Squamous Cell Carcinoma of Cervix with Isolated Metastasis to Ethmoidal Sinus: A Rare Occurrence
Prita Pradhan1, Debasis Gochhait2, Arun Kumar3
1 Junior Resident, Department of Pathology, Jawaharlal Institute of Post graduate Medical Education and Research, Puducherry, India.
2 Assistant Professor, Department of Pathology, Jawaharlal Institute of Post graduate Medical Education and Research, Puducherry, India.
3 Senior Resident, Department of Pathology, Jawaharlal Institute of Post graduate Medical Education and Research, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arun Kumar, Senior Resident, Department of Pathology, Jawaharlal Institute of Post graduate Medical Education and Research, Puducherry, India.
E-mail: arukuma2103@gmail.com
Squamous Cell Carcinoma (SCC) of the cervix is a highly prevalent malignancy. Its spread and metastasis is mostly loco-regional. The occurrence of distant extra-pelvic metastases is exceedingly rare, particularly with the involvement of paranasal sinus. This case report documents an unusual presentation of a 45-year-old female diagnosed and treated for squamous cell carcinoma of cervix with metastatic deposits in the ethmoidal sinus without deposits in any intervening foci.
Cervical, Extra-pelvic, Nasal endoscopy, Paranasal sinus, Radiation
Case Report
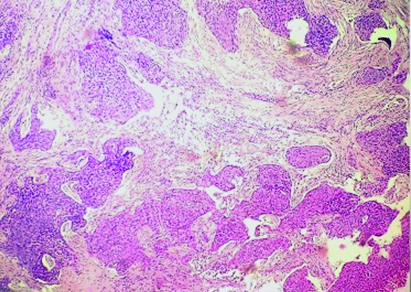
A 45-year-old female (para three, live three), who was post-menopausal for seven years, presented with foul smelling discharge and bleeding per vaginum. On examination there was an ulceroproliferative growth involving the entire cervix, all the fornices and the anterior wall of lower one third of the vagina. Bilateral parametria were involved, which was reaching up to the lateral pelvic wall on the right side. Rectal mucosa was free. A clinical diagnosis of carcinoma cervix III B was made which was confirmed on the histopathologic examination [Table/Fig-1]. Radiotherapy was given 46Gy/23fx→HDRI, II and II→PO boost 10 Gy/5fx.
Section from the cervix showing nests of polygonal malignant squamous cells infiltrating into the cervical stroma and desmoplastic response. (H&E, 20X);
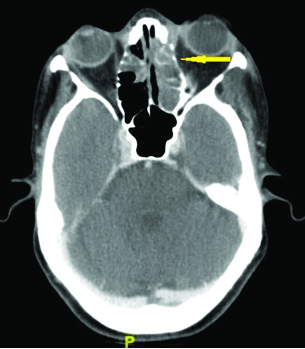
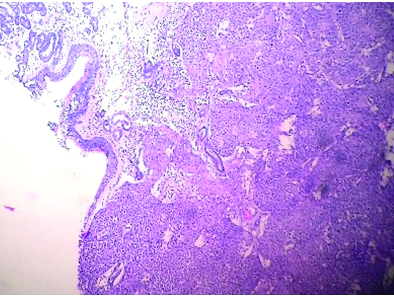
Within two months of completion of her radiotherapy she presented with left orbital swelling for three weeks duration. On examination, there was fullness in the left frontal region, periorbital oedema and conjunctival discharge in the left eye. Left eye was displaced 5 mm medially and 10 cm inferiorly. Mild disc pallor with a cup disc ratio of 0.3 and defined margins was noted. Contrast Enhanced Computed Tomography (CECT) showed a well defined lesion in the left frontal and ethmoidal sinus and soft tissue density in the left frontal region measuring 4 x 1 cm, with no obvious intracranial extension [Table/Fig-2]. Diagnostic Nasal Endoscopy (DNE) showed a friable, granular and irregular mass predominantly in the left anterior and posterior ethmoidal cells. Biopsy was taken during DNE from the mass, which showed multiple tissue bits lined by respiratory epithelium. The subepithelium showed nests of tumour cells composed of polygonal cells having mildly hyperchromatic nuclei with moderate to abundant eosinophilic cytoplasm and prominent intercellular bridging. Mitoses were frequent. These nests were separated with fibrocollagenous septa with mild chronic inflammatory infiltrate. The tumour cells showed diffuse strong nuclear positivity for p63 confirming a squamous cell carcinoma [Table/Fig-3,4 and 5]. Positron Emission Tomography (PET) scan was done which did not show metastatic deposits in any other intervening foci. Hence, possibility of a metastatic SCC was considered in view of the past history. Patient was planned for palliative care with radiation and is currently on follow up for the last four months.
Contrast Enhanced CT (CECT) of the paranasal sinus showing a 4 x 1 cm well-defined, soft tissue density in the left frontal and ethmoidal sinus (arrow) with no evidence of intracranial extension;
Biopsy from the ethmoidal sinus on low power, showing the tissue lined by respiratory epithelium with nests of cells infiltrating the stroma. (H&E, 10X).
High power view of the ethmoidal sinus biopsy showing nests of cells showing polygonal cells with prominent intercellular bridging, hyperchromatic pleomorphic nucleus having coarse chromatin and high nucleus to cytoplasm ratio. (H&E, 40X).
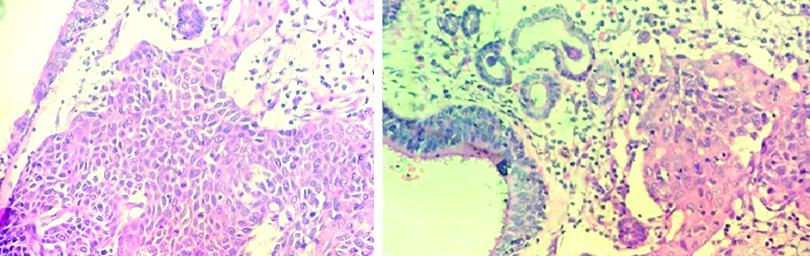
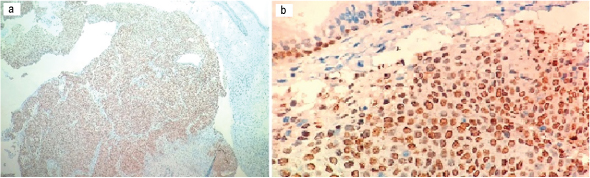
The p63 immunostains show diffuse strong nuclear positivity seen in the nests of malignant cells below the respiratory epithelium. (a; 10X, b;40X).
Discussion
Carcinoma of the cervix is one of the common diseases in India and a common cause of cancer related morbidity and mortality [1]. Most of the cases of carcinoma cervix spread in a contiguous fashion and via lymphatics mostly resulting in pelvic organ involvement and lymph node infiltrate. Extra-pelvic deposits are quite rare. However, they have been documented in the brain, bone and gastrointestinal tract [2–4]. Ethmoidal sinus as a site of metastasis is scarcely documented in literature. Most cases of ethmoidal sinus metastasis are adenocarcinomas recorded to arise from primaries in the kidney or breast [5,6]. This case to our knowledge is the first of its kind for it shows a SCC arising in the cervix metastasising to an unusual location like ethmoidal sinus. Unlike the established literature this tumour was found to be confined only to the ethmoidal sinus. The underlying brain and meninges were found to be free of tumour [5,6].
As was highlighted in an autopsy-based study, this case impresses an important understanding of the mechanisms of spread in cases of carcinoma cervix. The subsets of patients managed with radiation as a primary modality of treatment showed a higher propensity to present with extra-pelvic metastases, often sparing the intervening local organs. The extra-pelvic sites are often found to be lung and liver [7]. However, as shown here the deposits can be at unusual sites causing unusual presentations, which can cause diagnostic difficulties. Particularly interesting is presentation of the metastatic disease at an extra-pelvic location without involvement of any intervening lymph node or organ. The local pelvic organs and the lymph nodes were found to be free from the disease [7]. This is possibly due to better local disease control due to radiation. However, the short duration of time within which the metastatic deposit presented in the given case is very unusual and lead to diagnostic difficulties. The provided history and immunohistochemical evaluation showing diffuse strong nuclear positivity for p63 in the given case helped in confirming the diagnosis.
A careful and complete history taking, diagnostic assessment performed and treatment provided at time of primary diagnosis, a robust multidisciplinary approach involving relevant radiological interventions with an appropriate sampling for histopathologic examination and a pertinent immunohistochemical evaluation can help in diagnosing these common tumours at unusual locations with greater certainty.
Conclusion
Metastatic carcinoma cervix requires timely diagnosis and appropriate management to minimise morbidity and mortality. Presentation with metastasis at extra-pelvic sites like ethmoidal sinus is rare, but needs to be suspected and diagnosed with the help of appropriate correlation of the history, the clinico-radiologic details, with the histomorphology and appropriate immunohistochemistry.
[1]. ICO Information Centre on HPV and cancer (Summary Report 2014-08-22). Human Papillomavirus and Related Diseases in India. 2014 [Google Scholar]
[2]. Balaji R, Ramachandran K, Kumar A, Krishnakumar AS, Venugopal M, Pachymeningeal metastasis from squamous cell carcinoma of the uterine cervix with involvement of the optic nerve: case report and review of the literatureCancer Imaging 2007 24:138-40. [Google Scholar]
[3]. Pasricha R, Tiwari A, Aggarwal T, Lal P, Carcinoma of uterine cervix with isolated metastasis to fibula and its unusual behavior: report of a case and review of literatureJ Cancer Res Ther 2006 2:79-81. [Google Scholar]
[4]. Raphael JC, Ram TS, Pavamani S, Choudharie L, Viswanathan PN, Squamous cell carcinoma cervix with metastasis to pyloroduodenal regionJ Cancer Res Ther 2011 7:183-84. [Google Scholar]
[5]. Larrosa F, Aguilar F, Traserra J, Ethmoidal metastasis of renal adenocarcinomaActa Otorrinolaringológica Esp 2000 51:76-79. [Google Scholar]
[6]. García Triguero D, Molina Quirós C, Sanz Fernández R, Ethmoid metastasis of primary breast tumorActa Otorrinolaringológica Esp 1998 49:163-64. [Google Scholar]
[7]. Badib AO, Kurohara SS, Webster JH, Pickren JW, Metastasis to organs in carcinoma of the uterine cervix. Influence of treatment on incidence and distributionCancer 1968 21:434-39. [Google Scholar]