World population of elderly (people aged 60 years and above) has increased in last two decades at a pace faster than any other times before. As per World Health Organization (WHO), between 2015 and 2050, it is expected that proportion of the world’s population over 60 years will double from about 12% to 22%. Similarly, the number of people aged 80 years or older will rise from 125 million to 434 million in same period [1]. India will also not be untouched by this demographic transition in coming decades. The number of elderly in India has increased by 54.77% in the last 15 years against 42.34% rise in the working population (15-59 years of age) during the same time period [2]. The proportion of the people with age more than 60 years will grow from 8% in 2010 to 19% in 2050 while the population of those aged 80 years and older will expand from 0.8% to 3%. By the year 2042, the proportion of people aged 60 years and older will exceed that of people in 0–14 year’s age group in India [3].
This profound shift in the proportion of older Indians, taking place in the context of changing family relationships and limited social support system will bring with it a variety of social, economic and health care policy challenges. One direct implication of this would be increase in the prevalence of chronic conditions such as cardio vascular diseases, chronic respiratory diseases, locomotor disorders and mental disorders etc. Estimates say that nearly 45% of India’s disease burden is projected to be borne by older adults in 2030, when the population age groups with high levels of chronic conditions will represent a much greater share of the total population [3].
A number of social security measures have been taken by the Indian government. The government of India came out with the National Policy for Older Persons in 1999 to promote the healthcare, financial security, nutrition, shelter, education and welfare of senior citizens in India [4].
IGNOAPS was launched in 1995 subsequently to provide monthly pension to elderly who are Below Poverty Line (BPL). In 2000, Annapurna scheme was launched which aimed at providing food security to elderly [4].
Maintenance and Welfare of Parents and Senior Citizen Act 2007 aimed to ensure need based maintenance for parents and senior citizens, protection of their rights and welfare was introduced [4]. A comprehensive National Program for Health Care of the Elderly (NPHCE) was launched subsequently in 2010 with the vision to provide accessible, affordable and high-quality long-term, comprehensive and dedicated care services to ageing population [4].
These social security measures are important and at times the only means of support for elderly. However, to assess the impact and steps for further improvement in future of such measures, it is important to have information about the level of awareness and practical problems faced by elderly while utilizing them. Therefore, this study was conducted with an objective to assess awareness, utilization and barriers faced by elderly while utilizing social security schemes in a secondary care hospital situated in a rural area in Delhi.
Materials and Methods
This was a cross-sectional study conducted among individuals aged 60 years and above, attending a secondary level care hospital situated in a rural area in Delhi, Pooth Khurd, who gave written informed consent to participate in the study. Sample size was calculated on the basis of a previous study by Murugen PB et al., in which prevalence of awareness about social security schemes was 73.2% and that of utilization of old age pension scheme among study subjects was 73% [5]. Taking confidence interval of 95% with absolute error of 5%, the sample size was calculated to be 313. A total of 360 subjects were included in the study. These subjects were interviewed and questionnaire was filled by the investigator during each interview. Study subjects were selected by simple random sampling method.
Data was collected using a pretested semi-structured schedule, which included socio-demographic profile, awareness and utilization of various social security schemes and other measures taken by the government for the elderly, and difficulties faced in availing these schemes. Variables were decided based on the variables used in previous similar studies [2,4,5]. Pretesting was done at the secondary level hospital in rural area of Delhi among 50 elderly subjects attending medicine OPD. Accordingly, questionnaire was edited and modified. Information was also obtained about financial dependence and family support in providing care.
Statistical Analysis
Data was analysed using SPSS (version 17.0). Results were presented in simple proportions and means (±SD). Chi-square test was used to observe any statistical significance of difference between proportions. The results were considered statistically significant if p-value was less than 0.05.
The study was approved by the Institutional Ethics Committee of the hospital.
Results
Sociodemographic Profile
As shown in [Table/Fig-1], the study sample consisted of 318 (88.3%) subjects aged 60-74 years and 33 (9.2%) in 75-84 years age group. A majority of study participants were females-195 (54.2%) and 165 (45.8%) were males. Mainly the study samples were Hindus (89.7%), married (60.3%) and were not engaged in any occupation (82.8%). Those who were residing in joint families were 260 (72.2%) while 24 (6.7%) subjects were staying alone.
Socio-demographic profile and awareness about social security schemes among study subjects.
| Characteristic | N=360 Number (%) | Awareness about social security schemes |
|---|
| IGNOAPS N (%) | Annapurna N (%) | Senior Citizens Act N (%) |
|---|
| Age: |
| p-value | | p=0.52 | p=0.4 | p=0.51 |
| 60-74 years | 318 (88.3) | 257 (80.8) | 174 (54.7) | 10 (3.1) |
| 75-84 years | 33 (9.2) | 29 (87.9) | 14 (42.4) | 0 (0.00) |
| >85years | 9 (2.5) | 8 (88.9) | 5 (55.6) | 0 (0.00) |
| Sex: |
| p-value | | p=0.01 | p=0.67 | p=0.04 |
| Male | 165 (45.8) | 145 (87.9)* | 86 (52.1) | 8 (4.8)* |
| Female | 195 (54.2) | 149 (76.4) | 107 (54.9) | 2 (1.0) |
| Education: |
| p-value | | p=0.17 | p=0.59 | p=1.00 |
| Literate | 181 (50.3) | 153 (84.5) | 100 (55.2) | 5 (2.8) |
| Illiterate | 179 (49.7) | 141 (78.8) | 93 (52.0) | 5 (2.8) |
| Occupation: |
| p-value | | p=0.72 | p=0.78 | p=0.22 |
| Working | 62 (17.2) | 52 (83.9) | 32 (51.6) | 0 (0.0) |
| Not-working | 298 (82.8) | 242 (81.2) | 161 (54.0) | 10 (3.4) |
| Religion: |
| p-value | | p=0.36 | p=1.00 | p=1.00 |
| Hindu | 323 (89.7) | 266 (82.4) | 173 (53.6) | 9 (2.8) |
| Others | 37 (10.3) | 28 (75.7) | 20 (54.1) | 1 (2.7) |
| Family type |
| p-value | | p=0.33 | p=0.81 | p=0.67 |
| Nuclear | 76 (21.1) | 66 (86.8) | 43 (56.6) | 2 (2.6) |
| Joint | 260 (72.2) | 210 (80.8) | 138 (53.1) | 8 (3.1) |
| Staying alone | 24 (6.7) | 18 (75.0) | 12 (50.0) | 0 (00.0) |
| Caste: |
| p-value | | p=0.25 | p=0.94 | p=0.53 |
| Scheduled casts (SC)/ Scheduled tribe (ST) | 94 (26.1) | 72 (76.6) | 49 (52.1) | 3 (3.2) |
| Other backward Classes (OBC) | 167 (46.4) | 137 (82.0) | 90 (53.9) | 3 (1.8) |
| General | 99 (27.4) | 85 (85.9) | 54 (54.5) | 4 (4.0) |
| Place of stay |
| p-value | | p=0.06 | p=0.07 | p=0.16 |
| Own house | 266 (73.9) | 222 (83.5) | 152 (57.1) | 10 (3.8) |
| Rented house | 86 (23.9) | 64 (74.4) | 37 (43.0) | 0 (0.0) |
| Old age home/ Homeless | 8 (2.2) | 8 (100.0) | 4 (50.0) | 0 (00.0) |
| Marital status: |
| p-value | | p=0.01 | p=0.10 | p=0.74 |
| Married | 217 (60.3) | 197 (90.8)* | 124 (57.1) | 7 (3.2) |
| Unmarried/Widow/ Separated/ Divorcee | 143 (39.7) | 97 (67.8) | 69 (48.3) | 3 (2.1) |
| Below poverty line |
| p-value | | p=0.40 | p=0.01 | p=0.04 |
| Yes | 223 (61.9) | 179 (80.3) | 140 (62.8)* | 3 (1.3)* |
| No | 137 (38.1) | 115 (83.9) | 53 (38.7) | 7 (5.1) |
Figure with * mark were statistically significant (p<0.05). Chi-square test applied.
A house was owned by 266 (73.9%) subjects, 86 (23.9%) were residing in a rented house and rest stayed in old age homes.
Awareness about Social Security Measures
Awareness about IGNOAPS was higher than other social security schemes as about four fifth of the subjects were aware of this as compared to about half who were aware of Annapurna scheme and only 10 (2.8%) subjects knew about senior Citizens Act. There was significant difference in awareness about Senior Citizens Act with gender (p<0.05). Subjects who were below poverty line were more aware about Annapurna scheme with 140 (62.8%) subjects knew about the same as compared to 53 (38.7%) who were above poverty line (p<0.05). A total of 294 (81.7%) subjects were aware about Indira Gandhi National Widow Pension scheme. Females (76.4%) were significantly more aware about the same as compared to males (87.9%) (p<0.05). Subjects who were widow/separated/ single or divorced were less aware (67.8%) about the same as compared to those who were married (90.8%) (p<0.05).
[Table/Fig-2] shows results when the study subjects were inquired if they were aware about other measures of support provided to them by government. A little less than half were aware about bus travel concession provided to elderly in form of bus pass. Out of 360 subjects, 41 (11.3%) subjects were not aware about such measures of government to support elderly.
Awareness about social support measures among study subjects (n=319)
| Support measures | Number | Percentage (%) |
|---|
| Bus travel concession | 162 | 45 |
| Train travel concession | 58 | 16.1 |
| Air travel concession | 8 | 2.2 |
| High interest rates by banks | 37 | 10.2 |
| Income tax benefits | 35 | 9.7 |
| NPHCE | 19 | 5.3 |
Frequency distribution table.
Only 36 (10.0%) subjects reported that they have done savings for old age. A small number of subjects, 7 (3.6%) among females and 29 (17.6%) among males reported that they did savings for old age which was statistically significant (p<0.05). A total of 182 (50.6%) subjects said that they were dependent on their family members for their living. Higher percentage of those who were non-working (54.0%) than working (33.9%) reported that they are dependent on family (p<0.05). When asked about family support, 213 (59.2%) subjects reported that their family members take care of them well while 147 (40.8%) subjects responded that their family members do not take care of them well. There was significant difference between gender where 110 (66.7%) among males and 103 (52.8%) among females said that their families take care of them well (p<0.05). Similarly, 90 (65.7%) subjects who were above poverty line responded that their family members take care of them well than 123 (55.2%) subjects who were below poverty line (p<0.05). A significantly higher number of subjects who belonged to OBC category (27.5%) agreed that they were satisfied with their lives as compared to SC/ST (4.3%) and general category (13.1%) (p<0.05). Noticeably, only 2 (0.6%) subjects were having health insurance to meet their health security cover.
[Table/Fig-3] shows sources of information about various social security schemes and measures taken for elderly. Most common source of information was ‘local leaders’ as reported by 130 (36.1%) subjects. Family and friends were the next most common sources as reported by 112 (31.1%) subjects. Television was third most common source as told by 23 (6.4%) subjects. Out of the total 360, 48 (13.3%) subjects could not remember their source of information or had no such source.
Sources of information about social security schemes and measures among study subjects (n=312).
| Sources of information | Number | Percentage |
|---|
| Local leaders | 130 | 36.1 |
| Family/friends | 112 | 31.1 |
| Television | 23 | 6.4 |
| Panchayat (local government members) | 20 | 5.6 |
| Radio | 18 | 5.0 |
| Hoardings | 5 | 1.4 |
| Posters | 4 | 1.1 |
Frequency distribution table.
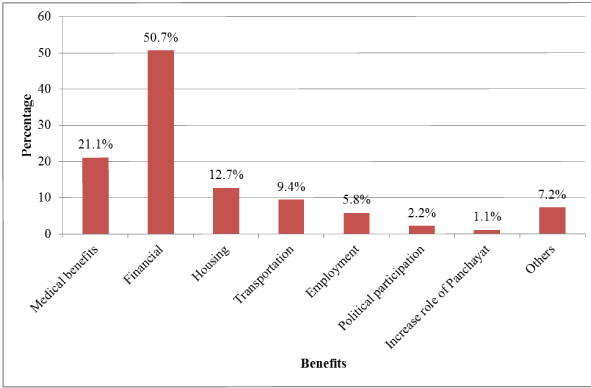
When asked about additional benefits study subjects expect from government, 76 (21.1%) subjects responded that more medical benefits, 183 (50.7%) demanded for more financial support, 46 (12.7%) said housing facilities, 34 (9.4%) expected for more transportation facilities, 21 (5.8%) asked for employment opportunities, 8 (2.2%) demanded for more political participation for them and 4 (1.1%) desired an increase in their role in local governance (panchayat) as shown in [Table/Fig-4].
Additional benefits expected from government by study population
Subjects below Poverty Line
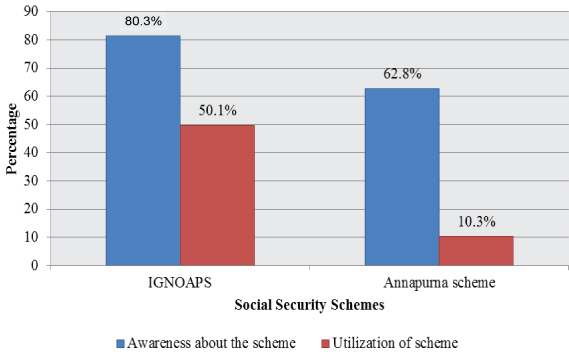
Following analysis has been done only among subjects who were below poverty line and were eligible for social security schemes like IGNOAPS and Annapurna scheme. Among 223 subjects who were below poverty line, 179 (80.3%) were aware of IGNOAPS while only 112 (50.2%) of them were utilizing the scheme. Annapurna scheme was known to 140 (62.8%) subjects but only 23 (10.3%) were utilizing the same as given in [Table/Fig-5]. They were asked about the problems faced in utilization of social security schemes. The options given to the subjects were corruption, difficulty in knowing whom and where to approach, tedious administrative formalities, other problems and no problem faced and the answers were 11.2%, 20.6%, 38.1%, 20.1% and 10% respectively. When asked if they are financially dependent on their family members, 55.2% answered yes. On probed regarding their major sources of finance, 79.4% were found to be dependent on their children and 31.8% reported that they have to borrow money from relatives often, to meet their expenses.
Awareness and utilization of social security schemes among those eligible for the same among study subjects
A high proportion of (40.8%) subjects grumbled that their family members do not take care of them well. When asked if they were satisfied with their lives, only 24 (10.8%) responded positively while 199 (89.2%) were dissatisfied with their lives.
Among below poverty line subjects, majority (87.4%) said that government has not taken adequate steps for welfare of the elderly. When enquired about the additional benefits they need from government, following responses were given – medical (18.8%), financial (57.4%), housing (13.9%), transportation (10.3%), employment opportunities (7.6%) and participation in local politics (1.3%).
Discussion
The present study was conducted among 360 elderly individuals who came to seek health care services in a secondary level hospital situated in Delhi. The study population mainly comprised of subjects who were in 60-80 years age group. Hindus were found to be predominant in the study population in comparison to Muslims and Christians, which reflect the national level population structure based on religion. About half of the subjects were illiterate. Such profile was similar to the elderly profile reported by Dhanasekaran G in his study carried out in a rural area in Tamil Nadu [6].
A significant proportion of elderly were aware about IGNOAPS. It was known to 80.3% subjects and there was no association found with age, family type, caste. Lesser known than IGNOAPS was Annapurna scheme, which was known to 53.6% subjects. Awareness was significantly higher among those who were BPL. These findings were consistent with that reported by Srivastava AK et al., in their study conducted in district Dehradun [7]. In that study, awareness of IGNOAPS was observed in 74.6% of the elderly [7]. Only 10 (2.8%) subjects knew about Senior Citizens Act, with a higher proportion of males than females were aware of the same. Bus travel concession was known to about 45% subjects but other measures like National Program for Healthcare of the elderly, interest rates etc. were known to very less subjects. This is lower than figures reported by Joseph N et al., in their study conducted in Mangalore city. The possible reasons could be higher literacy rate of subjects in that study and rural urban differentials [8].
An important finding was that despite the fact that 72.2% subjects were living in joint families, only 59% subjects replied that their family members take care of them well. There were gender differentials seen with this aspect where significantly higher number of males were taken care well by their families than females. Similarly, more literate subjects than illiterate were taken care well by families. This reflects impact of education not only in livelihood and living standard but also in social support system at household level. Such gender differentials in social support among elderly have been documented by another study also where males were more likely to be heard and involved in decision making at household level as compared to females [9].
Main sources of information were local leaders followed by family and friends. Hence, local leaders should take more steps to raise awareness about social security measures among elders in their areas and to remove barriers wherever possible. Envisioning recreation centers for elders, where they can gather together and share information with each other can prove to be an added advantage.
Major barriers reported were corruption (11.2%) and tedious administrative procedures (38.1%). This is consistent with findings of a previous mentioned study in which also bribe, procedural delay and nobody to guide were main barriers [5]. Innovative steps using information technology should be taken to make the procedure easier and to reduce the number of visits to offices for applying and tracking their applications. Corruption charges if found true should be dealt with stringent punitive actions since it deteriorates the faith of elders in system and deprive them of their rights.
Majority of subjects asked for additional financial benefits from government. The reason could be meager amount of monthly pension which is insufficient to fulfill even basic needs of a person. Insufficiency of amount has been reported by another study carried out by Nivedita BM et al., in Bengaluru as well, in which 79% subjects responded that the amount is insufficient for meeting basic needs [10]. Medical benefits were next expected need from government since health care cost of chronic illness is huge, especially in setting where majority of subjects belong to low income group. Although, government has started a separate program NPHCE for promoting geriatric health care facilities and competence among treating medical staff, the program is still in its infancy state with hardly any required infrastructure. Elderly in India are currently facing risk of dual medical problems, i.e., both communicable as well as non–communicable diseases. At present, most of the geriatric OPD services are available at tertiary care hospitals located in urban areas [11]. This tertiary care is often too expensive for people with limited income sources. As a result, those with conditions requiring tertiary care often go untreated or are left with devastating hospital bills, both of which exacerbate poverty [12]. More steps are needed by government to provide support for medical expenses for elderly population.
When analysis was done for BPL subjects who were eligible for IGNOAPS and Annapurna scheme, it was found that although 80.3% were aware of IGNOAPS only 50.2% were utilizing the scheme. This is comparable to a previously mentioned study in which 45.4% subjects were utilizing IGNOAPS [7]. Similarly, 62.8% were aware of Annapurna scheme but only 10.3% were utilizing the same. This shows a gap between awareness and actual utilization of schemes. Advertisements on mass media like television, radio, newspaper, etc., can help in increasing awareness. Corruption, difficulty in knowing whom and where to approach and tedious administrative formalities were the major barriers. Inconsistencies in identification of beneficiaries, political influence and corruption are known factors reported earlier also which poses a serious question on the implementation of this scheme [13].
Limitation
Firstly, the study involved subjects only from rural area. It would have been more representative of the population if elderly from urban area were also involved. Secondly, since study was conducted at secondary level hospital due to resource constraints, only those elderly patients who were coming to the hospital were included in the study. For more generalizable results, healthy elderly subjects from the residential areas also could have been included.
Conclusion
The present study highlights important areas of concern in providing social security for elderly population in rural area of Delhi. About 79.4% of elderly were aware and 45% of the eligible subjects were utilizing pension scheme. Awareness about other measures of social security was low. Major barriers were corruption, tedious administrative procedures and difficulty in identifying where and whom to approach for information regarding social security schemes. It is recommended that local leaders should take efforts to make elders aware of such measures. The expectations of elders for more financial security and medical benefits should be looked into in framing future polices for them. Awareness generation, provision of information on how to approach the concerned authority for utilizing the scheme and ease of administrative procedures should be an integral part of any social security scheme or measure.