Meckel’s Diverticulum Enterolith: An Extremely Rare Cause of Intestinal Obstruction
Nikolaos Symeonidis1, Athanasios Kofinas2, Kyriakos Psarras3, Efstathios Pavlidis4, Theodoros Pavlidis5
1 Consultant Surgeon, Second Surgical Propedeutic Department, Aristotle University of Thessaloniki, Medical School, Thessaloniki, Greece.
2 Resident Surgeon, Second Surgical Propedeutic Department, Aristotle University of Thessaloniki, Medical School, Thessaloniki, Greece.
3 Assistant Professor, Second Surgical Propedeutic Department, Aristotle University of Thessaloniki, Medical School, Thessaloniki, Greece.
4 Consultant Surgeon, Second Surgical Propedeutic Department, Aristotle University of Thessaloniki, Medical School, Thessaloniki, Greece.
5 Professor, Second Surgical Propedeutic Department, Aristotle University of Thessaloniki, Medical School, Thessaloniki, Greece.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nikolaos Symeonidis, Hippokratio General Hospital, Konstantinoupoleos 49, Thessaloniki-56224, Greece.
E-mail: niksym@hotmail.com
Meckel’s diverticulum is usually asymptomatic but occasionally presents with complications. Formation of an enterolith inside a Meckel’s diverticulum is very uncommon and dislodgement of such a stone causing obstruction is extremely rare. We herein present a case of a 48-year-old man who presented with small bowel obstruction. Preoperative radiologic studies revealed a stone-like lesion in the right lower quadrant. Upon laparotomy, an inflamed Meckel’s diverticulum was found as well as a 2.5 cm stone obstructing the terminal ileum. The stone was removed and the diverticulum was excised. The differential diagnosis of acute intestinal obstruction should include this extremely rare clinical entity especially when the combination of small bowel obstruction with radiopaque stone-like finding on preoperative x-rays is present.
Intestinal stone, Meckelitis, Small bowel obstruction
Case Report
A 48-year-old male presented to the emergency department with a 48-hour history of diffuse abdominal discomfort, which progressed to colicky right lower quadrant pain accompanied with abdominal distention, bilious vomiting and lack of flatulence.
He was afebrile, with normal vital signs. Physical examination revealed increased bowel sounds and tenderness on the right iliac fossa.
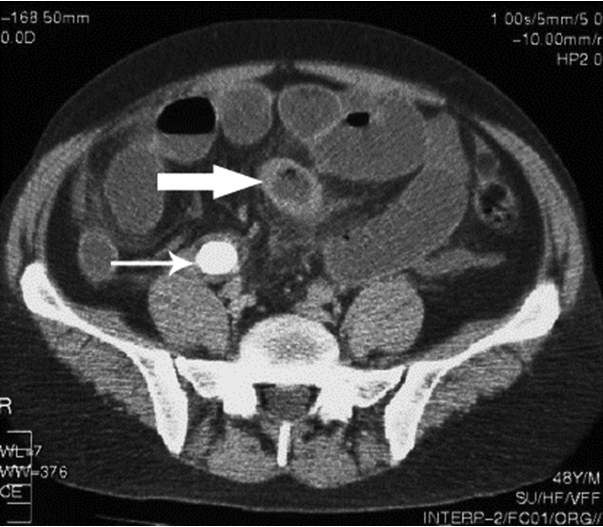
No hernias were detected and digital rectal examination was normal. Past history included an appendectomy during childhood. White blood cell count was elevated (16340/ μL). Abdominal X-ray showed dilatation of small bowel loops and a radiopaque lesion in the right lower quadrant [Table/Fig-1]. Computed Tomography (CT) scan confirmed the obstruction of small bowel, with thickening of jejunal and ileal loops and a transition point in the distal ileum, after which the colon appeared collapsed.
Abdominal X-ray showing dilated small bowel loops and the radiopaque lesion (enterolith) in the right lower quadrant.
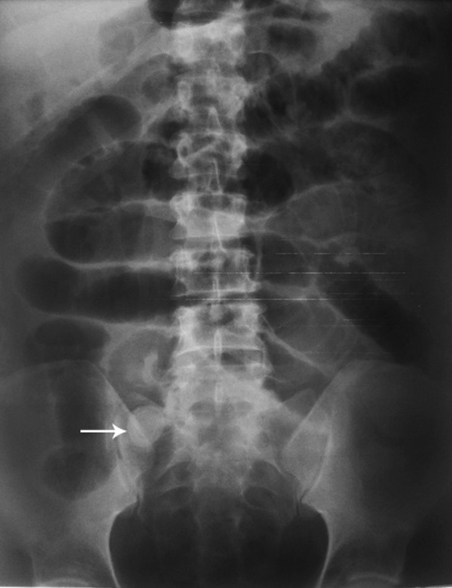
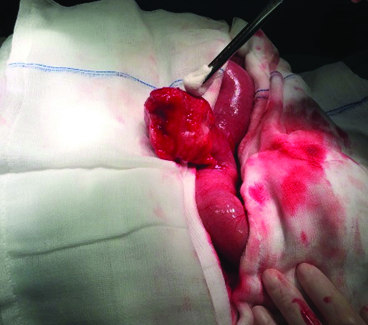
Just proximal to this point, a radio-opaque high-density lesion with radiolucent center was found, measuring approximately 2.5 cm in diameter. An inflamed blind intestinal pouch was also visible, suggestive of the presence of a Meckel’s diverticulum [Table/Fig-2]. Upon laparotomy, an inflamed Meckel’s diverticulum was found approximately 40 cm from the caecum [Table/Fig-3] and an enterolith was palpated downstream impacted in the ileocecal junction causing the obstruction.
CT scan showing dilated small bowel loops, presence of a radiopaque lesion with radiolucent center (small arrow) and a Meckel’s diverticulum (big arrow).
The inflammed Meckel’s diverticulum.
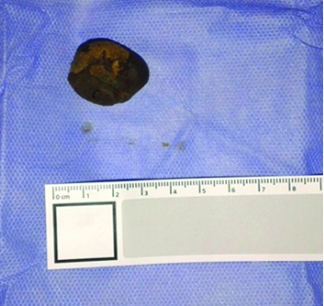
The enterolith was milked upstream and removed from an incision made at the site of excision of the Meckel’s diverticulum, just above its base [Table/Fig-4]. The diverticulum was excised with the application of a linear stapler at its base, below the diverticulotomy.
The patient had an uneventful recovery and was discharged on the sixth postoperative day. Histology showed mucosal ulceration and diverticular wall necrosis [Table/Fig-5].
Transmural ischaemic haemorragic necrosis of the Meckel’s diverticulum (H&E ×250).

Discussion
Meckel’s diverticulum represents the most common congenital malformation of the gastrointestinal tract, with a reported incidence of 2-4% [1]. It is a remnant of the omphalomesenteric duct and as a true diverticulum, it contains all layers of the intestinal wall. It arises from the antimesenteric border of the small intestine, usually located 40-60 cm proximally to the ileocecal valve [1]. Meckel’s diverticulum in the majority of the cases is asymptomatic. Occasionally it manifests in the form of a complication such as bleeding (28%), intussusception (13%), obstruction (11%), diverticulitis (8%) and volvulus (5%). Bleeding is the most common presentation in the pediatric population [2]. Enterolithiasis is an uncommon medical condition with a reported prevalence of 0, 3-10% [3]. In the setting of Meckel’s diverticulum, enteroliths are present in 3-10% of the patients, with a 3:1 male to female ratio [4]. Patients with a Meckel’s diverticulum have a lifetime risk of complications ranging from 4-6.4% the most common of which are hemorrhage, inflammation and intestinal obstruction [5]. Small bowel obstruction in the presence of a Meckel’s diverticulum usually happens due to local inflammation, external compression of adjacent loops (Mirizzi-type) [6], volvulus, intussusception, adhesions, fibrous bands or internal herniation. However, dislodgement of an enterolith from a Meckel’s diverticulum causing intestinal obstruction is an extremely rare occurrence. Literature search with Pubmed, Embase and Google Scholar using the MeSH terms Meckel’s diverticulum, enterolith or faecolith, intestinal obstruction revealed only 13 similar cases previously reported [Table/Fig-6] [7-19].
Previously reported cases of intestinal obstruction caused by a Meckel’s enterolith. N/A: data not available.
| Author | Age | Sex | Diagnosis | Radiopaque |
|---|
| Field RJ et al., [7] | 53 | M | Intraoperative | NO |
| Danzis M [8] | N/A | N/A | N/A | N/A |
| Grosdidier J et al., [9] | N/A | N/A | N/A | N/A |
| Benhamou G et al., [10] | N/A | N/A | N/A | N/A |
| Grant AB et al., [11] | 65 | M | Intraoperative | NO |
| Lopez PV et al., [12] | 85 | M | X-Ray/Intraoperative | YES |
| Rudge FW[13] | N/A | N/A | N/A | N/A |
| Trésallet C et al., [14] | 37 | M | CT | YES |
| Rice RD et al., [15] | 73 | M | CT | YES |
| McCallion WA et al.,[16] | 37 | F | INTRAOPERATIVE | NO |
| Garrigós G et al., [17] | 62 | M | X-Ray/US | YES |
| Gamblin TC et al., [18] | 24 | M | Intraoperative | NO |
| Demetriou et al., [19] | 30 | F | X-Ray/CT | YES |
| Symeonidis et al., [present case] | 48 | M | X-Ray/ CT | YES |
Enteroliths formed in a Meckel’s diverticulum represent primary intestinal stones. Predisposing factors for their creation include intestinal stasis, inflammation and extreme alkaline or acidic intraluminal environment, which result in precipitation of calcium or bile salts respectively. 30-50% of enteroliths are radiopaque and therefore easily detected with abdominal x-rays or CT scan. They are typically depicted as round or triangular with dense periphery and radiolucent center or they can appear laminated [3]. Differential diagnosis includes gallstones, which occasionally can present with intestinal obstruction, as well as other abdominal and pelvic calcified lesions like kidney stones, swallowed foreign bodies, phleboliths, fecaliths, calcified lymph nodes, teratomas, etc.
Management of Meckel’s stone ileus is mainly surgical. Treatment options include bowel resection with primary anastomosis, digital fragmentation of the enterolith and manual guiding (milking) of the fragments towards the large intestine or removal of the stone through a proximal enterotomy. Laparoscopic approach has been deemed safe and effective both as a diagnostic and therapeutic tool in symptomatic Meckel’s diverticulosis [17], but there have been no reports of cases in which intestinal obstruction due to a Meckel’s enterolith was treated laparoscopically.
Conclusion
Meckel’s enterolith causing intestinal obstruction is an extremely rare complication of Meckel’s diverticulosis. It should be included in the differential diagnosis of acute intestinal obstruction, especially if an enterolith is found in preoperative radiology studies. However, diagnosis of this condition is usually made during exploratory laparotomy. The consulting surgeon should be aware that the combination of small bowel obstruction with radiopaque stone-like finding on preoperative x-rays is indicative of this extremely rare clinical entity, which warrants immediate surgical treatment.
[1]. Sagar J, Kumar V, Shah DK, Meckel’s diverticulum: a systematic reviewJR Soc Med 2007 100(2):69 [Google Scholar]
[2]. Kusumoto H, Yoshida M, Takahashi I, Anai H, Maehara Y, Sugimachi K, Complications and diagnosis of Meckel’s diverticulum in 776 patientsAm J Surg 1992 164(4):382-83. [Google Scholar]
[3]. Gurvits GE, Lan G, EnterolithiasisWorld J Gastroenterol 2014 20:17819-29. [Google Scholar]
[4]. Gadhia U, Raju D, Kapoor R, Large enterolith in a meckels diverticulum causing perforation and bowel obstruction: an interesting case with review of literatureIndian J Surg 2013 75:177-79. [Google Scholar]
[5]. Bani-Hani KE, Shatnawi NJ, Meckel’s diverticulum: comparison of incidental and symptomatic casesWorld J Surg 2004 28(9):917-20. [Google Scholar]
[6]. Jones RP, McWhirter D, Intermittent small bowel obstruction caused by Meckel’s enterolithAnn R Coll Surg Engl 2010 92(5):W16-17. [Google Scholar]
[7]. Field RJ Sr., Field RJ Jr, Intestinal obstruction produced by fecalith arising in Meckel’s diverticulumAMA Arch Surg 1959 79(1):8-9. [Google Scholar]
[8]. Danzis M, Intestinal obstruction in Meckel’s diverticulum with report of a case with a large enterolithJ Med Soc N J 1950 47(12):548-53. [Google Scholar]
[9]. Grosdidier J, Rollin B, Richaume B, Intestinal obstruction caused by a coprolith originating in a Meckel’s diverticulumSem Hop 1972 48(41):2661-64. [Google Scholar]
[10]. Benhamou G, Small intestinal obstruction by an enterolith from a Meckel’s diverticulumInt Surg 1979 64(1):43-45. [Google Scholar]
[11]. Grant AB, Meckel stone ileus: a case reportAust NZJ Surg 1981 51(1):77-78. [Google Scholar]
[12]. Lopez PV, Welch JP, Enterolith intestinal obstruction owing to acquired and congenital diverticulosis. Report of two cases and review of the literatureDis Colon Rectum 1991 34(10):941-44. [Google Scholar]
[13]. Rudge FW, Meckel’s stone ileusMil Med 1992 157:98-100. [Google Scholar]
[14]. Trésallet C, Renard-Penna R, Nguyen-Thanh Q, Cardot V, Chigot JP, Menegaux F, Intestinal obstruction by an enterolith from a perforated giant Meckel’s diverticulum: diagnosis with CT reconstructed imagesInt Surg 2007 92(3):125-27. [Google Scholar]
[15]. Rice RD, Parker DM, Seery JM, Arciero CA, A small bowel obstruction secondary to a Meckel’s enterolithAm Surg 2010 76(2):222-24. [Google Scholar]
[16]. McCallion WA, Higgins PM, Dane TE, Enterolith obstruction of the small bowelUlster Med J 1992 61:179-81. [Google Scholar]
[17]. Garrigós G, Gómez SÁ, Peris N, Ripollés T, Martínez Abad M, Intestinal obstruction due to Meckel’s diverticulum enterolithiasisCir Esp 2012 90(10):674-76. [Google Scholar]
[18]. Gamblin TC, Glenn J, Herring D, McKinney WB, Bowel obstruction caused by a Meckel’s diverticulum enterolith: a case report and review of the literatureCurr Surg 2003 60:63-64. [Google Scholar]
[19]. Demetriou V, McKean D, Briggs J, Moore N, Small bowel obstruction secondary to a liberated Meckel’s enterolithBMJ Case Rep 2013 31:2013 [Google Scholar]