Light Microscopic Features of Type II Dens Invaginatus in A Deciduous Mandibular Molar
Deepak Pandiar1, C Vijayalakshmi2, Amit Kumar3, Shameena Pallikandi Maliyekkal4, Manjusha Pattamparambath5
1 Phd Scholar, Department of Oral Pathology and Microbiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
2 Senior Resident, Department of Oral Pathology and Microbiology, Government Dental College, Kottayam, Kerala, India.
3 Ex-Resident, Department of Oral Pathology and Microbiology, Government Dental College, Calicut, Kerala, India.
4 HOD and Prefessor, Department of Oral Pathology and Microbiology, Government Dental College, Allapuzha, Kerala, India.
5 Fellow in Head and Neck Pathology, Department of Pathology, Malabar Cancer Center, Thalassery, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepak Pandiar, Faculty of Dental Sciences, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005, Uttar Pradesh, India.
E-mail: deepakpandiar1923@yahoo.com
Bulbous, Developmental anomaly, Histology, Parazones, Spindles
Dens invaginatus (Dens-in-dente/DI) is a rare developmental anomaly characterized by invagination of calcified tissues into the pulp which is lined by enamel [1]. The purpose of this paper is to present histological features of Type II DI in an undemineralized deciduous mandibular molar.
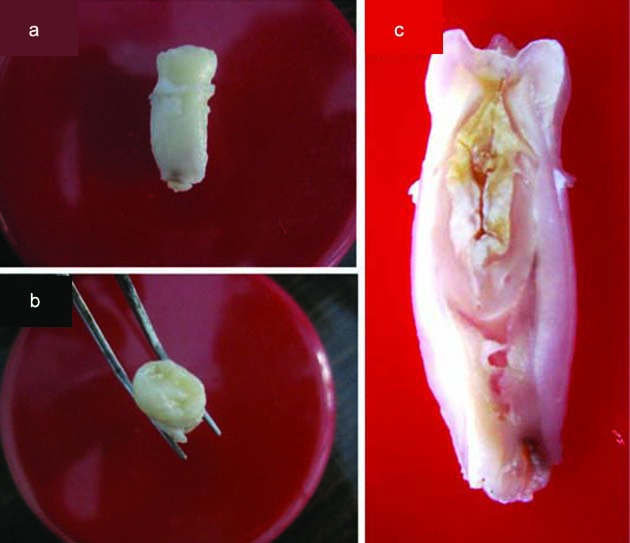
A 13-year-old female patient reported to the Department of Oral Medicine with a complaint of abnormally erupting tooth in the back tooth region of the lower jaw on the right side. On examination, the right mandibular permanent first premolar was seen erupting lingually to its predecessor which was immobile and sound. Keeping in mind the chronological order of eruption it was decided to extract the deciduous right first molar to provide space for the erupting tooth. The tooth was extracted under local anesthesia in Oral Surgery Department on the same day and the patient was discharged off. Unexpectedly the extracted tooth consisted of single large bulbous root. The apex of the extracted tooth appeared incompletely formed [Table/Fig-1a-c]. The tooth was sent to Oral Pathology Unit for histological examination where a ground section was prepared and mounted in Dibutylphthalate Polystyrene Xylene (DPX).
a,b) Extracted specimen and c) cut section.
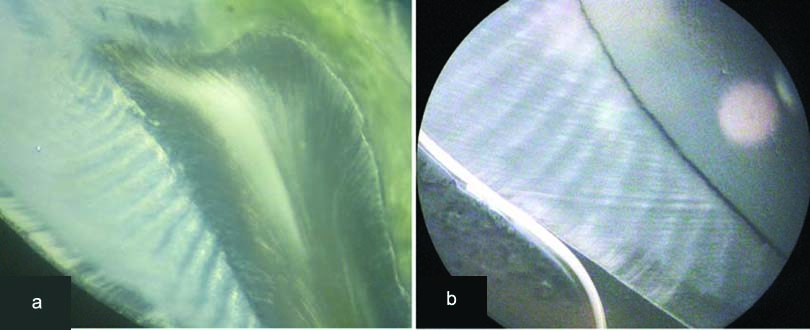
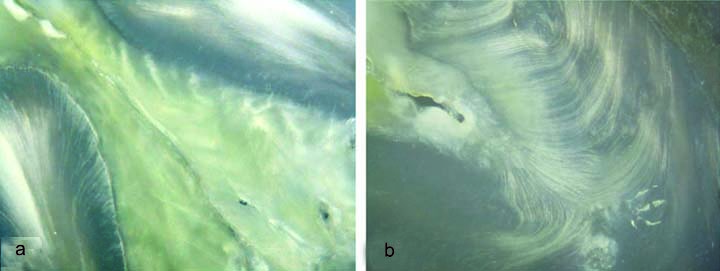
The conventional transmitted light microscopy revealed histological features consistent with DI (Type II). The Outer Enamel (OE) appeared normal and showed the presence of lamellae, tufts, spindles and striae of Retzius with an accentuated appearance [Table/Fig-2]. Under reflected light, Hunter Schreger Bands (HSBs) were seen which showed thicker parazones as compared to diazones originating at an angle from Dentino-Enamel Junction (DEJ) to approximately half of the thickness of enamel [Table/Fig-3a]. [Table/Fig-3b] shows HSBs of a normal tooth for comparison. The OE towards the invagination was irregular but well formed with a deep fissure extended into Invaginated Enamel (IE) (clinically no pit was appreciated in the extracted tooth specimen). A sharp line of demarcation was seen between OE and IE. Invaginated enamel was vase shaped [Table/Fig-4] and showed marked differences in characteristics from OE [Table/Fig-5]. It was amorphous, homogeneous and aprismatic with few haphazard irregularities, reminiscent of enamel lamellae, originating from a straighter DEJ [Table/Fig-6]. For most of the parts DEJ lacked normal scalloping but at some areas, the junction was seen as multilayered fish scale like pattern [Table/Fig-7]. Under reflected light, IE showed a light brownish hue with short crisscross light and dark bands towards DEJ [Table/Fig-8a]. The dentin showed S shaped dentinal tubules in most of the areas except at the base of IE where the dentinal tubules showed marked irregularities and dentin formation appeared to occur around obstacles resembling ‘lava flowing around boulders’ like pattern characteristic of dentin dysplasia [Table/Fig-8b]. The enamel especially at the base of IE appeared more hypomineralized [Table/Fig-9]. No communicating channels were seen between pulp and enamel howbeit few remnants of pulp tissues were seen within IE. Pulp appeared normal [Table/Fig-10a]. The outer surface was covered by a thin layer of cementum [Table/Fig-10b].
Photomicrograph of ground section showing outer normal appearing enamel (100X).
a) HSBs in present case under reflected light; b) Compare with HSBs of a normal specimen (100X).
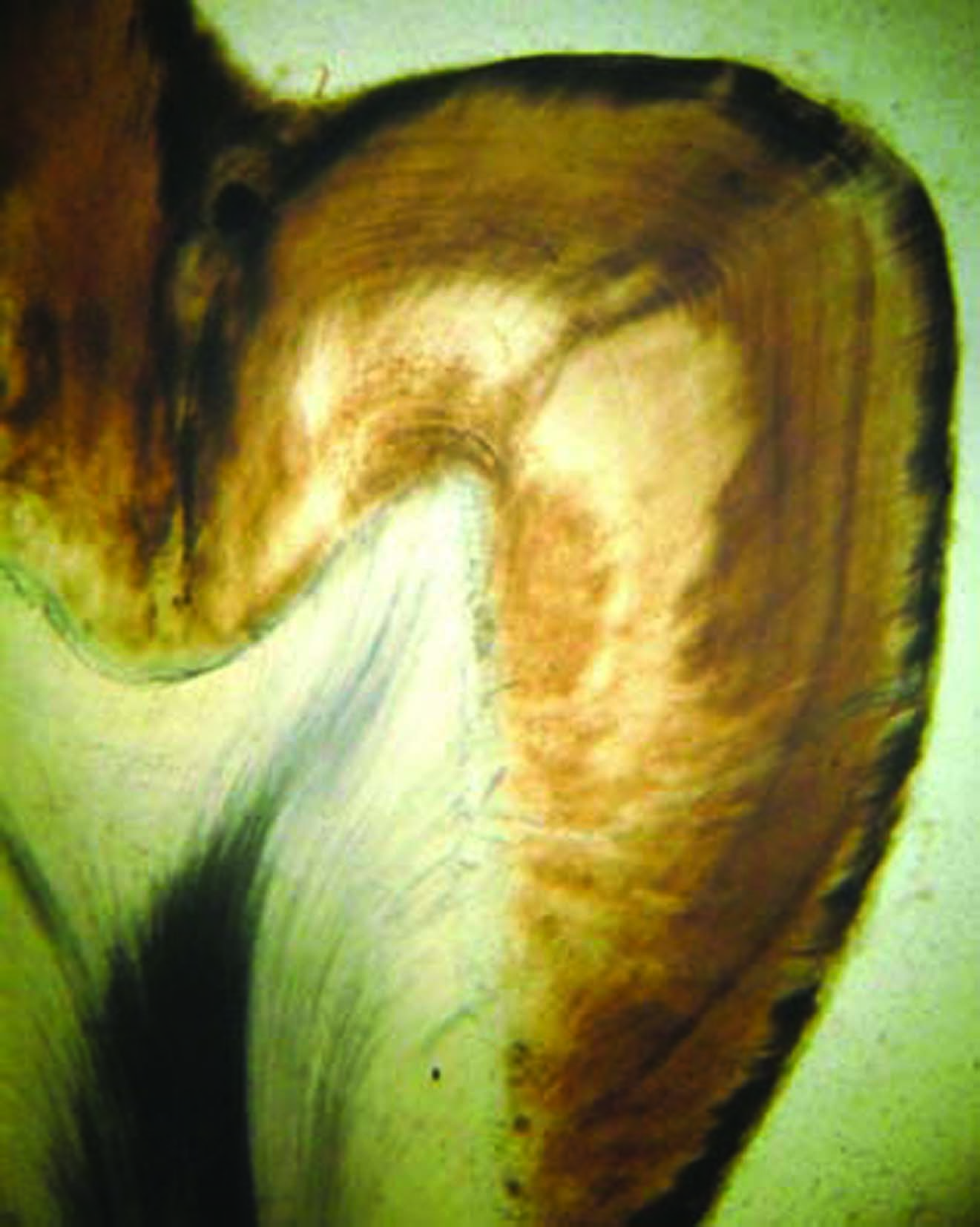
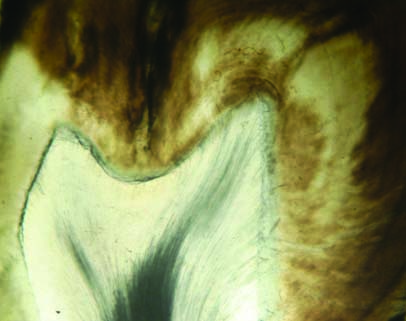
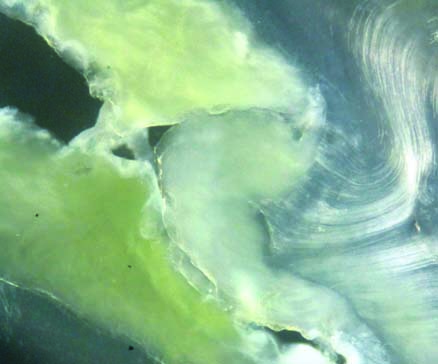
Mounted specimen showing vase shaped invagination of enamel.

Ground section showing the area of invagination. Note a deep fissure extending into invaginated enamel and well demarcated zone between IE and OE (100X).

Ground section showing straight DEJ between IE and dentin. IE is amorphous and aprismatic. Few remnants of pulp tissue are also seen. (100X).

Multiple fish scale DEJ between OE and dentin (100X).
a) IE under reflected light and b) disorganized dentinal tubules with dentin dysplasia like features (100X).
More hypomineralized IE especially at the base invagination (100X).
a) Pulp tissue in canal and b) thin cellular cementum covering root; c-e) OE and IE under polarized light (100X).
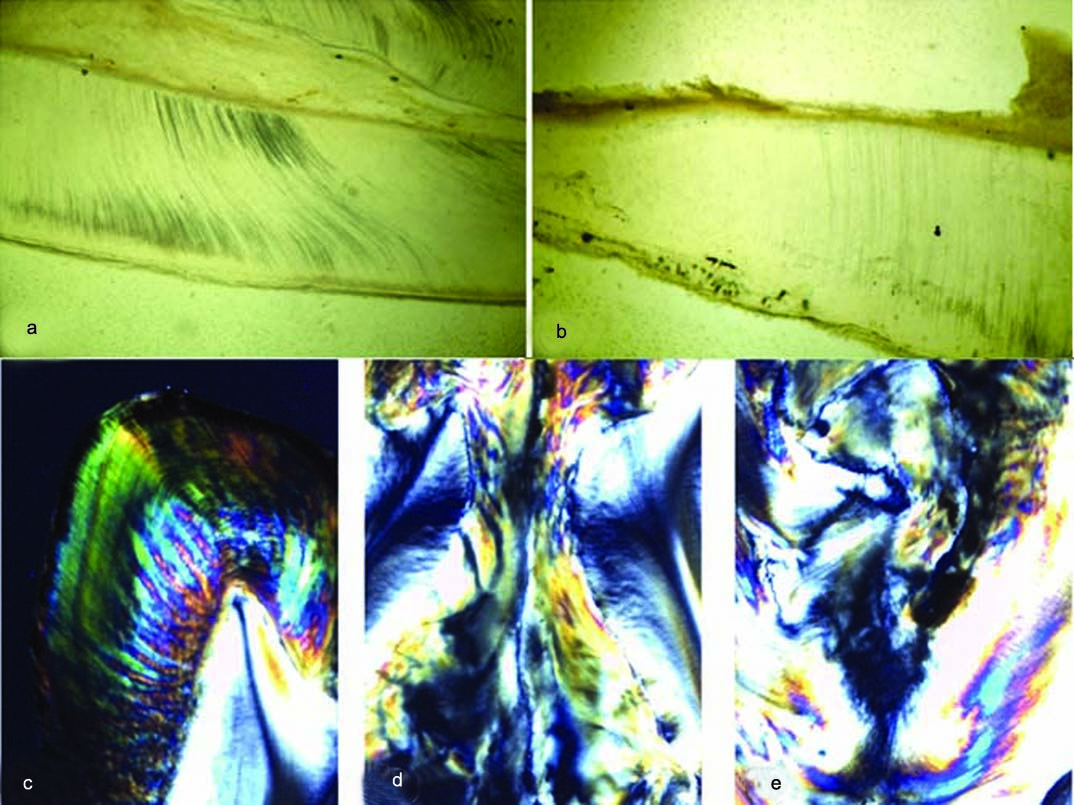
Under polarizing light all the aforementioned features were more accentuated. The OE showed a well demarcated surface layer that lacked normal prismatic appearance. The area of invagination showed that IE was totally ill formed lacking normal striae of Retzius. The crisscross bands reminiscent of HSBs were more clearly depicted. The deep fissure was also clearer on polarizing light [Table/Fig-10c-e). Thus, in the present case it was noticed that the features described under transmitted and reflected light appeared more accentuated under polarizing light.
This case shows unique features like uneven HSBs in OE, crisscross pattern of HSBs in IE, multilayered fish scale like DEJ and a dentin dyplasia like pattern at the base of IE. Multilayered fish scale like DEJ has been previously reported by Mishra S et al., [2]. Catin M and Fonseca GM presented a morphological study of impacted mesiodens in a nine-year-old girl using cone beam CT and explained histological features not distinctive from the present case [3].
In conclusion, DI at times goes undiagnosed because the condition may sometimes be asymptomatic with minimal discomfort to the patient. Thus, the extracted specimen should be submitted for histological examination that may present features unexplained so far.
[1]. Oehlers FA, Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown formsOral Surg Oral Med Oral Pathol 1957 10:1204-18. [Google Scholar]
[2]. Mishra S, Mishra L, Sahoo SR, A Type III dens invaginatus with unusual helical CT and histologic findings: a case reportJ Clin Diagn Res 2012 6(9):1606-09. [Google Scholar]
[3]. Cantín M, Fonseca GM, Dens invaginatus in an impacted mesiodens: a morphological studyRom J Morphol Embryol 2013 54(3 Suppl):879-84. [Google Scholar]