Materials and Methods
In this retrospective study, we included those cases from whom Aeromonas spp. were isolated alone or along with another microorganism from extra intestinal sites after obtaining approval from the Institutional Ethics Committee from December 2015 to October 2016. Total 26 cases of Aeromonas were analysed retrospectively. Clinical features and the underlying co-morbid conditions were noted. Clinical samples evaluated for microbiological investigations were wound swabs (13), pus (8), tissues (8), bile (1) and corneal scrapping (1). All clinical samples were cultured on 5% sheep blood agar and MacConkey agar after Gram staining and incubated at 37°C for 18-24 hours. Isolates were further identified by Gram staining, colony characteristics, biochemical tests like oxidase test, indole test, Voges-Proskauer test, triple sugar iron test, arabinose and esculin hydrolysis test [4] and finally by Matrix Assisted Laser Desorption Ionization Time-of-Flight (MALDI-TOF) VITEK®MS. Antimicrobial susceptibility testing of the isolates was done by VITEK®2 system (bioMérieux, Inc, Durham, NC).
Polymicrobial infection was diagnosed when another microorganism isolated along with Aeromonas spp. from the same clinical specimen.
Aeromonas spp. was identified as MDR, when they were non-susceptible to ≥1 agent in ≥3 antimicrobial categories [5].
Statistical Analysis
Patient demographics, clinical characteristics, co-morbid conditions and laboratory parameters were presented as mean±standard deviation, frequency and percentage as deemed appropriate.
Results
Among the 26 patients diagnosed with Aeromonas infection, 84.6% (22/26) were male. The mean (SD) age of the patients was 41.58 (±17.86) years (range: 15-80 years). A majority of the patients had a surgical admission (53.8%) followed by orthopedics (38.5%) and medicine (3.8%). The mean (SD) hospital stay was 16.55 (±12.29) days.
Out of 26 individuals, 24 (92.3%) of them presented with SSTI at the time of admission. In 50% (12/24) patients, SSTI started after trauma to the site. The common site of infection was lower extremities (16 cases, 66.7%). Clinical presentation varied from localized infection to the severe gangrenous form. Out of 24 patients, 15 of them (62.5%) presented with gangrene of the extremities. Though 45.8% (11/24) of the patients with SSTI had underlying co-morbid conditions, none of them presented with invasive infection. Diabetes (5/24, 20.8%) was the most common underlying co-morbid condition. 54.2% (13/24) cases of SSTI were polymicrobial in nature. Organisms like Staphylococcus aureus, Citrobacter spp., E.coli and Pseudomonas aeruginosa were isolated along with Aeromonas spp. in polymicrobial infections.
Other than SSTI, 2 cases presented with cholangitis and keratitis. From both the cases A. hydrophila was isolated as a single pathogen. None of them had any underlying co-morbid conditions. Both the patients were young individuals. Patient demographics, clinical characteristics and co-morbid conditions associated with Aeromonas infections are mentioned in [Table/Fig-1].
Patient demographics, clinical characteristics and co-morbid conditions associated with Aeromonas infections.
| Character | Number of Cases (26) | Percentage |
|---|
| Age (years) |
| 10-20 | 04 | 15.4 |
| 21-40 | 09 | 34.6 |
| 41-60 | 09 | 34.6 |
| 61-80 | 04 | 15.4 |
| Gender |
| Male | 22 | 84.6 |
| Female | 04 | 15.4 |
| Preceding trauma | 12 | 46.2 |
| Clinical Presentation |
| Gangrene | 15 | 57.7 |
| Necrotizing fasciitis | 03 | 11.5 |
| Post-op wound infection | 03 | 11.5 |
| Localized wound infection | 03 | 11.5 |
| Cholangitis | 01 | 3.8 |
| Keratitis | 01 | 3.8 |
| Co-morbid conditions |
| Diabetes | 05 | 19.2 |
| Hepatic disorders | 01 | 3.8 |
| Cardiovascular disorder | 04 | 15.4 |
| Renal disorders | 01 | 3.8 |
| Type of Infection |
| Monomicrobial infection | 13 | 50 |
| Polymicrobial infection | 13 | 50 |
| Management |
| Wound debridement+ antibiotic therapy | 13 | 50 |
| Only antibiotic therapy | 4 | 15.4 |
| Amputation done | 9 | 34.6 |
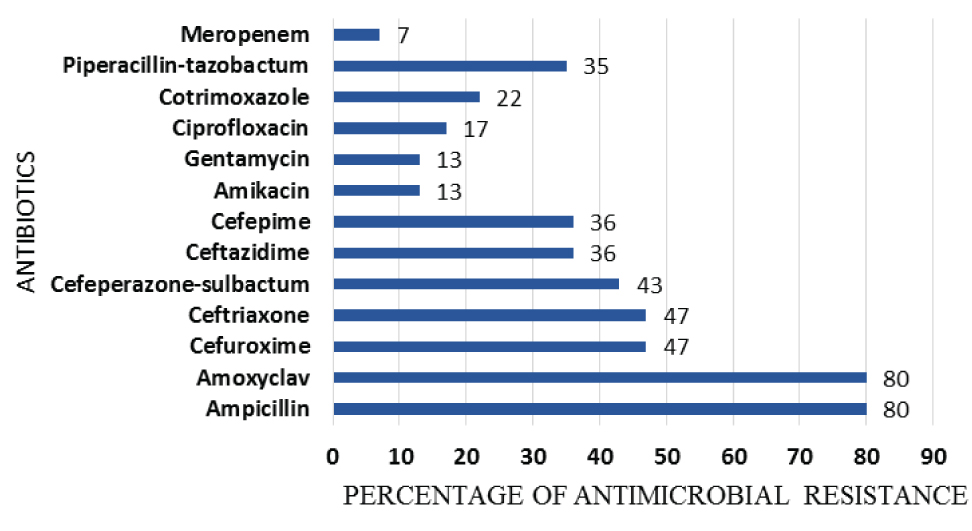
Most common isolated Aeromonas spp. was A. hydrophila (23/26, 88.5%) followed by A. sobria (11.5%). An 80% of Aeromonas were resistant to ampicillin, amoxy-clavulanic acid. Some of them even showed, resistance to second, third and even fourth generation of cephalosporin [Table/Fig-2]. A 13% of the A. hydrophila isolates were MDR. Carbapenem resistance was also noted.
Antibiotic resistant pattern of the isolated Aeromonas spp.
Discussion
Aeromonas spp. is inhabitants of fresh and brackish water and increasingly having associated with diarrheal disease [1]. They also have a significant role in the variety of extra-intestinal diseases in human. A. hydrophila, A. caviae, and A. veronii biovar sobria are responsible for more than 85% of human infections [6].
SSTI (92.3%) was the most common extra-intestinal manifestation by Aeromonas spp. in our study, similar to the other literature [7]. This infection commonly occurred in healthy young men, as reported elsewhere [8]. In 50% cases, trauma and concomitant exposure to contaminated soil (50%) had a significant role in the pathogenesis of SSTI [9]. The common site of infection was lower extremities (66.7%), also mentioned by Semel JD et al., [10]. These characteristics of the disease suggest that it is common in individuals who are more involved in outdoor activities and come in contact with contaminated soil. Mechanism of injuries involved road traffic accident (5 cases), accidental puncture wound (5 cases) and lacerated wound (2 cases). These types of injuries are more prone to contaminated soil exposure as mentioned elsewhere [11]. In the remaining 12 cases, there were underlying co-morbid conditions e.g., diabetes, hepatic disorders, renal disorders which might have predisposed the development of infection. Under these co-morbid conditions, Aeromonas can invade the blood stream [12]. But none of our cases had bacteraemia secondary to wound infection similar to earlier report by Lamy B et al., [6].
The various clinical types of SSTI are cellulitis, necrotizing fasciitis and localized wound abscess. Rarely, it progresses to severe form like myonecrosis or gangrene of the soft tissue due to production of extracellular products. But in our study, the typical clinical presentation was the gangrene of the infected tissue (15/24=62.5%) in contrast to previous report [9]. Aeromonas was found to be a sole causative agent of SSTI in 11 cases and 72.7% (8/11) of them presented with severe gangrenous form. Out of 8, one of them had diabetes. Presence of polymicrobial wound infection in 54.2% cases support the previous literature [7]. In polymicrobial infection, probably along with Aeromonas, other organisms like S. aureus, Citrobacter spp. and P. aeruginosa were also contributed to the wound pathology.
Aeromonas hydrophila (23 cases, 88.5%) were the most frequently isolated species causing SSTI infection, as mentioned by Janada JM et al., [11]. Isolation of Aeromonas sobria (11.5%) from the wound infection due to their cytotoxic activity is not very uncommon also [13]. Other than SSTI, we encountered cases of keratitis and cholangitis. In the event of keratitis, contact lens and the lens solution were the sources of infection. The isolate was sensitive to conventional ophthalmic antimicrobial agents like amoxicillin-clavulanic acid, gentamycin, ciprofloxacin and cotrimoxazole. The case was treated with topical fortified tobramycin (1.5%) and ciprofloxacin (0.3%) eye drops. Keratitis, due to the usage of contaminated contact lens is not very uncommon [14].
Post cholecystectomy, biliary tract infection by Aeromonas spp. can occur either through ascending route from the gastrointestinal tract, through hematogenous spread via portal vein or through contaminated water used at the time of operation [15]. Cholangitis was treated with a parenteral third generation cephalosporin.
Aeromonas strains are frequently resistant to penicillin, ampicillin, amoxicillin- clavulanic acid, cefazolin [16]. Eighty percent of our isolates also showed resistance towards amoxicillin-clavulanic acid and ampicillin similar to other studies due to the production of beta-lactamase enzyme [17-19].
We observed in our study, initial treatment for SSTI cases started with amoxicillin-clavulanic acid because most of the time it mimics staphylococcal or streptococcal skin infection [9]. But later in most of the cases antibiotic treatment shifted to ceftazidime along with aminoglycosides. Third generation cephalosporin e.g., ceftriaxone and piperacillin-tazobactam were used in few cases based on the antimicrobial susceptibility pattern. But we observed resistance to ceftriaxone (47%) and piperacillin-tazobactam (35%) also in our study, in contrast to the study by Zong Z et al., [20]. Fluoroquinolone resistance (17%) was similar to other study but in contrast resistance to co-trimoxazole was much less (22%) [2]. Multi drug resistance Aeromonas species have been reported globally by different authors [19,20]. Three of our A. hydrophila isolates were also MDR. They were resistant to ampicillin, amoxy-clavulanic, second, third and fourth generation cephalosporin, piperacillin-tazobactam, co-trimoxazole and ciprofloxacin. The MDR isolates were treated with carbapenem. Even carbapenem resistance was also noted in 7% cases.
Most of the SSTIs were managed by wound debridement followed by antibiotic therapy. Amputation was performed in few cases (9/26) due to severe gangrenous condition. Out of nine, three of them had diabetes also. All the cases responded clinically and microbiologically after the treatment.
Overview of various extra intestinal manifestations by Aeromonas spp. shows the necessity for routine identification of Aeromonas in the lab. The automated system along with the battery of biochemical require for their identification. Alone automated system can readily identify to the level of A.hydrophila group or A.hydrophila/A. caviae. However, these identification systems are often unable to detect interspecies differences. Phylogenetic analysis will provide a better result.
Limitation
Though we isolated Aeromonas spp. organism from different extra-intestinal sites, we could not be able to furnish several virulence factors responsible for these infections.
Conclusion
Extra-intestinal manifestations by Aeromonas spp. are not very uncommon in the coastal part of India. They were frequently isolated from post-traumatic wound site and rarely from some other sites like bile, corneal scrapping etc. The infections were treated either with a combination of surgical debridement and antimicrobial therapy with a third generation cephalosporin and aminoglycosides or only with antimicrobial therapy. We observed MDR and carbapenem resistant Aeromonas spp. also in this part of India, which is a real issue of concern.
Our study will make the clinicians more alert about this organism and their antimicrobial susceptibility pattern that will be useful for future patient management.