Quality Assessment of Family Planning Sterilization Services at Health Care Facilities: Case Record Audit
Medha Mathur1, Ram Chandra Goyal2, Navgeet Mathur3
1 Senior Resident, Department of Community Medicine and Family Medicine, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
2 Principal, Department of Preventive and Social Medicine, Rural Medical College, Pravara Institute of Medical Sciences (DU), Loni, Maharashtra, India.
3 Senior Resident, Department of General Medicine, Dr. S.N. Medical College, Jodhpur, Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Medha Mathur, 306, PG Hostel, AIIMS, Jodhpur, Rajasthan, India.
E-mail: drmedhamathur@yahoo.co.in
Introduction
Quality of sterilization services is a matter of concern in India because population control is a necessity. Family Planning Sterilization (FPS) services provided at public health care facilities need to be as per Standard Operating Procedures.
Aim
To assess the quality of FPS services by audit of case records at selected health care facilities.
Materials and Methods
This cross-sectional study was conducted for two and a half year duration at selected public health care facilities of central India by simple random sampling where FPS services were provided. As per the standards of Government of India, case records were audited and compliance was calculated to assess the quality of services.
Results
Results of record audit were satisfactory but important criteria like previous contraceptive history and postoperative counselling were found to be deviated from standards. At Primary Health Centres (PHCs) only 89.5% and at Community Health Centres (CHCs) 58.7% of records were having details of previous contraceptive history. Other criteria like mental illness (only 70% at CHCs) assessment were also inadequate. Although informed consent was found to be having 100% compliance in all records.
Conclusion
Quality of care in FPS services is the matter of concern in present scenario for better quality of services. This study may enlighten the policy makers regarding improvements needed for providing quality care.
Case history, Population control, Survey
Introduction
India is the second most populous country in the world. Since ages, population control is a matter of concern in Indian subcontinent. Literature shows that birth control clinics were functioning in the country since 1930. In 1952 the Government of India formulated national family planning program which was the first in world. Initially, program was modest with establishment of few clinics and distribution of educational material, training and research. In the year 1997, the Reproductive and Child Health (RCH) programme was launched which espouses the principles of client satisfaction in delivering comprehensive and integrated high quality health services [1]. Under the National Rural Health Mission (NRHM) and Reproductive and Child Health II (RCH II) programmes (2005) launched by Government of India many strategies were being operationalized to reduce the unmet need in RCH services including contraception [2]. Camp approach was required to fulfil the demand of FPS services, but standards maintained during camps were still questionable and quality of sterilization services was a matter of concern [2].
Quality of care in public health care system, with special stress on improvement of family planning services will result in more satisfied clientele [3]. Quality assurance is defined as process that contributes to defining, designing, assessing, monitoring and improving the quality of healthcare. It is a comprehensive and multifaceted concept that measures how well clients’ expectations as well as providers’ technical standards are being met [1]. The quality assurance programme has two main components, namely quality assessment and quality improvement.
To measure the quality of health services, three dimensions of quality assessment are required using a system approach in the form of input, process and outcome. Quality of family planning services may lead to fertility reduction, which as a result leads to meet the demographic objectives.
Improvements in quality of family planning services by enhancing the choice of contraceptive methods available in a country would increase the overall practice of contraception [4].
In order to provide quality care, FPS services provided at public health care facilities should be as per the Standard Operating Procedures. In 2008, ‘Quality Assurance for District Reproductive and Child Health Services in Public Health System: An Operational Manual’ was published by Ministry of Health and Family Welfare, Government of India, New Delhi [5]. This document basically suggested Standard Operating Procedures for providing FPS services for females and males and health facilities to improve the quality of services by standardizing the services. Rural areas need to have services of good quality for sterilization because it was found that rural women had higher unmet need than urban women for both spacing and limiting, which is reflected by higher fertility rate in rural than urban areas i.e., 3.0 and 2.1 respectively.
This study was designed to assess the quality of FPS services provided in static settings by audit of client case records, which is a part of quality assessment in health care delivery system, at selected health care facilities of Wardha district.
Materials and Methods
This was a cross-sectional study, conducted for two and a half years (June 2011 to October 2013). This facility based study was conducted at selected public health care facilities of Wardha district, Maharashtra where FPS services were provided. A list of all the health facilities providing sterilization services was obtained from district health office. Wardha district has 27 PHCs, eight CHCs and one district hospital, out of which by using simple random sampling 19 health facilities were selected for this study. Selected health facilities comprised one district hospital, four CHCs and 14 PHCs. One of the PHCs had no functional operation theatre hence that particular health facility was excluded from sampling frame, without affecting the power of the study.
Strategy: Selected health facilities were visited by the principal investigator and secondary data was collected. As a part of quality assessment of FPS services, client case records were assessed by audit as mentioned in ‘An Operational Manual by Government of India’ (2008) [5]. This Operational Manual has mandated that out of the available surgical case records randomly 20 case records need to be selected by investigator and checked for complete record filling and maintenance of criteria as per standards. The facility registers and client records were reviewed to check if record keeping was done correctly and completely. For the purpose of audit a sample of randomly selected cases (20 surgical case records) were taken [5]. Criteria for client case audit included recording of marital status of the patients, number of living issues, history of previous contraceptive use, haemoglobin level, body temperature, assessment of mental illness, blood pressure measurement, method specific counselling of the patient, informed consent for the operative procedure, skin condition at surgical site, postoperative instructions to the patients and skin preparation with betadine before surgical procedure as accepted from Operational manual [5] [Table/Fig-1].
Criteria used for audit of client case records.
| Sr. No. | Criteria |
|---|
| I | Marital status of the patient |
| II | Number of live issues |
| III | Previous contraceptive history taken from patient |
| IV | Haemoglobin noted in case record |
| V | Body temperature checked |
| VI | Mental illness checked |
| VII | Blood pressure recorded |
| VIII | Method specific counselling of the patient done |
| IX | Informed consent for the operative procedure taken |
| X | Any skin condition involved at surgical site |
| XI | Postoperative instructions to the patients |
| XII | Skin preparation with betadine |
The audit criteria were numbered and criterion was counted ‘+’ if it was found to be followed positively and similarly counted ‘-’ if not followed as per standards. A criterion was considered to be out of compliance if it had less than 95 percent calculated compliance percentage.
Based on the above assumptions, percentage compliance was calculated as:

Compliance was assessed by compliance percentage calculation and quality was graded in four categories namely very good, good, poor and very poor as per the percentages obtained against standard [Table/Fig-2].
Grades for quality of services.
| Grade | Quality | Score in compliance percentages |
|---|
| A | Very good | 76% and above score |
| B | Good | 51% – 75% score |
| C | Poor | 26% – 50% |
| D | Very poor | Upto 25% score |
In general if only one criterion in 20 case records was found to be out of compliance it was not reported to health authorities for undertaking corrective measures. However, if two or more criteria were found to be out of compliance a plan for correction was suggested. Ethical approval was obtained from the institutional review board (approval number 2011-12/288).
Results
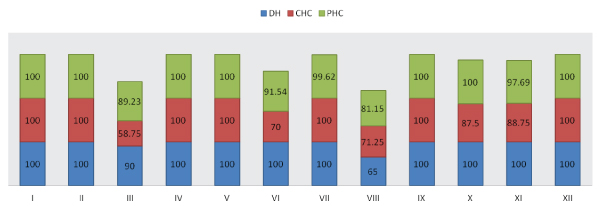
All the criteria used for client case record audit were cumulatively assessed. It was found that at district hospital only two criteria were found to be deviated namely previous contraceptive history and method specific counselling of the patients. It was observed that counselling of the patients was done in only 65% cases at district hospital.
At CHCs along with criteria III and VIII, criteria VI, X, XI were also found to be scoring low. Previous contraceptive history was ignored and not recorded properly at CHCs and assessment of mental illness (70%) was also not given due importance in case records by health workers. It was also an important observation that postoperative instructions were not imparted consistently to all the patients which may lead to poor health outcome after surgery.
At PHCs it was observed that recording of previous contraceptive history (89.2%) and assessment of mental illness (91.5%) of the patients were inadequate along with low compliance for method specific counseling (81.1%) of the patients [Table/Fig-3].
Evaluation of twelve criteria at district hospital, four CHCs and thirteen PHCs.
Amongst PHC compliance were found to be 83.3% as the lowest and maximum 100% compliance was observed at two of the PHCs. CHCs showed 76.7% as the lowest compliance for criteria while one of the CHC showed 100% compliance. At district hospital compliance was found to be 96.3% [Table/Fig-4].
Evaluation of cumulative criteria at selected health care facilities.
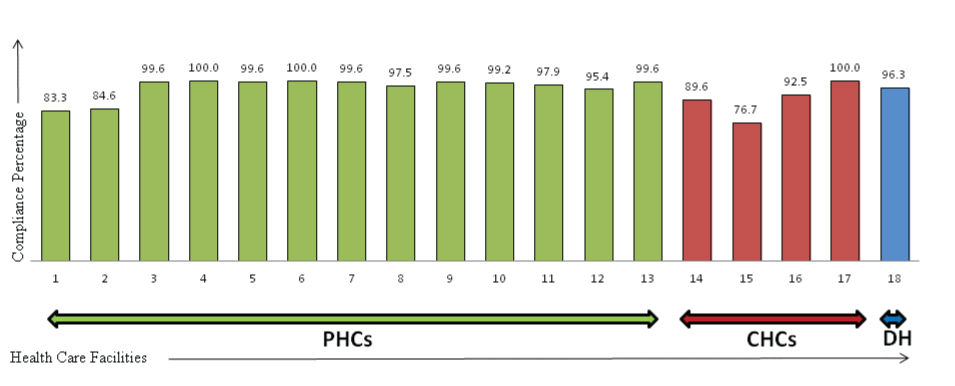
It was observed that at district hospital 92% criteria were graded ‘A’ i.e., very good and only 8% were graded as ‘B’ i.e., good. While at CHCs, 75% of criteria lied in category of very good (Grade A) and 25% were only good (Grade B). At all the 13 PHCs, all the criteria were graded ‘A’ with more than 75% compliance.
Discussion
Quality of care still needs to be addressed in Indian scenario. The present study aimed to assess quality of FPS services by audit of client case records. Although at all the health facilities client case records were present regarding sterilization services but were not adequately maintained reflecting inadequate health practices. It was found that quality of services was compromised which is clear by inadequate compliance for mental illness assessment, method specific counselling, contraceptive history of patients, observation for skin condition involvement at surgical site and postoperative counselling. Three fourth (75%) of the criteria were completed in all client audit records like marital status, number of living children, hemoglobin level, blood pressure, temperature records, informed consent and skin preparation before surgery.
Studies by Prakash RR and Pal SR et al. revealed that consent was taken by 100% subjects, similar finding was depicted by the current study [6,7]. Pal SR et al., Bijalwan R and Maithili B found that presterilization counselling was imparted to 76.2% and 12% subjects respectively while in this study 84.6% subjects received presterilization counselling [7,8]. Criterion like taking contraceptive history was not adequate at all the health facilities. Marital status and number of living children were the criteria which were adequately taken at all the health facilities but technical criteria like counselling of patients postoperatively or assessment of mental illness were inadequately done by health workers.
PHCs were found to be better performing in context of majority of criterions in comparison to CHCs. Although the reason for the poorly executed criterion could be untrained staff for record keeping but this study has not evaluated the training of record keepers which is one of the limitation of this study.
Conclusion
It can be concluded from the study that although case records were present but quality was compromised as important criteria like previous contraceptive history, method specific counselling, mental illness checkup, skin conditions involvement and postoperative counselling were missing at health facilities which is a reflection of poor quality of FPS services. It is recommended to impart formal training to health workers for the better services including record maintenance. It is recommended that policy makers prefer quality over the quantity component in family planning services and audits of record could be an effective measure for the purpose.
[1]. Division of research studies and standards. Ministry of Health & Family welfare, (GOI). Quality assurance manual for sterilization services 2006 New DelhiGovernment of India [Google Scholar]
[2]. Ministry of Health and Family Welfare, (GOI). Standard Operating Procedures for Sterilization Services in Camps 2008 New DelhiGovernment of India [Google Scholar]
[3]. Bruce J, Fundamental elements of the quality of care: A simple frameworkstudies in family planning 1990 21(2):61-91. [Google Scholar]
[4]. Jain AK, Fertility reduction & quality of family planning servicesstudies in family planning 1989 20(1):1-16. [Google Scholar]
[5]. Ministry of Health and Family Welfare, (GOI). Quality Assurance for District Reproductive and Child Health Services in Public Health System: An Operational Manual 2008 New DelhiGovernment of India [Google Scholar]
[6]. Prakash RR, “Informed Consent in Sterilisation Services: Evidence from Public and Private Health Care Institutions in Chennai” Health and Population Innovation Fellowship Programme. Working Paper. No. 4 2007 New DelhiPopulation Council [Google Scholar]
[7]. Pal SR, Singh B, Shakya S, Continuing Concerns: An Assessment of Quality of Care and Consequence of Female Sterilization in Bundi District of Rajasthan in 2009-10Centre for Health and Social Justiceaccessed on July 07 2013New DelhiAvailable at<hptt://www.chsj.org/uploads/swarup_r_pal_bajrang_singh _singh_shreeti_shakya_03_01_12.pdf> [Google Scholar]
[8]. Bijalwan R, Maithili B, Status of user's perspective on the quality family planning services and care in Doiwala block, Dehradun district of UttarakhandThe International Journal of Engineering and Science 2013 2(1):299-302. [Google Scholar]