Clinical Outcome of Treatment of Diaphyseal Fractures of Humerus Treated by Titanium Elastic Nails in Adult Age Group
Amit Verma1, Sudhir Shyam Kushwaha2, Yasir Ali Khan3, Farid Mohammed4, Subhanshu Shekhar5, Ankur Goyal6
1 Assistant Professor, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow, Uttar Pradesh, India.
2 Assistant Professor, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow, Uttar Pradesh, India.
3 Assistant Professor, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow, Uttar Pradesh, India.
4 Associate Professor, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow, Uttar Pradesh, India.
5 Junior Resident, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow, Uttar Pradesh, India.
6 Junior Resident, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sudhir Shyam Kushwaha, Assistant Professor, Department of Orthopaedics, Era’s Lucknow Medical College, Lucknow-226003, Uttar Pradesh, India.
E-mail: sudhirshyamkushwaha@gmail.com
Introduction
Humerus shaft fracture is one of the most common injuries to the musculoskeletal system, which are managed both conservatively and surgically. There are pitfalls, advantages and disadvantages in each method. The individual fracture analysis determines the therapeutic options.
Aim
To assess the clinical outcome of treatment of diaphyseal fractures of humerus treated by Titanium elastic nail in adult age group by DASH scoring.
Materials and Methods
It was a prospective study of 20 cases of diaphyseal fracture of humerus admitted to Era’s Lucknow Medical College and Hospital between October 2014 and September 2015 treated with close reduction and internal fixation with titanium elastic nail. Functional outcome was evaluated using DASH scoring system and radiological outcome was evaluated by serial radiographs. The data was processed with SPSS software version 16.0 (Chicago, inc. USA) and it was summarized in proportion and percentage.
Results
In our series of 20 patients, 17 were males and three were females. Most of the patients were between 30-50 years of age (mean 38 years). Most common mode of injury, side of involvement, level of fracture and fracture type were road traffic accidents (60%), right side (53.3%) and mid one third (75%), transverse (60%) respectively.
So, in 65% of the patients, there was no disability of arm shoulder and hand as DASH score was within normal range and in 15% of the patients the disability was mild to moderate as scoring was slightly higher than normal and in 20% the disability was severe as the DASH score could not be calculated because of non union.
Conclusion
Elastic nail fixation require very minimal soft tissue dissection and being a close reduction, the biology of the fracture is also not disturbed and the chances of nerve injury are much less and as the non union was seen in oblique and spiral fracture type hence it should be used with caution or else other alternative methods of fixation should be used.
DASH scoring, Dynamic compression plate, Intramedullary nailing
Introduction
Trauma has been the leading cause of mortality and morbidity since the beginning of mankind and is on the rise in the present age. Diaphyseal fractures of humerus accounts for 3%-5% of all fractures [1]. With increasing road traffic accidents it is likely to be more in future.
Diaphyseal fractures of the humerus could be managed by both conservative methods as well as surgically also [2]. Conservative treatment has its demerits such as prolonged limb immobilization, the need for constant co-operation, compliance and follow ups [3]. Secondly it cannot be recommended in every case like unstable fractures (spiral/long oblique), comminuted fractures, segmental fractures, pathological fractures, fractures with delayed union or nonunion. Such fractures require operative line of treatment [4-7]. Closed interlocking nailing has got the advantage of biological fixation with preservation of fracture haematoma and minimal periosteal stripping. However, it has a disadvantage of rotator cuff impingement, rotator cuff injury and restricted elbow movements [8].
Plate osteosynthesis has always been a gold standard and always given a good result for union of the bone if properly done according to principle of Open Reduction Internal Fixation (ORIF) but the complete compression is achieved as the primary union should be achieved with absolute fixation [9], but has the disadvantage of excessive periosteal stripping, large incision and increased chances of infection and iatrogenic radial nerve palsy, less secured fixation in an osteopenic bone, there may be stress raiser in primary healing in absolute fixation compared to the callus healing seen in relative fixation with an intramedullary nailing [8].
Simple humeral shaft fractures can be treated non operatively, with good results in most cases [7]. Furthermore, nonunion after conservative treatment of these fractures does occur in up to 10% of the cases and treatment of this condition can be very difficult [10].
There is growing interest in treating even simple humeral shaft fractures by Dynamic Compression (DC) plate fixation or Intramedullary (IM) nailing in order to avoid these problems and to allow earlier mobilization and rapid return to work [11]. Although, IM nailing was recently accepted as an effective method to treat humeral fractures and cases of nonunion, there was little scientific evidence to support this [12].
The elastic nail method was developed by Küntscher and the principle was 3 point fixation when introduced in the medullary canal of long bones and was first used in the fracture of long bones of lower extremities and soon became very popular method for fracture fixation of long bone and later used for diaphyseal fracture of humerus [13].
The need for anatomic reconstruction and the absolute rigidity of AO techniques, however, easily leads to extensive soft tissue dissection; iatrogenic radial nerve lesion is a common complication of plating in humeral shaft fractures [14].
Despite technical improvements of humeral IM nails and the locking mechanism, one of the common complication noted was the shoulder joint impingement and stiffness and the common complication associated with DC plating was the extensive muscle dissection necrosis and non union, cortical bone necrosis and iatrogenic radial nerve palsy [15]. Even after so many technical improvement the treatment for humeral fracture fixation is still controversial. One of the recent implant technique being surgical correction of fracture is by titanium elastic nails. The principle of fixation is same as the earliest elastic nail. Titanium elastic nailing is done by closed reduction and internal fixation. Titanium elastic nailing is mainly used for the fractures in children.
Disabilities of the Arm Shoulder and Hand (DASH) scoring are a self-rated questionnaire which is a measure of upper-extremity disability and symptoms. The DASH is scored in two components: the disability/symptom questions (30 items, scored 1-5) and the optional module includes high performance sport/music/work section (4 items, scored 1-5). The scoring varies from 0-100. A higher score indicates more disability [16]. The aim of this study was to evaluate the functional outcome of titanium elastic nailing in the diaphyseal fractures of humerus in the adult age group and the outcome to be evaluated using DASH score.
Materials and Methods
It was a prospective study of 20 cases of diaphyseal fracture of humerus admitted to Era’s Lucknow Medical College and Hospital, Uttar Pradesh, India, between October 2014 and September 2015. After informed consent and clearance from the Ethical Committee of our Institute, 20 patients with age group of 18-60 years with isolated close fracture of shaft humerus presenting to our outpatient department and emergency department were included in the study. Patients with open fracture of shaft humerus, polytrauma patients, patient not willing for surgery and patient with other injuries of the same limb were excluded from the study. Out of the total 20 patients, there were 17 males and three females. All patients were treated with closed reduction and internal fixation with titanium elastic nail. Titanium elastic nails can be inserted in antegrade fashion with the entry point at the proximal part of the humerus and retrograde fashion with entry point at the distal end of the humerus. In our study we have used the retrograde method of insertion in the humeral shaft. Follow up was done at 1 week, 3 weeks, 3 months and 6 months and were assessed clinically for pain and range of motion and radiologically to look for bony union. At the last follow up DASH questionnaire were given to the patients and score of individual patients were calculated and then this data was statistically analysed to produce the results of the study. The data was processed with SPSS software version 16.0 (Chicago, inc. USA) and it was summarized in proportion and percentage.
Results
Out of the total 20 patients, youngest patient was 19-year-old and eldest was 57 years. Majority of patients were between 21 to 50 years of age group [Table/Fig-1]. The level of fracture in 85% (17) patients was middle one third and then in 15% (3) upper one third [Table/Fig-2]. Transverse fracture pattern was the most common fracture pattern and 60% (12) of the patients had this fracture pattern [Table/Fig-3]. Majority of fracture (50%) united in 10-16 week followed by 25% in 16-20 week and 5% in 20-24 week and remaining 20% had nonunion and all of them were having spiral and oblique fracture patterns [Table/Fig-4], for which re-surgery was done as implant removal and open reduction internal fixation with dynamic compression plating after freshening the fracture ends along with bone graft. The DASH scoring was calculated for all the patient after the fracture was clinically united as after serial questionnaire and the score was found to be in the range of 21-30 in 40% (8) of the patients followed by 10-20 in 25% (5) 51-60 in 10% (2) and between 31-40 in 5% (1) of the cases [Table/Fig-5]. Superficial infection near the entry site was present in 2 (10%) patients [Table/Fig-6]. DASH scoring was in the range of 10-30 in 13 (65%) of the patients interpreted as no disability. The DASH score was not calculated in the 20% of the cases who were declared as non union after appropriate clinical and radiological studies [Table/Fig-7].
Age distribution of patients.
| Age Group (Years) | No of Patients | % |
|---|
| 18-20 | 2 | 10 |
| 21-30 | 5 | 25 |
| 31-40 | 5 | 25 |
| 41-50 | 6 | 30 |
| 51-60 | 2 | 10 |
| Total | 20 | 100 |
| Anatomical Level | No of Patients | % |
|---|
| Upper Third | 3 | 15 |
| Top Third | 17 | 85 |
| Lower Third | -- | 00 |
| Total | 20 | 100 |
| Type of Fracture | No of Patients | % |
|---|
| Transverse | 12 | 60 |
| Oblique | 3 | 15 |
| Spiral | 2 | 10 |
| Segmental | -- | |
| Comminuted | 3 | 15 |
| Total | 20 | 100 |
Average time taken for union.
| Time of Week | No of Patients | % |
|---|
| Less Than 10 Weeks | -- | -- |
| 10 – 16 | 10 | 50 |
| 16 – 20 | 5 | 25 |
| 20 – 24 | 1 | 5 |
| 24 – 30 | -- | -- |
| 30 – 36 | -- | -- |
| Total | 16 | 80 |
Functional assessment of arm shoulder and hand (DASH score).
| DASH Score | No of Patients | % |
|---|
| 10-20 | 5 | 25 |
| 21-30 | 8 | 40 |
| 31-40 | 1 | 5 |
| 41-50 | -- | -- |
| 51-60 | 2 | 10 |
| 61-70 | -- | -- |
| 71-80 | -- | -- |
| 81-90 | -- | -- |
| 91-100 | -- | -- |
Complications observed in study.
| Complication | No of Cases | % |
|---|
| Infection– Superficial | 2 | 10 |
| Infection – Deep | - | - |
| Nonunion | 4 | 20 |
| Implant Failure | 1 | 5 |
| Delayed Union | - | - |
| Iatrogenic Radial Nerve Palsy | - | - |
| Elbow Stiffness | 2 | 10 |
Interpretation of DASH score.
| No of Patients | % | DASH Score Range | Level of Disability |
|---|
| 13 | 65 | 10-30 | No disability |
| 3 | 15 | 31-60 | Mild to moderate disability |
| 4 | 20 | Could not be calculated | Severe disability |
Discussion
The management of diaphyseal fractures of humerus has always been a problem as these fractures are associated with complications like non union, malunion, delayed union and shortening. Surgical intervention is done in these cases to achieve length and alignment with active joint mobility during the treatment to avoid stiffness of the proximal and distal joint. The classical method of treatment of humerus shaft fracture has been the use of U plaster cast. Though satisfactory result can be obtained with this method but residual angulation, malrotation, joint stiffness and limb length inequality are well documented [17].
Operative treatment should be considered in cases where principle of early mobilization is being followed to avoid complications such as malunion, delayed union, control rotational instability, shoulder and elbow stiffness, limb length discrepancies and poor compliance. The aim of this biological, minimally invasive fracture treatment is to achieve a level of reduction and stabilization that is appropriate to the age of the patient [8].
The biomechanical principal of the titanium elastic nail is based on the symmetrical bracing action of two elastic nails inserted into the metaphysis, each of which bears against the inner bone at three points which provides axial, translational and rotational stability which are essential for optimal result.
This study was done to determine the efficacy of internal fixation of titanium elastic nail in treatment of fracture shaft of humerus. The titanium elastic nails can be inserted in humerus either in antegrade or retrograde manner. In antegrade method the entry point is proximal and lateral part of humerus just inferior to insertion of deltoid muscle and in retrograde manner; nail can be inserted via lateral and medial entry portals at the distal end of humerus [18]. Two nail can be inserted with lateral portals with entry point one at 1.5 cm superior and posterior to lateral epicondyle and another at 1.5 cm superior and posterior to the first entry point with nail either C or S shape configuration or two nail can be inserted with one at lateral first entry point and other from the medial side with entry point at 1.5 cm superior and posterior to medial epicondyle. But the lateral entry for two nails is more preferred over lateral and medial entry to prevent ulnar nerve injury. However, a medial and lateral entry point provides more stability but caution should be taken and should be done only after ulnar nerve exploration by a small incision.
In our study, superficial infection around the entry was noted in two patients while signs of deep infection were not noted in any patient. Nonunion of humeral shaft fractures is defined as a fracture with no evidence of healing six weeks after the injury. Non-union has been reported in 8% to 12% of cases of fractures of humeral shaft [19]. The effectiveness of flexible nailing as a treatment modality for the treatment of humeral shaft fracture has been assessed by many studies [20-22].
Most of these studies have used ender’s nail as a method of nailing. Hall RF et al., done a prospective study with ender’s nail in 89 patients with humeral shaft fracture and the outcome was measured by union time and the frequency of the complications. Average time of union was 7.2 weeks [23]. Healing rate was high and nonunion was reported in only one patient. Zatti G et al., favoured the use of flexible nailing because patients treated with plate osteosynthesis and flexible nailing have no difference regarding time to union of these fractures (11 weeks) [22].
Shazar N et al., performed a retrospective review of 94 patients treated with ender’s nailing. The average duration of follow up was 71 weeks. In 91.5% of the patients union occurred without any additional intervention and the functional result was good in 74% of the patients [24].
In our study, 80% (16) fractures out of our 20 cases united [Table/Fig-8,9,10 and 11], with 20% (4) cases gone into non union while Bell MJ et al., reported 97% union rate with plating in which out of 34 patients 33 cases united [25]. Out of 20 patients in our study, 15 patients had good range of movements at shoulder and elbow joint, whereas in other studies like Bell MJ et al., out of 34 cases 33 (97%) had got good range of mobility at the shoulder and elbow joint.
Preoperative X-ray anteroposterior and lateral view showing transverse fracture of mid shaft humerus.
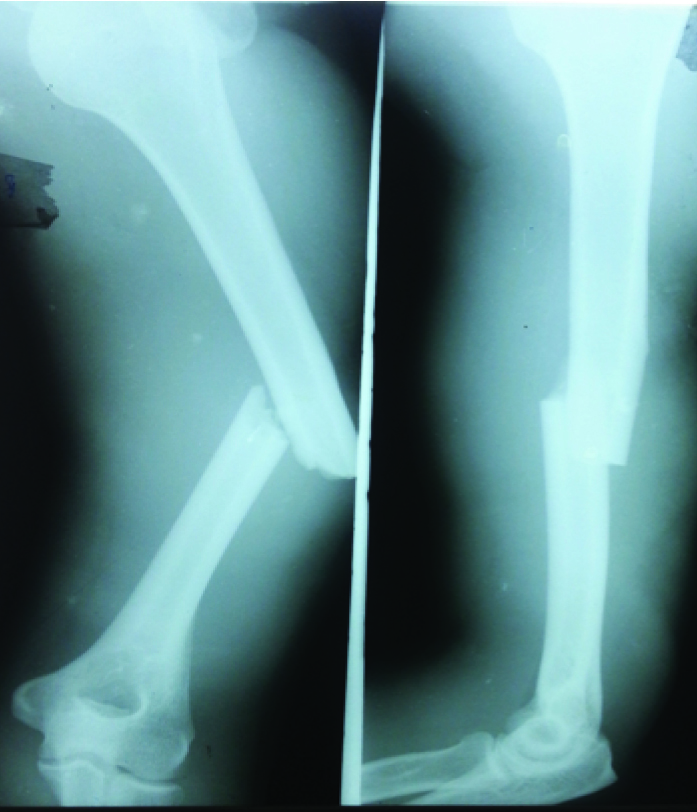
Immediate postoperative X-ray after close reduction and internal fixation with titanium elastic nail system.
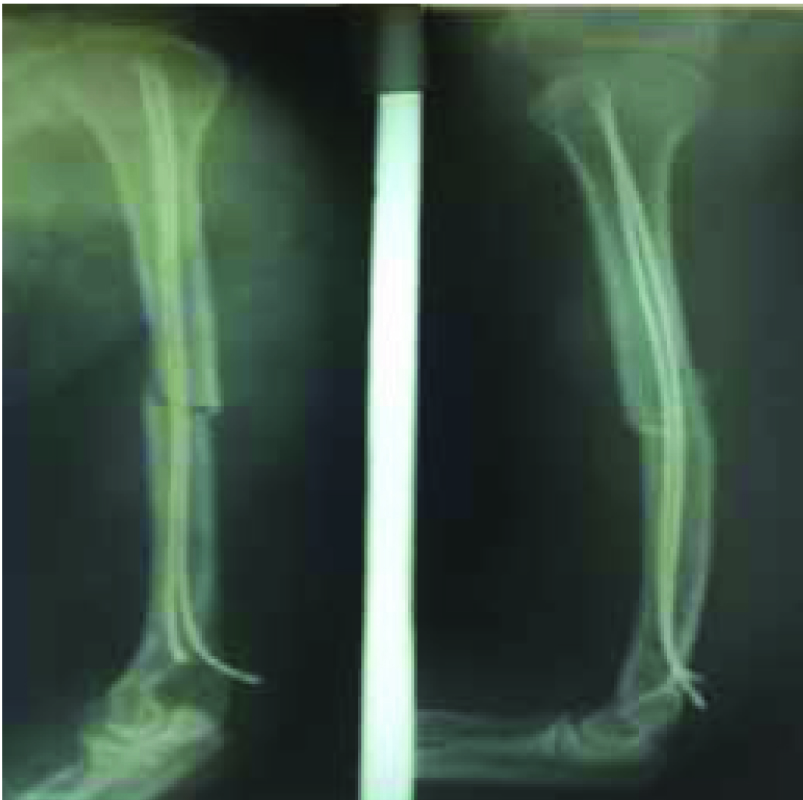
Follow up X-ray at 12 weeks showing callus formation at fracture site.

Follow up X-ray at one year showing complete union.

The result obtained by various authors using different modalities of treatment has varied from 75%-100% of good or excellent result [Table/Fig-12] [26-28]. In our study 65% of the patients, had no disability of arm, shoulder and hand as the scoring was within normal range and in 15% of the patients the disability was mild to moderate as scoring was slightly higher than normal. In 20% the disability was severe as the DASH score could not be calculated because of non union.
Overall results obtained in various studies (DCP-dynamic compression plate, IMILN-inter locking intramedullary nailing) [26-28].
| Study | Year | No of patients | Method of treatment | Excellent result (%) |
|---|
| Kuppa Srinivas et al., [26] | 2015 | 25 | DCP | 88% |
| Pal JN et al., [27] | 2015 | 66 | Functional brace | 90% |
| S Rawa et al., [28] | 2009 | 25 | IMILN | 68% |
| Present study | 2015 | 20 | Titanium elastic nail | 80% |
So, as total 80% of the patients had functional score either normal or slightly higher than the normal they could be considered to have excellent to good result in our study.
Limitation
In our study the sample size was small and so, to draw a definite conclusion a study with a larger sample size and longer duration of follow up is needed. Furthermore, DASH scoring is a measure of disability of the upper extremity. It is not a specific scoring for the arm only. So, there may be other factors like pathology of shoulder and wrist which may affect the scoring.
Conclusion
Titanium elastic nail system is a good alternative for treatment of diaphyseal fractures of humerus in adult age group as it requires minimum invasive approach, can achieve union without disturbing the biology of fracture site, and reduce the chances to almost none of iatrogenic radial nerve injury but selection of the fracture type should initially be taken into consideration.
[1]. Sahu RL, Ranjan R, Lal A, Fracture union in closed interlocking nail in humeral shaft fracturesChin Med J 2015 128(11):1428-32. [Google Scholar]
[2]. Sharma V, Awasthi B, Mehta SM, Yadav RS, Babhulkar S, Evaluation of results of different treatment modalities in management of diaphyseal fractures of humerusIndian Journal of Clinical Practice 2014 24(11):1068-74. [Google Scholar]
[3]. Clement ND, Management of humeral shaft fractures;non-operative versus operativeArch Trauma Res 2015 4(2):e28013 [Google Scholar]
[4]. Mulier T, Seligson D, Sioen Bergh JV, Reynaert P, Operative treatment of humeral shaft fracturesActa Orthopaedica Belgica 1997 63(3):170-77. [Google Scholar]
[5]. Foster RJ, Dixon GL, JrBach AW, Appleyard RW, Green TM, Internal fixation of fractures and non-unions of the humeral shaft. Indications and results in a multi-center studyJ Bone Joint Surg Am 1985 67(6):857-64. [Google Scholar]
[6]. Klenerman L, Fractures of the shaft of the humerusJ Bone Joint Surg Br 1966 48(1):105-11. [Google Scholar]
[7]. Sarmiento A, Waddell JP, Latta LL, Diaphyseal humeral fractures: Treatment optionsInstr Course Lect 2002 51:257-69. [Google Scholar]
[8]. Gupta SK, Kumar MK, K. Reddy R, Guru Prasad SS, Gopichand K, Comparative study of management of humeral diaphyseal fractures by DCP plate and IMIL nailJournal of Evolution of Medical and Dental Sciences 2014 17(7):1782-88. [Google Scholar]
[9]. Uhthoff HK, Poitras P, Backman DS, Internal plate fixation of fractures: short history and recent developmentsJournal of Orthopaedic Science 2006 11(2):118-26. [Google Scholar]
[10]. Healy WL, White GM, Mick CA, Nonunion of the humeral shaftClin Orthop 1987 219:206-13. [Google Scholar]
[11]. Wali MGR, Baba AN, Latoo IA, Bhat NA, Baba OK, Sharma S, Internal fixation of shaft humerus fractures by dynamic compression plate or interlocking intramedullary nail: a prospective, randomised studyStrategies in Trauma and Limb Reconstruction 2014 9(3):133-40. [Google Scholar]
[12]. Kivi MM, Soleymanha M, Haghparast-Ghadim-Limudahi Z, Treatment outcome of intramedullary fixation with a locked rigid nail in humeral shaft fracturesArchives of Bone and Joint Surgery 2016 4(1):47-51. [Google Scholar]
[13]. Bong MR, Koval KJ, Egol KA, The history of intramedullary nailingBulletin of the NYU Hospital for Joint Diseases 2006 64(3 and 4):94-97. [Google Scholar]
[14]. Wang JP, Shen WJ, Chen WM, Huang CK, Shen YS, Chen TH, Iatrogenic radial nerve palsy after operative management of humeral shaft fracturesJ Trauma 2009 66(3):800-03. [Google Scholar]
[15]. Zhao J-G, Wang J, Wang C, Kan S-L, Kellam JF, Intramedullary nail versus plate fixation for humeral shaft fractures: a systematic review of overlapping meta-analysesMedicine 2015 94(11):e599 [Google Scholar]
[16]. Atroshi I, Gummesson C, Andersson B, Dahlgren E, Johansson A, The disabilities of the arm, shoulder and hand (DASH) outcome questionnaire: reliability and validity of the Swedish version evaluated in 176 patientsActa Orthopaedica Scandinavica 2000 71(6):613-18. [Google Scholar]
[17]. Jaiswal A, Pruthi KK, Goyal RK, Singh VP, Stack nailing for management of diaphyseal fractures of humerus: analysis of 65 casesInternational Journal of Contemporary Medical Research 2016 3(9):2526-30. [Google Scholar]
[18]. Garnavos C, Diaphyseal humeral fractures and intramedullary nailing: Can we improve outcomes?Indian Journal of Orthopaedics 2011 45(3):208-15. [Google Scholar]
[19]. Hierholzer C, Sama D, Toro JB, Peterson M, Helfet DL, Plate fixation of ununited humeral shaft fractures: effect of type of bone graft on healingJ Bone Joint Surg Am 2006 88(7):1442-47. [Google Scholar]
[20]. Matityahu A, Eglseder WA, JrLocking flexible nails for diaphyseal humeral fractures in the multiply injured patient: a preliminary studyTech Hand Up Extrem Surg 2011 15(3):172-76. [Google Scholar]
[21]. Stannard JP, Harris HW, McGwin G, JrVolgas DA, Alonso JE, Intramedullary nailing of humeral shaft fractures with a locking flexible nailJ Bone Joint Surg Am 2003 85(11):2103-10. [Google Scholar]
[22]. Zatti G, Teli M, Ferrario A, Cherubino P, Treatment of closed humeral shaft fractures with intramedullary elastic nailsJ Trauma 1998 45(6):1046-1050. [Google Scholar]
[23]. Hall RF, Pankovich AM, Ender nailing of acute fractures of the humerus. A study of closed fixation by intramedullary nails without reamingJ Bone Joint Surg Am 1987 69(4):558-67. [Google Scholar]
[24]. Shazar N, Brumback RJ, Vanco B, Treatment of humeral fractures by closed reduction and retrograde intramedullary Ender nailsOrthopedics 1998 21(6):641-46. [Google Scholar]
[25]. Bell MJ, Beauchamp CG, Kellan JK, The result of plating of humerus shaft fracture in patients with multiple injuriesJ Bone joint Surg (Br) 1985 67(2):293-96. [Google Scholar]
[26]. Srinivas K, Rajaiah D, Ramana Y, Omkaram S, Venkateswar Reddy S, A study of surgical management of diaphyseal fractures of humerus by dynamic compression plate osteosynthesisJournal of Evolution of Medical and Dental Sciences 2015 4(8):1290-96. [Google Scholar]
[27]. Pal JN, Biswas P, Roy A, Hazra S, Mahato S, Outcome of humeral shaft fractures treated by functional cast braceIndian Journal of Orthopaedics 2015 49(4):408-17. [Google Scholar]
[28]. Rawa S, Farooq M, Singh S, Wani M, Bhat M, Hussain A, Results of antegrade humeral interlocking nailing in adults–a prospective studyThe Internet Journal of Surgery 2009 24(2) [Google Scholar]