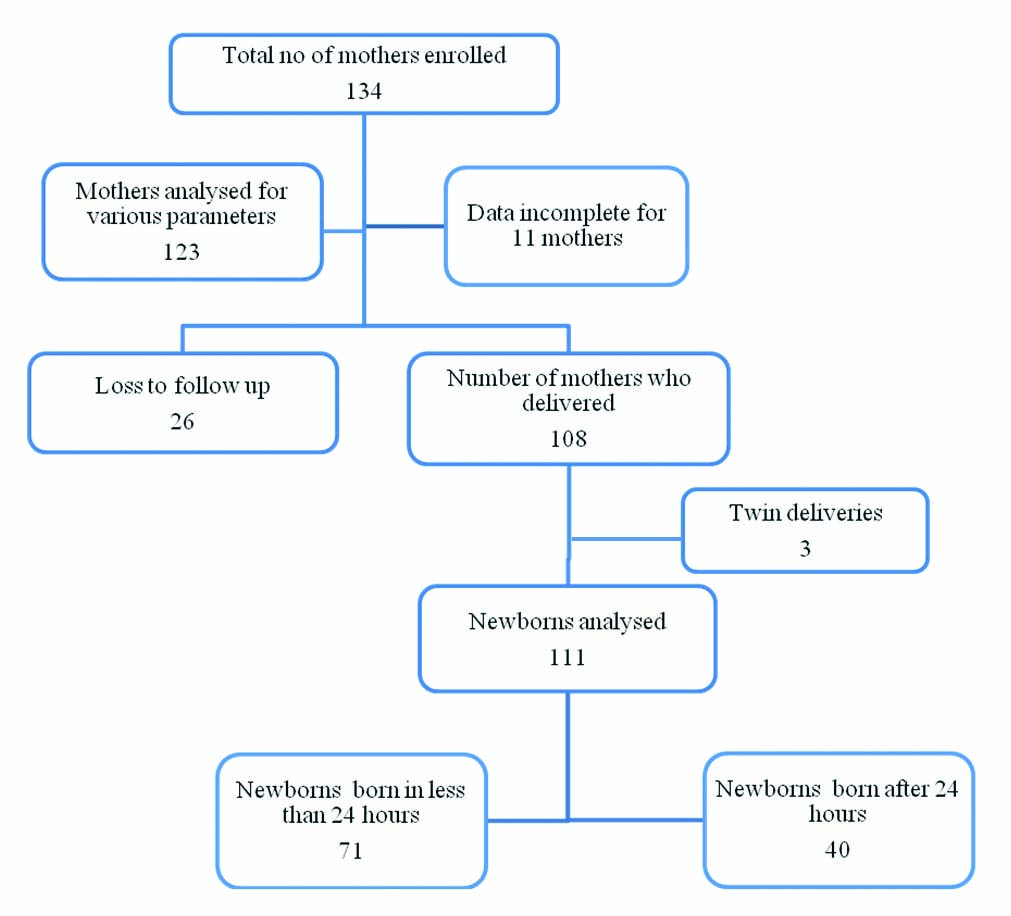
Total 134 mothers were enrolled according to inclusion and exclusion criteria. Out of these, there were 11 mothers for whom record of both the sets of investigations (before and after betamethasone administration) was not available. Thus, 123 mothers were analysed for various investigations. Out of total 134, 108 mothers delivered in our hospital; of them three delivered twins. Total 111 newborns were studied for neonatal parameters, 71 of whom were born within 24 hours of betamethasone administration [Table/Fig-1]. Mean (SD) age of the mothers was 25.6 (4.7) years. Mean (SD) weeks of gestation at the time of presentation were 33.58 (2.3). Eighty seven (64.9%) mothers were multigravida while 47 (35.1%) were primigravida. The most common diagnosis recorded was idiopathic preterm pain in 52 (38.8%) mothers followed by Pregnancy Induced Hypertension (PIH) in 20 (15%) mothers [Table/Fig-2]. Paired t-test revealed that mean RBC (p= 0.002) and mean PC (p<0.001) significantly reduced after administration of injection betamethasone as compared to baseline values whereas, mean TC increased (p=0.019). However, there was no significant change observed in mean RBS and mean Hb [Table/Fig-3]. Seventy-one newborns delivered within 24 hours of betamethasone administration and rest 40 delivered after 24 hours. Out of these 71, 51(71.8%) deliveries were preterm while 20 (28.7%) full term. Out of 111, 81 (72.9%) newborns were in low birth weight category (<2.5 kg) while 30 were having normal birth weight (>2.5 kg) [Table/Fig-4]. RDS at birth was recorded in only 14 neonates out of whom, 12 were born within 24 hours of betamethasone administration. The other recorded diagnoses were Transient Tachypnoea of Newborn (TTN), Birth Asphyxia (BA). Stillbirth and neonatal death was also recorded in seven and three cases respectively [Table/Fig-5]. Respiratory outcomes of neonates viz., RDS, TTN and BA were correlated with the maternal diagnosis. Idiopathic preterm was the diagnosis recorded most commonly in each group. RDS in neonates born in less than 24 hours was observed in anemic mothers (4) more commonly whereas, TTN developed more in mothers suffering from Premature rupture of membranes (2) [Table/Fig-6].
Algorithm of study participants.
Demographic details of mothers.
| Variables | Mean (SD) |
|---|
| Age (years) | 25.66 (4.73) |
| Systolic blood pressure (mm Hg) | 126.26 (16.78) |
| Diastolic blood pressure (mm Hg) | 81.06 (10.30) |
| Weeks of gestation | 33.58 (2.33) |
| N (%) |
| Gravid status (enrolled patients) | 134 (100) |
| Primigravida | 47 (35.07) |
| Multigravida | 87 (64.93) |
| Diagnosis: | |
| Idiopathic preterm pain | 52 (38.80) |
| PIH | 20 (14.92) |
| Antepartum eclampsia | 13 (9.70) |
| Anaemia | 14 (10.44) |
| Oligohydroamnios | 9 (6.71) |
| Premature rupture of membranes | 8 (5.97) |
$ More than 1 diagnosis was recorded in few patients
Characteristics of parameters before and after betamethasone administration in enrolled mothers (n= 123) {All the data are presented as mean (SD); Paired t-test for comparison of means}
| Vari- ble | Before betame- thasone | After betame- thasone | mean difference | Standard Error of difference of means | 95% confidence interval | p- value |
|---|
| RBC count | 4.0342 (0.916) (million/mm3) | 3.819 (0.6456) (million/mm3) | 0.21 (million/mm3) | 0.06 | 0.079 – 0.350 | 0.002 |
| PC | 2.34 (0.964) (lakh/mm3) | 2.17 (0.916) (lakh/mm3) | 0.17 (lakh/mm3) | 0.04 | 0.094 – 0.255 | 0.000 |
| TC | 12269.91 (9003.34) (thousands/mm3) | 14221.13(5398.07) (thousands/mm3) | - 1951.21 (thous- ands/mm3) | 823.34 | (-3581.1) (-321.32) | 0.019 |
| Hb level | 9.62 (2.61) (gm/dl) | 9.40 (1.69) (gm/dl) | 0.22 (gm/dl) | 0.18 | (-0.147) – 0.596 | 0.235 |
| RBS level | 101.49 (35.74) (gm/dl) | 96.41 (18.27) (gm/dl) | 5.08 (gm/dl) | 3.43 | (-1.712) – 11.874 | 0.141 |
Demographic characteristics of 111 newborns.
| Characteristics | number (%) |
|---|
| maturity | |
| Preterm | 70 (63.06) |
| Full term | 41 (36.94) |
| Sex | |
| Male | 63 (56.76) |
| Female | 48 (43.24) |
| Birth Weight | |
| Normal | 30 (27.03) |
| Low birth weight | 81 (72.97) |
| Diagnoses | |
| Normal | 74 (66.70) |
| Respiratory distress syndrome | 14 (12.60) |
| Transient tachypnoea of newborn | 7 (6.30) |
| Birth asphyxia | 2 (1.80) |
| Still born | 7 (6.30) |
| Neonatal death | 3 (2.70) |
| Others | 4 (3.60) |
Diagnosis in babies born within (n= 71) and after (n= 40) 24 hours of betamethasone administration.
| Diagnosis | < 24 hours N (%) | >24 hours N (%) |
|---|
| Normal | 42 (59.16) | 29 (72.5) |
| RDS | 12 (16.90) | 2 (5) |
| NND | 2 (2.82) | 1 (2.5) |
| SB | 6 (8.45) | 1 (2.5) |
| TTN | 4 (5.63) | 3 (7.5) |
| Birth asphyxia | 1 (1.41) | 1 (2.5) |
| DAMA | 4 (5.63) | 3 (7.5) |
| Total | 71 | 40 |
Correlation of neonatal respiratory outcomes with maternal diagnosis.
| Neonatal diagnosis (n) | Injection – delivery interval(n) | Maternal diagnosis(n) |
|---|
| RDS (14) | < 24hours (12) | Moderate anaemia (4) |
| | Idiopathic preterm pain (3) |
| | Abruption placenta (2) |
| | Premature rupture of membranes (1) |
| | Antepartum eclampsia (1) |
| | Oligohydroamnios (1) |
| >24hours (2) | Idiopathic preterm pain (2) |
| TTN (7) | < 24hours (4) | Premature rupture of membranes (2) |
| | Idiopathic preterm pain (1) |
| | Antepartum eclampsia (1) |
| >24hours (3) | Idiopathic preterm pain (1) |
| | Pregnancy induced hypertension (1) |
| | Rheumatic heart disease (1) |
| BA (2) | < 24hours (1) | Oligohydroamnios (1) |
| >24hours (1) | Abruption placenta (1) |
RDS: Respiratory Distress Syndrome; TTN: Transient Tachypnoea of Newborn; BA: Birth Asphyxia
At birth, 20 (19.2%) neonates had Downe’s score and Silverman Anderson scores ≥ four, suggesting respiratory distress. The independent sample t-test, done for comparison of Downe’s and Silverman Anderson score for neonates born within and after 24 hours of betamethasone administration, revealed that the mean scores were significantly higher in neonates who were born within 24 hours after betamethasone administration, as compared to those who were born after 24 hours (p-value<0.001) [Table/Fig-7]. Total 34 neonates required NICU admission; of these 25 required ventilation. A multivariable Logistic Regression (LR) model (with backward LR method) was generated to understand the individual contribution of each variable on the need of ventilatory support for the neonates admitted into the NICU. The logistic model revealed that the Silverman Anderson score (OR=4.751, 95% CI: 2.143, 10.535, P<0.0001) was significantly associated with need for ventilatory support in the neonates admitted into the NICU. The predictive value of the model was very good with 88.6% correct classification rate. The Nagelkerke coefficient of determination was 0.772.
Independent sample t-test for comparison of downe’s and Silverman Anderson score in neonates born within and after 24 hours of betamethasone administration {data presented as mean (SD)}.
| Score | IDI less than 24 hr | IDI more than 24hr | Mean difference | Standard error of mean difference | 95% confidence interval | p- value |
|---|
| Downe’s Score | 1.96 (1.953) | 0.55 (1.176) | 1.408 | 0.29 | 0.819 – 1.997 | <0.001 |
| SA score | 1.61 (1.863) | 0.30 (0.992) | 1.306 | 0.27 | 0.768 – 1.843 | <0.001 |
Discussion
In our hospital, which is a tertiary healthcare center, most of the patients referred to us are from primary and secondary healthcare centers. Referral is usually delayed due to various reasons and consequently the mothers tend to deliver soon after arriving to the emergency department. This accounts for a higher number of preterm deliveries, comparable to a couple of other studies [6,7].
Mean weeks of gestation in our study were 33.5. This corresponds with range of gestational weeks when corticosteroid administration is recommended to mothers in order to impart maximum benefits to the neonates born [8,9]. Another study by Danesh A et al., also reported similar findings [10]. Most common recorded diagnosis in our study was idiopathic preterm pain followed by PIH, anaemia, antepartum eclampsia, premature rupture of membranes, oligohydroamnios, abruptio placenta. This was comparable to the various diagnoses recorded in other studies by Mulder EJ et al., and Porto AMF et al., [11,12].
We observed that the mean red blood cell count significantly decreased after betamethasone administration as compared to baseline values (p=0.002). In another study by Niewegłowska N et al., steroid administration caused a significant decrease in RBC where the significant changes were observed between before and after second day of betamethasone administration (p<0.001) which was comparable to our study [13]. Mean PC reduced significantly after betamethasone administration as compared to baseline values (p<0.001). However in the study by Danesh A et al., the decrease in PC after betamethasone administration was not statistically significant [10]. This difference could be because in this study, majority of the patients delivered within 24 hours of drug administration leading to significant blood loss during delivery process. Thus, it was not possible to predict the effect of betamethasone on haematological parameters in such acute time interval. Corticosteroids like betamethasone affect circulating white blood cells [14]. We observed that mean leucocyte count increased significantly after betamethasone administration as compared to baseline values. This was similar to the studies by Vaisbuch E et al., and Kadanali S et al., [15,16]. In this study, 64% babies were born in less than 24 hours of betamethasone administration and rest after 24 hours which was comparable to findings reported in the study by Peltoniemi OM et al., [7]. Most of the neonates diagnosed with RDS were born in less than 24 hours. However, significance of this finding cannot be established due to the small number of subjects.
Significance of association of maternal diagnosis with respiratory outcome of neonate could not be established due to small sample size in each group. Roberts D and Dalziel SR reported that the incidence of RDS was significantly reduced in infants born before 48 hours and between one and seven days of treatment of mothers with corticosteroid, but not in those born before 24 hours in corticosteroid treated mothers [8]. Neonates with less than 24 hours of injection delivery interval had higher mean Downe’s and Silverman Anderson scores. This is in line with the observation that the number of neonates with RDS was more in the group born within 24 hours.
The number of neonates requiring admission into an intensive care unit was similar to another study, by Natile M et al., [17]. A multivariable logistic regression model revealed that Silverman Anderson score was significantly associated with need of ventilation for the babies admitted in NICU. A study by Haowei G et al., concluded that Silverman Anderson score can predict preterm respiratory failure in advance, and that it will therefore further aid clinicians in rapid assessment of the severity and extent of respiratory failure in such preterm infants [18].
Limitation
Sample size was a major limiting factor in this study. We were looking at an established practice of care; there was no control group in the study; therefore the association and strength of these results need to be assessed by performing a similar study in a larger population.
Conclusion
Betamethasone administration affects the haematological parameters in mothers in antenatal period nearing term. This study showed that there was no significant improvement in outcome of babies born within 24 hours of betamethasone administration to pregnant mothers in antenatal period. There is definitely some beneficial effect in babies born after 24 hours of betamethasone administration. Usage of antenatal corticosteroids in pregnant mothers should be subjected to a continuous quality improvement parameter and using quality cycles such as Plan-Do-Study-Assess (PDSA), their administration should be monitored by all healthcare practitioners and academic healthcare institutions in developing countries.
$ More than 1 diagnosis was recorded in few patients
RDS: Respiratory Distress Syndrome; TTN: Transient Tachypnoea of Newborn; BA: Birth Asphyxia