FBSS is a fairly common problem encountered in neurosurgical practice. This syndrome is characterised by recurrent or residual back pain after spinal surgery and has a reported incidence of 5%-40% [1]. FBSS has a wide spectrum of causes. The common causes include residual/recurrent disc herniation, epidural fibrosis or postoperative scarring, infection, improper instrumentation, arachnoiditis, mechanical instability following surgery, spinal stenosis and surgery at the wrong level [2].
Plain radiographs are helpful in assessing alignment but have limited role in identifying the cause. Computed Tomography (CT) can assess fixation device placement and bony spinal canal but has limited capability to distinguish disc herniation from scar tissue [3]. MRI with its multiplanar capabilities and superior soft tissue characterisation is the modality of choice for imaging the postoperative spine. It plays a pivotal role in identifying the cause of failed back syndrome in a majority of cases and helps to direct the appropriate therapy [4].
The treatment of FBSS is difficult and includes conservative measures and reoperation. The aim of this study was to evaluate the spectrum of imaging findings on postoperative MRI in patients with FBSS.
Materials and Methods
A total of 30 patients who had undergone spinal surgery and had symptoms of persisting or recurrent pain and/or persisting or worsening neurological symptoms postsurgery from September 2014 to September 2016 at our institution were included in this study. Patient consent was obtained in all cases and Ethical Committee Approval was taken for undertaking the study. Twenty six patients had undergone spinal surgery for degenerative disc disease and four patients had undergone spinal fixation for spondylolisthesis or trauma. The patients included were symptomatic for at least six months postsurgery. All patients underwent a thorough clinical and neurological examination prior to imaging with MRI.
Plain radiograph (AP and lateral) of the spine was done in all cases. The patients underwent MRI on 1.5 Tesla (GE) scanner. The sequences included T1WI, T2WI and STIR images in axial, coronal and sagittal planes and postcontrast fat saturated T1WI in all planes. Gadodiamide (Omniscan) contrast was administered in all cases. Dose of the contrast was 0.1 mmol/kg body weight. Imaging was done within two minutes after contrast administration to distinguish scar tissue from residual disc. Only patients with MRI compatible implants were included in the study. Patients with contraindication to MR imaging were excluded. In addition to MRI, NCCT was also done in patients with spinal implants to better delineate the placement of the metallic implant. Complete blood counts, ESR and blood cultures were obtained when deemed necessary depending on the clinical and imaging findings. Two patients underwent image guided (CT) aspiration cytology.
Results
A total of 30 symptomatic patients postspinal surgery were included in this study. There were 23 males and seven female patients. The age of the patients ranged from 22 to 65 years, majority (11) were in the age group of 50-60 years. A total of 26 patients had surgery for the degenerative disc disease and four patients had spinal fixation surgery. Spectrum of varied symptoms was noted [Table/Fig-1]. The average duration of symptoms ranged from six months to three years.
Distribution of symptoms.
| Symptoms | Number |
|---|
| Backache (worsening/recent onset) | 27 |
| Neurological deficit (worsening/recent onset) | 11 |
| Mechanical instability | 02 |
| Fever | 01 |
Different causes of failed back surgery were appreciated on imaging [Table/Fig-2]. Sixteen (53%) patients had recurrent/residual disc herniation. The herniated disc showed continuity with and was similar in signal intensity on all pulse sequences with the parent disc. On immediate postcontrast images, there was no enhancement of the herniated disc [Table/Fig-3]. A thin rim of enhancement along the periphery of the disc was appreciated in some cases. Secondary spinal canal stenosis was seen in seven patients. Caudal migration of the disc was noted in four patients. Disc sequestration was noted in one case, with the detached fragment seen lying superior to the affected level in the spinal canal [Table/Fig-4].
Distribution of aetiology.
| Cause of FBSS | N=30 (100%) |
|---|
| Recurrent/residual disc prolapse | 16 (53%) |
| Epidural scar | 06 (20%) |
| Disc prolapsed with scar tissue | 03 (10%) |
| Arachnoiditis | 02 (7%) |
| Postoperative discitis | 02 (7%) |
| Malaligned implant | 01 (3%) |
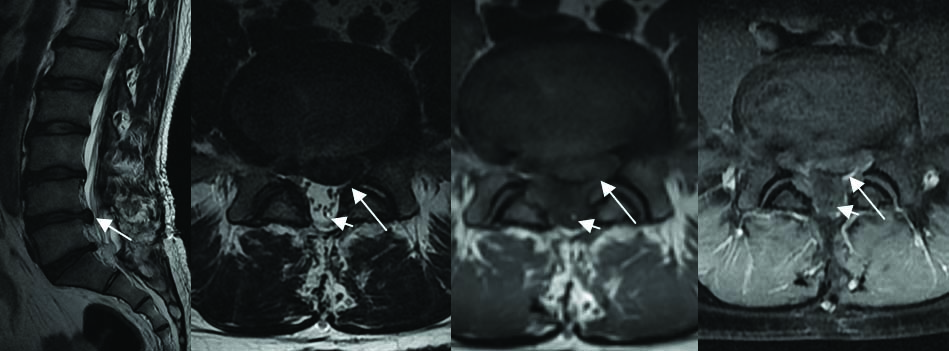
Recurrent Disc Herniation: Post Laminectomy status. Sagittal T2W image (a); Axial T2W image (b) Axial T1W image (c); Axial post contrast T1 fat suppressed image (d); Shows recurrent left central and paracentral disc herniation (arrow) at L4-5 level. This disc herniation shows no enhancement on postcontrast images and is causing compression on the left traversing nerve roots. Incidental finding of fatty filum terminale is seen (small arrow). (All Image left to right)
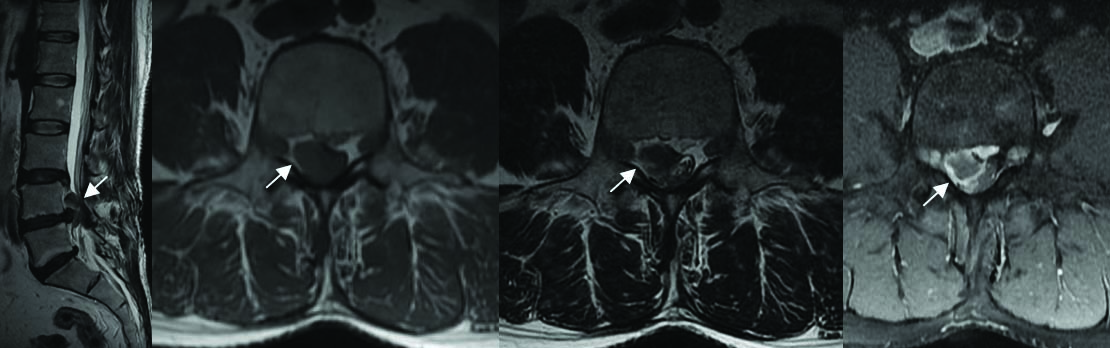
Disc Sequestration: Post laminectomy status. Sagittal T2W image (a); Axial T1W image (b); Axial T2W image (c); Axial post contrast T1 fat suppressed image (d); Shows cranially migrated sequestered disc fragment (arrow) at L4 vertebral level compressing the thecal sac. The disc fragment shows no enhancement on postcontrast images. There is thin peripheral rim of enhancement seen around this sequestered fragment suggestive of scar/inflammatory granulation tissue. (All Image left to right)
Six (20%) patients had epidural scar tissue appearing hypointense on T1WI and T2WI. In the early postcontrast images, brisk enhancement of the scar tissue was appreciated. In most cases, the scar tissue was seen encasing the nerve roots, which appeared as oval hypointense structures surrounded by the enhancing scar tissue [Table/Fig-5].
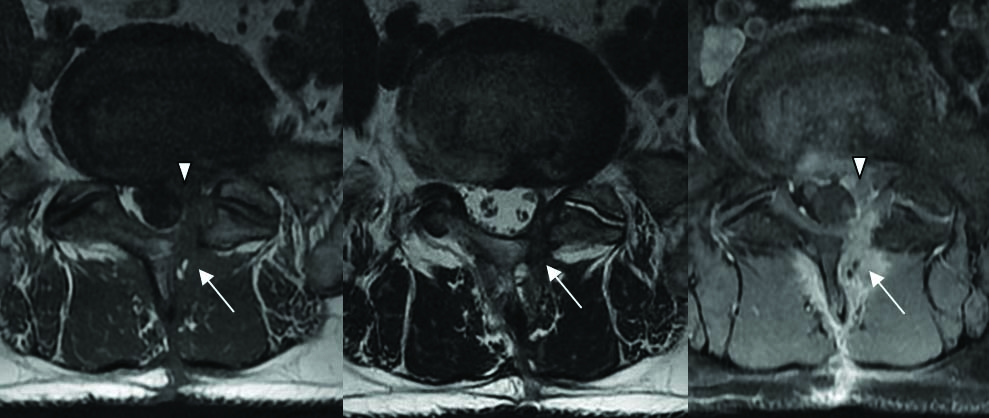
Epidural Scar: Axial T1W image (a); Axial T2W image (b) Shows epidural scar (arrow) in the left partial laminectomy defect and epidural space at L4-5 level. This scar tissue is encasing the left traversing nerve root (arrowhead) and appears hypointense on T1W and T2W images. Axial postcontrast T1 fat suppressed image (c) Show enhancing scar tissue surrounding the non enhancing nerve root. (All Image left to right)
Three patients (10%) had recurrent disc herniation and scar tissue. The disc showed continuity with the parent disc and did not enhance after contrast administration and was surrounded by the enhancing scar tissue.
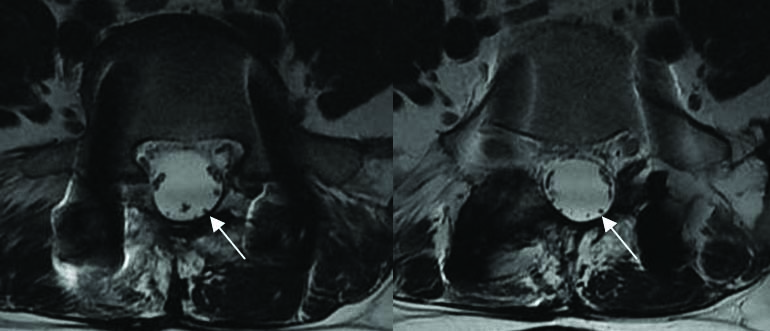
Two (7%) patients had evidence of postsurgery arachnoiditis. One case had clumped up nerve roots forming a nodular lesion appearing hypointense on T1 and T2WI [Table/Fig-6]. In the second case, the nerve roots were displaced peripherally along the dura with CSF occupying the center of the thecal sac [Table/Fig-7]. No enhancement of the nerves was seen on postcontrast images in both cases.
Arachnoiditis: Axial T2W images (a,b) At L2-3 level (post laminectomy status) shows clumping of the cauda equina nerve roots (arrow). (All Image left to right)
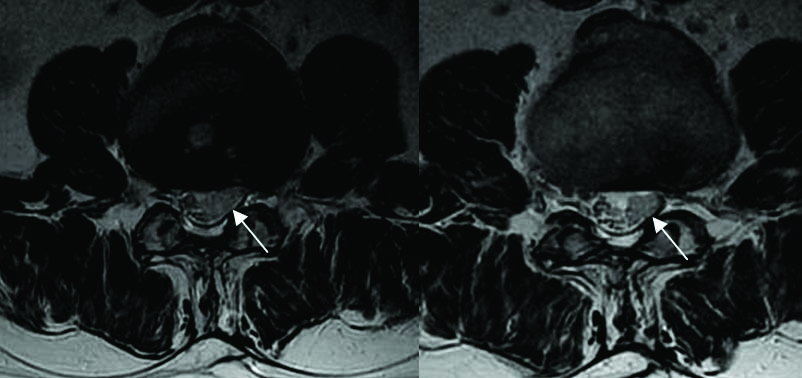
Arachnoiditis: Axial T2W images (a,b) At the level of L4-5 shows peripherally displaced cauda equina nerve roots (arrow) with empty thecal sac. Interpedicular screws fixation seen in situ. (All Image left to right)
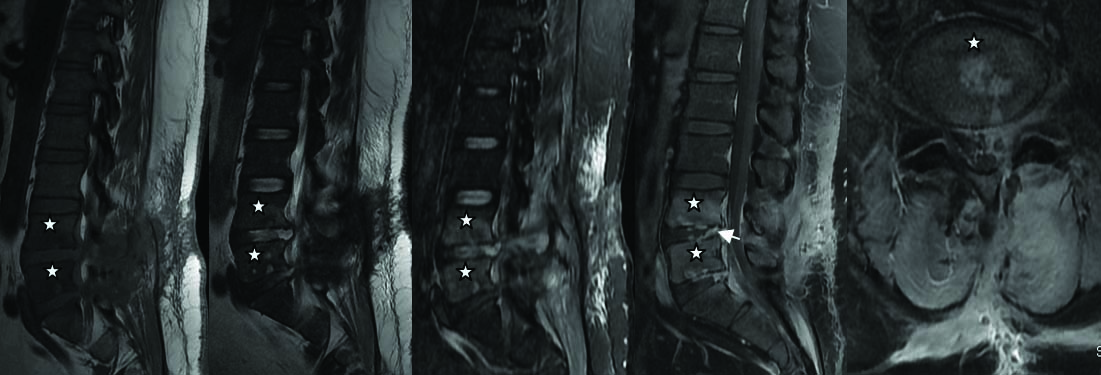
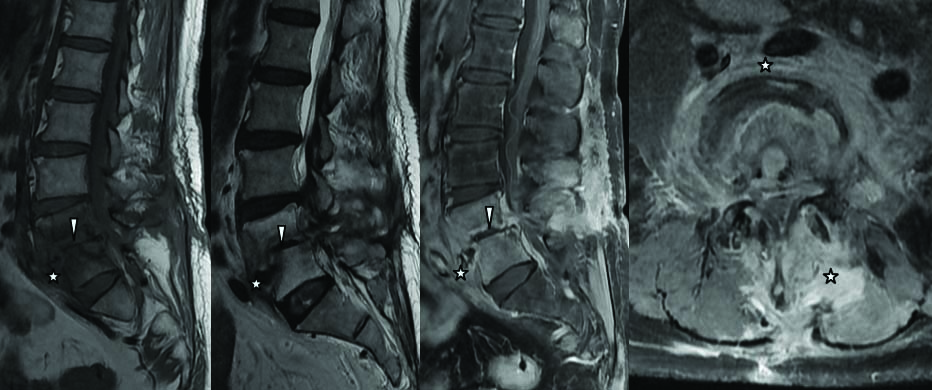
Two (7%) patients had hyperintense signal in the disc on T2WI with marrow oedema of the adjacent vertebral bodies, appearing hypointense on T1WI and hyperintense on T2WI & STIR imaging. On postcontrast images enhancement was seen involving the disc and the vertebral bodies. In one case, there was extensive enhancing granulation tissue seen around the disc and the vertebrae, with extension into the paravertebral tissues and the spinal canal. Findings were suggestive of postsurgery discitis [Table/Fig-8,9]. Patients underwent image guided aspiration cytology and received appropriate antibiotics. Repeat scanning after 12 weeks showed regression of the imaging findings and symptomatic improvement in both cases.
Spondylodiscitis: Post laminectomy status at L4-5 and L5-S1 level. Sagittal T1W image (a); T2W image (b); STIR image (c) Shows marrow oedema (star) involving the bodies of L4, L5 and S1 vertebrae appearing hypointense on T1W, hyperintense on T2W and STIR images. Hyperintense signal seen in the L4-5, L5-S1 disc on T2W and STIR images with adjacent end plate irregularity. On postcontrast T1 fat suppressed sagittal (d) and axial (e) images, there is enhancement seen in the bodies of these involved vertebrae and the intervening disc (arrow). (All Image left to right)
Spondylodiscitis: Post laminectomy status at L4-5 level. Sagittal T1W image (a); T2W image (b) Shows mildly reduced vertical height of L4, L5 vertebrae with adjacent end plate irregularity and loss of intervening disc height (arrow head). There is associated pre- paravertebral soft tissue component (star) seen at L4-5 level. Extensive bone marrow oedema noted involving the bodies of L4, L5 vertebrae showing hypointense signal on T1W images and hyperintense signal on T2WI. On postcontrast T1 fat suppressed image sagittal (c) And axial (d) Images, there is marked heterogeneous enhancement seen in the bodies of these involved vertebrae and in the pre and paraspinal granulation tissue (star). (All Image left to right)
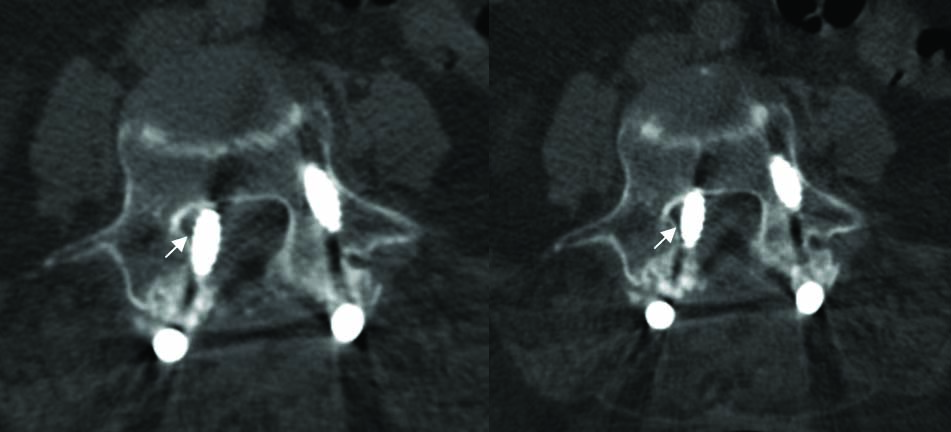
One patient had a malaligned implant postspinal fixation for spondylolisthesis. MR images were suggestive of malalignment despite image degradation due to the metallic implant. NCCT spine was done which confirmed the malalignment and medial displacement of the implant [Table/Fig-10].
Malaligned screws: Post laminectomy status with spinal fixation device. NCCT lumbar spine axial (a,b) Images in bone algorithm shows displaced right interpedicle metallic screw with compression of thecal sac and nerve roots (arrow). (All Image left to right)
Eight patients underwent reoperation for disc herniation and 01 patient for malaligned spinal implant following imaging.
Plain radiographs revealed postoperative status of laminectomy and fixation device placement and were helpful to assess spinal alignment. However, they were of limited value in providing information regarding the aetiology of symptoms in most cases.
Discussion
Imaging of the spine in the early postoperative period should be done with caution. Mass effect from the postoperative oedema and hemorrhage can simulate disc herniation. In the early postoperative period, there is normal enhancement of the vertebral end plates, post diskectomy disc space, paraspinal muscles, facet joints and the nerve roots. These changes gradually resolve over a period of six months [1-3,5].
Plain radiographs have a limited role and can be used to assess the alignment of the spine. However, they are not very helpful to evaluate the soft tissues and the disc. CT can accurately show the bony details and implant alignment, however cannot reliably differentiate residual disc from scar tissue [6,7]. Currently, MRI is the modality of choice for imaging of the postoperative spine. Its major advantages include multiplanar imaging capability, superior soft tissue resolution and excellent tissue characterization. Contrast enhanced scans are an essential component of postoperative imaging. They help to differentiate scar tissue from recurrent or residual disc herniation [1,8].
Studies confirm that disc herniation is responsible for 7%-37% of cases of FBSS [9-12]. A total of 53% patients in this study had residual/recurrent disc herniation. The smaller sample size of this study is probably the reason for the higher percentage of cases. The protruded disc was seen in continuity with the parent disc and showed no enhancement in the early postcontrast images. These findings are consistent with the postoperative MRI findings as elucidated in studies [1,2]. We had one case who had disc sequestration.
Scar tissue has increased vascularity and shows enhancement in the early postcontrast scans. Disc material is relatively avascular and does not enhance in the early postcontrast scans, however, it may show enhancement on delayed scans; hence the importance of scanning early following contrast administration [2,8,9]. In this study, 20% patients had epidural scar tissue with characteristic features on postcontrast images, as elaborated in published literature. The scar tissue was seen encasing the nerve roots which did not enhance. Recurrent disc prolapse and epidural fibrosis may coexist and is not an uncommon finding [9]. Also, it is known that a prolapsed disc may incite fibrosis in the absence of surgery [2,9]. About 10% patients had presence of recurrent disc herniation and scar tissue.
Three MRI patterns of arachnoiditis have been described. These include clumped nerve roots; an empty thecal sac caused by adhesion of the nerve roots to its walls; and an intrathecal soft tissue mass with a broad dural base. Contrast enhancement of the thickened roots may or may not be observed [1,13]. A total of 7% patients had postsurgery arachnoiditis with features of clumped nerve roots and empty thecal sac with peripherally displaced nerve roots. No enhancement of the nerve roots was seen. These findings are in agreement with the MRI patterns of arachnoiditis as detailed in the published literature [9,14].
Postoperative spondylodiscitis has been reported in up to 3% of patients in various series [1,15]. Diagnosis of spondylodiscitis in the postoperative period can be challenging especially in view of the normal enhancement of the disc and end plates in the early postoperative period. Presence of soft tissue collections, clinical suspicion and constellation of contrast MRI findings is helpful to suggest the diagnosis. A total of 7% patients in this study had postoperative spondylodiscitis. The diagnosis of infection was confirmed with image guided aspiration cytology. Both patients responded to antibiotics with symptomatic relief and regression of the findings on imaging.
Malalignment of fixation device can result in FBSS and this was seen in one patient. Pseudo-meningocele are CSF collections which can result following surgery due to inadvertent dural tear. These collections may compress the nerve roots and can be the cause of pain. Mechanical instability such as facet subluxation, pseudoathrosis following surgery may also be the cause of FBSS in some patients [16,17]. No such findings were appreciated in this study.
Limitation
Possible limitations of the study are that only a small sample size (n=30) was evaluated, due to the limited availability of patients.
Conclusion
FBSS is a multifactorial syndrome not uncommonly encountered in neurosurgical practice. Contrast MRI with its excellent resolution and multiplanar capabilities is the modality of choice for imaging these patients and plays a pivotal role in identifying the potential cause of symptoms and helps in guiding the correct treatment.