Lymphovascular Malformation – A Report of Two Cases
Mitakshara Sharma1, Varuna Mallya2, Nita Khurana3, Praveen Kumar4, Rajan Duggal5
1 Senior Resident, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
2 Assistant Professor, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
3 Director Professor, Department of Pathology, Maulana Azad Medical College, New Delhi, India.
4 Senior Resident, Department of Paediatric Surgery, Maulana Azad Medical College, New Delhi, India.
5 Additional Director, Department of Pathology, Fortis Escorts, Okhla, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Varuna Mallya, Assistant Professor, Department of Pathology, Room No 269, Pathology Block, Maulana Azad Medical College, New Delhi-110002, India.
E-mail: varunamallya@gmail.com
Congenital Vascular Malformations (CVM) represents a group of vascular anomalies that are the result of defective development of the vascular system. Lymphatic malformation consists of dilated lymphatic vessels caused by occlusion of the lymphatic drainage system due to congenital malformations or acquired causes such as the effects of trauma, infection, or surgery. Lymphaticovenous Malformation (LVM) is composed of lymphatic and venous channels. The most common sites are the neck and axilla. We report two cases of a four and a half-year-old and a seven-year-old child who presented with complaints of swelling in arm and groin respectively. A provisional diagnosis was made on radiological investigations. Excision was done and the diagnosis was confirmed on histopathology and immunohistochemistry. The cases which were presented as LVMs are rare congenital tumours and require a high index of suspicion on part of pathologist and surgeon to reach a definitive diagnosis.
Congenital tumours, Lymphatics, Podoplanin
Case Report
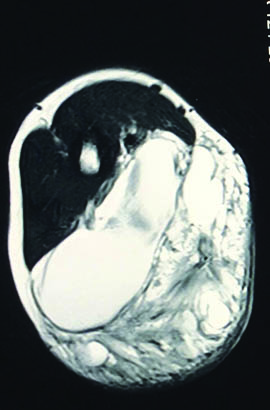
A four and a half-year-old male child presented with complaints of increase in a size of left arm swelling developed at two months of age. A seven-year-old boy presented with increase in swelling located in the groin since the age of two years. There was no history of trauma or associated infections in either case. Both the swellings were gradually increasing in size. On examination, the swellings were compressible, soft, cystic, measured 9 x 5 cm and 8 x 3 cm respectively. All the haematological investigations were within normal limits. MRI and angiography revealed multiloculated cystic lesion with no enhancement and a solid component in both cases [Table/Fig-1].
MRI showing multiloculated cystic lesion with no enhancement and a solid component in Case 1.
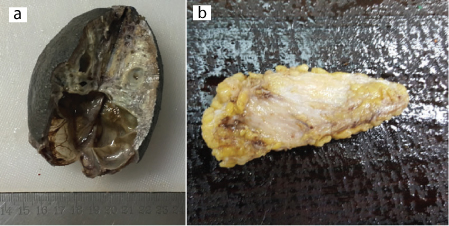
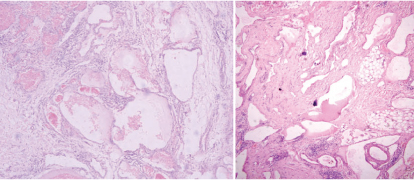
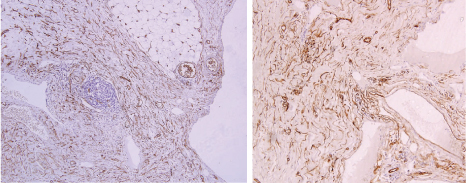
Excision was done and tissue was sent for histopathological examination. Grossly, both the swellings were skin covered soft tissues. The cut section showed multiple cystic areas ranging in size from 0.2–0.4 cm in the first case [Table/Fig-2a] and grey white areas admixed with fatty areas in the second case [Table/Fig-2b]. Microscopically, both the cases showed similar picture, there were numerous thin walled channels, filled with blood and pale eosinophilic secretions suggestive of vascular and lymphatic channels respectively showing anastomosis [Table/Fig-3a,b]. The intervening stroma showed lymphoid follicles. Findings were consistent with lymphovascular malformation. Immunohistochemistry was done and both the endothelial and the lymphatic channels were positive for CD31 [Table/Fig-4a,b], whereas only the lymphatic channels were positive for D2-40 [Table/Fig-5a,b].
(a) Gross image showing a solid cystic lesion in Case 1; (b) Gross image showing grey white areas admixed with fatty areas in Case 2. (All Image left to right)
(a) Photomicrograph of case 1 showing thin walled endothelium lined vessels. The stroma shows lymphoid aggregates. (H&E, 10X); (b) Photomicrograph of case 2 revealing lymphaticovenous anastamosis. The intervening stroma shows adipocytes and lymphocytes (H&E, 10X). (All Image left to right)
(a) Photomicrograph highlighting the lymphatic and the vascular channels stained positively by CD31 in Case 1 (IHC, 10X); (b) Photomicrograph highlighting the lymphaticovenous channels on CD31 stain in Case 2 (IHC, 10X). (All Image left to right)
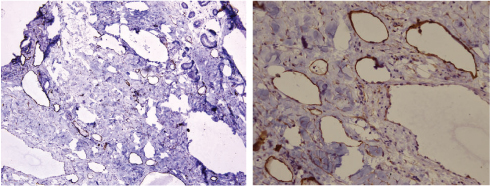
(a) Photomicrograph highlighting the lymphatic channels by D2-40 in Case 1 (IHC, 10X); (b) Photomicrograph highlighting only the lymphatics on D4-40 stain in Case 2 (IHC, 40X). (All Image left to right)
Both our patients were treated by complete surgical excision and have remained disease free after three and four months respectively.
Discussion
CVMs represent a group of vascular anomalies that are the result of defective development of the vascular system. They present at birth as an inborn vascular defect arising from the various stages of embryogenesis. They may involve one or more components of the peripheral circulation systems: arterial, venous, lymphatic and capillary systems [1]. Vascular malformations are defined as disorganized vascular development without new cell growth. LVMs, also known as haemangio-lymphangiomas are rare congenital tumours affecting mainly the head and neck area [2,3] and account for about 12% of vascular anomalies. These usually present spontaneously after birth but can be diagnosed prenatally during ultrasound. LVMs can be associated with Noonan’s syndrome and Klippel-Trenaunay syndrome. The cases often present as new onset or as enlargement of pre-existing swelling following trauma or infection [4,5]. LVMs are slow flow lesions commonly located in order of frequency in the head and neck, axilla, chest, and proximal upper extremity and are related to maldevelopment of primitive jugular, subclavian, and axillary lymphatic sacs [1]. Our cases were of four and half-year-old and seven-year-old boy who presented with gradual enlargement of preexisting swellings.
The true incidence of lymphangiomas may be uncertain as some of them may not be very evident. The most common types of vascular malformations are venous, lymphatic, and venolymphatic with an overall prevalence of up to 1% in the general population [6].
Two hypothesis have been proposed: firstly, the condition results from malformation of lymphatic vascular pathways; and secondly that it represents a tumour that grows by cellular (mainly endothelial) hyperplasia. The mutations involving VEGR3 and TIE2/TEK genes have been found to be associated in vascular malformations including lymphangiomas [6].
Many classifications are proposed for LVM. The International Society for the Study of Vascular Anomalies Classification (ISSVA) system divides vascular anomalies into two primary biological categories: vasoproliferative or vascular neoplasms and vascular malformations. There is increased endothelial cell proliferation and mitosis in vasoproliferative neoplasms whereas vascular malformations do not have increased endothelial cell turnover. Vascular malformations are classified according to the size into macrocystic (spaces≥ 2 ml), microcystic (spaces < 2 ml), or mixed type [7] according to the extent of the lesion in the cervicofacial area [8]. Vascular malformations unlike vasoproliferative malformations do not have increased endothelial cell turnover.
Diagnostic modalities for LVM are ultrasonography, MRI, angiography which usually reveals a multiloculated cystic lesion with low intensity [1].
Microscopically, they are made up of anastomosing lymphatic and venous channels. Our cases showed similar histology. The differential diagnosis included haemangiomas and arterio venous malformation. Demonstration of lymphatic channels on D2-40 or podoplanin helped us reach the appropriate diagnosis. IHC was done with CD31 to highlight the vascular and lymphatic channels followed by D2-40 which highlighted the lymphatics exclusively.
Management of LVMs is often not easy and depends on size, extent, and presenting symptoms of the lesion [1]. This condition has been treated by various modalities such as observation, aspiration, sclerotherapy, and surgical excision. Complete surgical excision still the standard option to treat LVMs by many surgeons. Complete surgical excision has shown a low rate of recurrence [9]. Both our patients were treated by complete surgical excision and have remained disease free after three and four month respectively.
Conclusion
We presented two cases of LVM, which is a rare entity. Both the cases were presented early after birth. The treatment modality was complete surgical excision.
[1]. Lee BB, Villavicencio L, Chapter 68. General considerations. Congenital vascular malformations. Section 9. Arteriovenous anomalies. In: Cronenwett JL, Johnston KW, edsRutherford’s Vascular Surgery 2010 7th ednPhiladelphia, PA, USASaunders Elsevier:1046-64. [Google Scholar]
[2]. Kukk E, Lymboussaki A, Taira S, Kaipainen A, Jeltsch M, Joukov V, VEGF-C receptor binding and pattern of expression with VEGFR-3 suggests a role in lymphaticvascular developmentDevlopm 1996 122:3829-37. [Google Scholar]
[3]. Eichmann A, Carbel C, Jaffredo T, Bréant C, Joukov V, Kumar V, Avian VEGF-C: Cloning, embryonic expression pattern and stimulation of VEGFR2-expressing endothelial cell precursorsDevlopm 1998 125:743-52. [Google Scholar]
[4]. Oduber CE, Van Beers EJ, Bresser P, van der Horst CM, Meijers JC, Gerdes VE, Venous thromboembolism and prothrombic parameters in Klippley-Trenauney syndromeNeth J Med 2013 71:246-52. [Google Scholar]
[5]. Croonen EA, Nillesen WM, Stuurman KE, Oudesluijs G, van de Laar IM, Martens L, Prenatal diagnostic testing of the noonan syndrome genes in foetuses with abnormal ultrasound findingsEur J Hum Genet 2013 21:936-42. [Google Scholar]
[6]. Hisin YH, Ho CC, Huang PH, Hsu SM, Co-Expression of VEGF-C and its receptors, VEGFR-2 and VEGFR-3, in endothelial cells of lymphangioma. Implication in autocrine or paracrine regulation of lymphangiomaLaboratory Investigation 2001 81:1729-34. [Google Scholar]
[7]. Greinwald JH Jr, Burke OK, Sato Y, Poust RI, Kimura K, Bauman NM, Treatment of lymphangiomas in children: An update of picibanil (OK-432) sclerotherapyOtolaryngol Head Neck Surg 1999 121:381-87. [Google Scholar]
[8]. De Serres LM, Sie KC, Richardson MA, Lymphatic malformations of the head and neck. A proposal for stagingArch Otolaryngol Head Neck Surg 1995 121:577-82. [Google Scholar]
[9]. Giguere CM, Bauman NM, Sato Y, Burke DK, Greinwald JH, Pransky S, Treatment of lymphangiomas with OK-432 (picibanil) sclerotherapy: A prospective multi institutional trialArch Otolaryngol Head Neck Surg 2002 128:1137-44. [Google Scholar]