Missing IUCD Strings: Role of Imaging in Locating the Misplaced Device
Deepti Goswami1, Anoosha K. Ravi2, Akanksha Sharma3
1 Professor, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
2 Junior Resident, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
3 Senior Resident, Department of Obstetrics and Gynaecology, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepti Goswami, Professor, Department of Obstetrcis and Gynaecology, Maulana Azad Medical College, Bahadur Shah Zafar Marg-110002, New Delhi, India.
E-mail: drdeeptigoswami@hotmail.com
Contraception, Cystoscopy, Intrauterine devices, Uterine perforation
A 30-year-old woman, para 7, presented with lower abdominal pain to the Gynaecology Outpatient Clinic. She had been experiencing the pain since the insertion of IUCD six months back. She was not aware of the type of IUCD inserted. Three months after the IUCD insertion she had conceived while the device was in situ. She had undergone termination of pregnancy at seven weeks of gestation. Uterine evacuation was done elsewhere one month back and pain had worsened since then. The IUCD was not retrieved during the procedure. She had no complaints of abnormal vaginal bleeding or disturbance of bowel or bladder habits. Her vital signs were stable and systemic examination was unremarkable. IUCD strings were not visualized on per speculum examination and per vaginal examination revealed mild uterine tenderness.
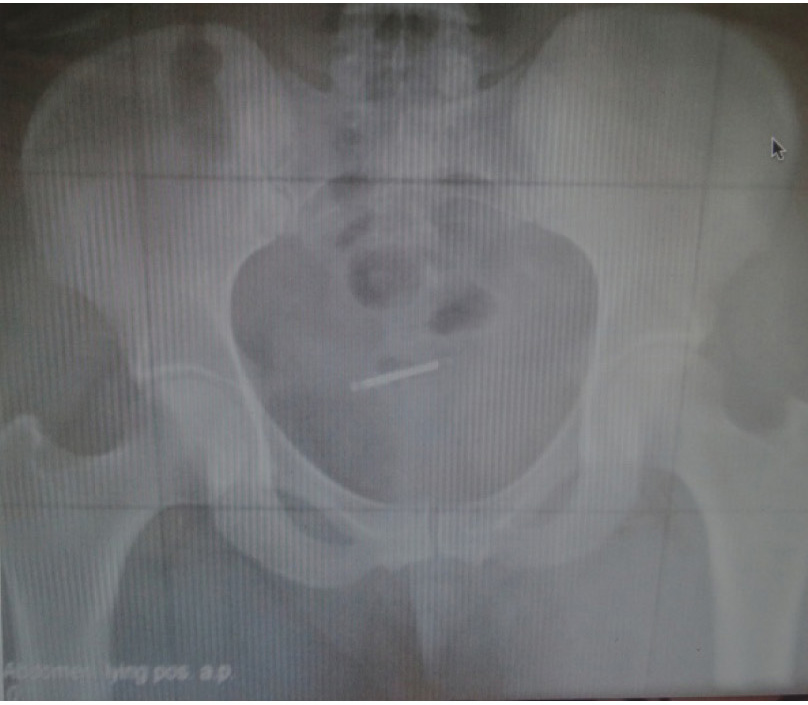
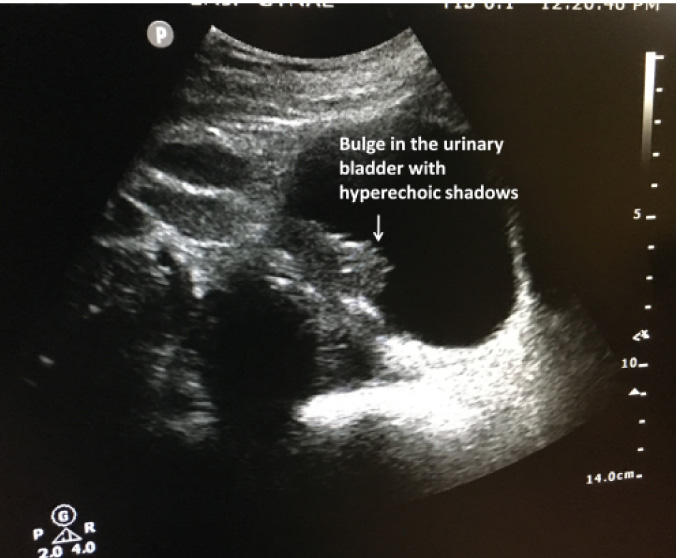
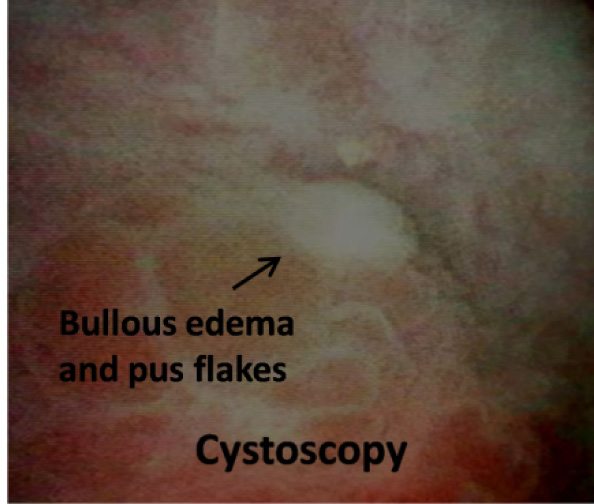
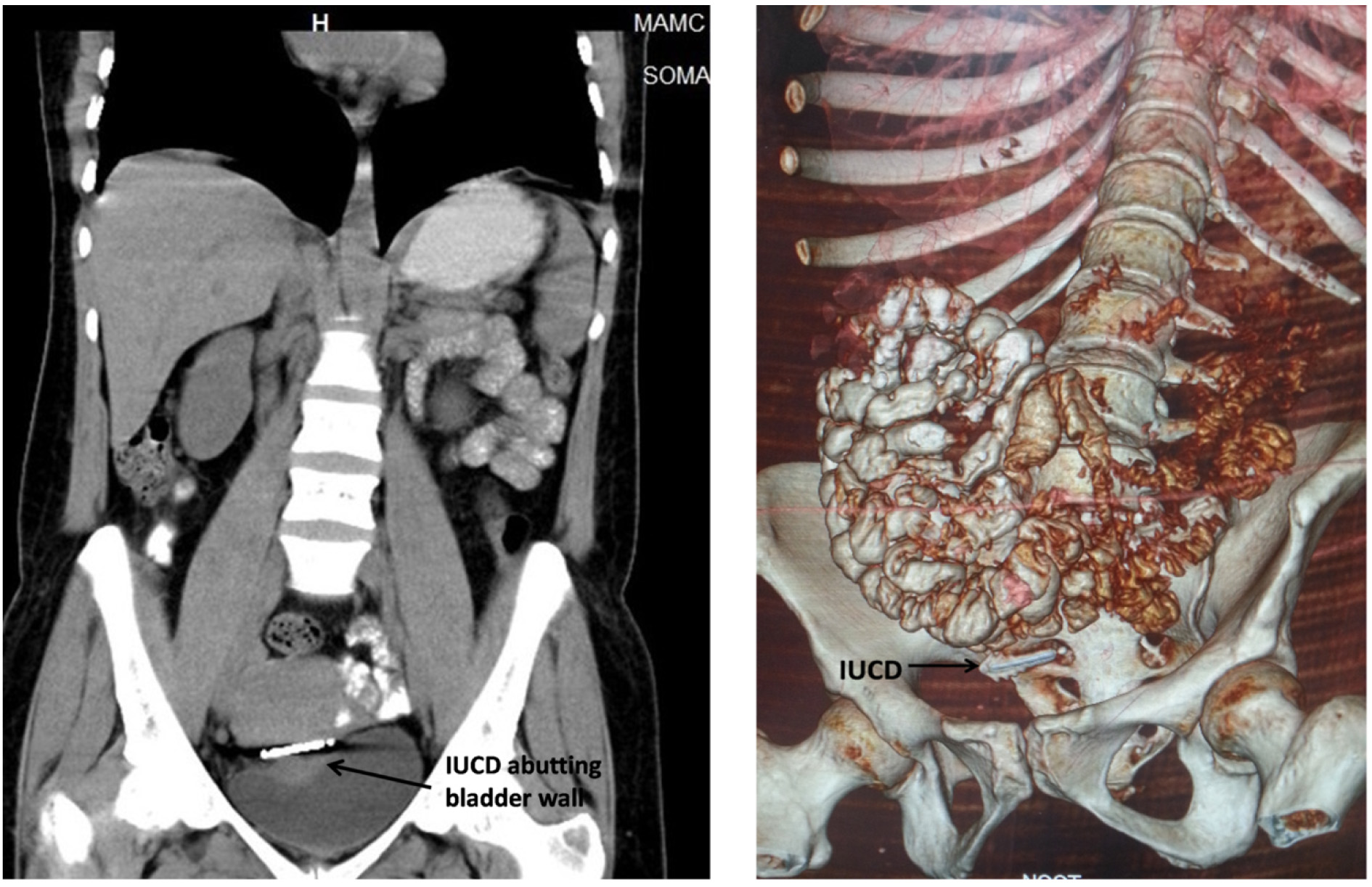
X-ray imaging showed the IUCD lying in the pelvic region [Table/Fig-1]. Transabdominal Ultrasonography (USG) showed normal endometrial stripe with no evidence of IUCD in the endometrial cavity. Hyperechoic shadows were visualised in the anterior myometrium along with a bulge in the adjacent bladder wall [Table/Fig-2]. Since perforation of the urinary bladder could not be ruled out, cystoscopy was done which revealed bullous oedema in the right lateral aspect of dome of bladder and a few pus flakes [Table/Fig-3]. However, IUCD was not visualized. Subsequently on Non-Contrast Computed Tomography (NCCT), IUCD was found lying between urinary bladder and uterus with focal thickening in right posterolateral wall of the urinary bladder [Table/Fig-4]. There was no evidence of breach in the bladder wall.
X-Ray Image showing IUCD in the pelvis.
USG image showing bulge in bladder wall and hyperechoic shadows suggestive of IUCD.
Cystoscopic view of bladder wall.
CT scan and 3D image localizing the IUCD between uterus and bladder wall.
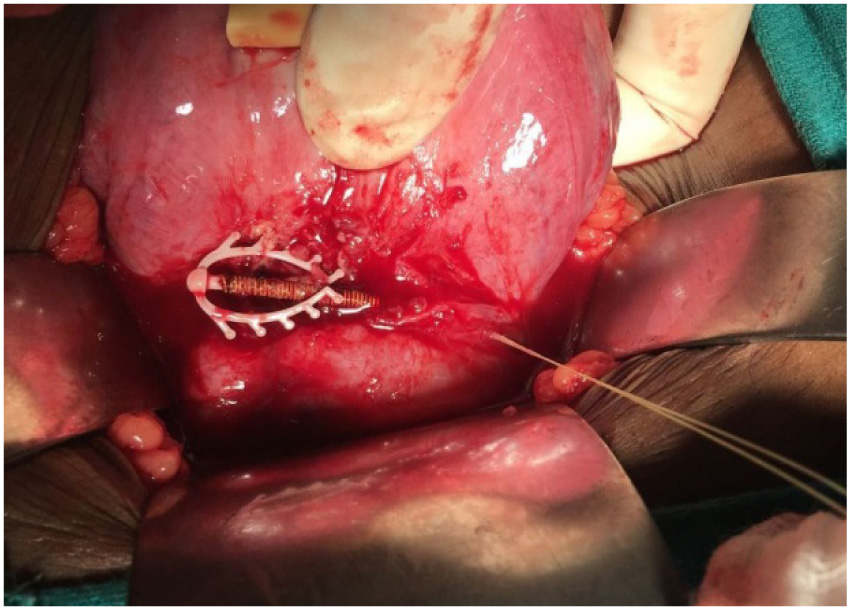
Patient was taken up for laparotomy. On opening the abdomen, the strings of IUCD were seen emerging out of the anterior wall of uterus adjacent to the bladder reflection. Sharp dissection in the uterovesical plane revealed a multiload device that had partly migrated across the uterine serosa. Its spikes were indenting the bladder wall [Table/Fig-5]. A small pocket of pus around the device was evacuated. Postoperative recovery of the patient was uneventful.
Operative findings showing the multiload IUCD buried beneath the uterine serosa with threads protruding out into the peritoneal cavity.
IUCD is a popular method of long term reversible contraception with failure rate of less than one per 100 women-years. Its side effects are few and generally well tolerated. Missing IUCD strings are observed in about 5% of the users [1]. The device is located within the endometrial cavity or cervical canal in 95% of the cases [2]. However, in a few cases it can perforate the uterus and migrate into adjoining structures. The underlying causes include perforation of the uterus at the time of insertion that occurs in 1-2 cases per 1000 insertions [3]. Secondary migration may occur later on due to chronic inflammation causing erosion of the uterine wall [4]. No difference has been found in the incidence of perforation for various IUCD devices [5]. Sites of migration are usually within pelvis or in omentum but at times the device may migrate far into upper abdomen. Even if asymptomatic, all misplaced IUCDs lying outside the uterus should be retrieved through laparoscopy or laparotomy to avoid complications like adhesions, fistula formation and intestinal obstruction.
Women with missing IUCD threads are usually asymptomatic. Some may report mild symptoms of abdominal pain with or without abnormal uterine bleeding. Occurrence of pregnancy in a woman using IUCD should raise the suspicion of misplaced device. In this case, the history of conception suggests that the IUCD was not in the correct place. There is a possibility of perforation of the uterus at the time of insertion of IUCD as patient was experiencing pain since the time of insertion. Subsequent uterine curettage could have displaced the device further and caused local infection as evidenced by pus collection in the tissue surrounding the device. This explains the exacerbation of the pain after curettage.
Misplaced IUCD are localized with the help of imaging techniques. X-ray of abdomen or pelvic sonography is the first modality of investigation. USG usually suffices to locate the IUCD as most of the times the device is present in the uterine cavity. CT scan helps in locating the IUCD that has migrated outside the uterus. Cystoscopy helps diagnose intravesical IUCD. In the presented case, USG findings were suggestive of bladder hematoma raising the possibility of bladder perforation by the IUCD. Cystoscopy ruled out bladder wall perforation and CT scan localised the IUCD precisely. Operative findings confirmed the imaging reports.
Non visualization of IUCD strings is suggestive of misplaced device. Judicious use of multimodality imaging helps in localizing the misplaced IUCD accurately. This is essential for planning the appropriate intervention to retrieve the device.
[1]. Marchi NM, Castro S, Hidalgo MM, Hidalgo C, Monteiro-Dantas C, Villarroeal M, Management of missing strings in users of intrauterine contraceptivesContraception 2012 86(4):354-58. [Google Scholar]
[2]. Barsaul M, Sharma N, Sangwan K, 324 cases of misplaced IUCD--a 5-year studyTrop Doct 2003 33(1):11-12. [Google Scholar]
[3]. Chi I, Feldblum PJ, Rogers SM, IUD--related uterine perforation: An epidemiologic analysis of a rare event using an international datasetContracept Deliv Syst 1984 5(2):123-30. [Google Scholar]
[4]. Zakin D, Stern WZ, Rosenblatt R, Complete and partial uterine perforation and embedding following insertion of intrauterine devicesObstet Gynecol Surv 1981 36(7):335-53. [Google Scholar]
[5]. O’Brien PA, Kulier R, Helmerhorst FM, Usher-Patel M, d’Arcangues C, Copper-containing, framed intrauterine devices for contraception: A systematic review of randomized controlled trialsContraception 2008 77(5):318-27. [Google Scholar]