Prosthetic Rehabilitation of an Insidiously Enlarged Traumatic Palatal Perforation after Orotracheal Intubation in a Young Diabetic Child
Kopal Garg1, Namita Kalra2, Rishi Tyagi3, Amit Khatri4, Gaurav Panwar5
1 Postgraduate Student, Department of Pedodontics and Preventive Dentistry, University College of Medical Sciences, Delhi University, Delhi, India.
2 Head and Professor, Department of Pedodontics and Preventive Dentistry, University College of Medical Sciences, Delhi University, Delhi, India.
3 Professor, Department of Pedodontics and Preventive Dentistry, University College of Medical Sciences, Delhi University, Delhi, India.
4 Associate Professor, Department of Pedodontics and Preventive Dentistry, University College of Medical Sciences, Delhi University, Delhi, India.
5 Postgraduate Student, Department of Pedodontics and Preventive Dentistry, University College of Medical Sciences, Delhi University, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kopal Garg, D-Pocket, Flat 771, Dilshaad Garden, Delhi-110095, India.
E-mail: kopalrocks@gmail.com
This report describes an unusual case of an insidiously enlarged traumatic palatal perforation after orotracheal intubation in a four-year-old female child with Insulin Dependent Diabetes Mellitus (IDDM). The child was first diagnosed with diabetes at 10 months of age when she was hospitalized for pneumonia. Severe respiratory distress warranted assisted ventilation via orotracheal intubation. Multiple factors namely infection, relative immunodeficiency, poor wound healing, trauma via orotracheal intubation as well as uncontrolled glucose levels, all contributed to the formation and deterioration of the palatal perforation. A palatal obturator was fabricated as an interim treatment until surgical closure could be performed.
Insulin dependent diabetes mellitus, Immunodeficiency, Palatal groove, Palatal obturator
Case Report
A four-year-old female patient was referred to the Department of Pedodontics and Preventive Dentistry by the Department of Plastic Surgery, with the chief complaint of nasal regurgitation.
The parents of the patient reported that the child was born at complete 36 weeks. Physical examination revealed an intact palate at birth. The patient was apparently normal till she was 10-month-old, when she got hospitalized for pneumonia. She had reported with very high fever, cough, poor feeding, irritability, respiratory insufficiency and failure to thrive. Blood cultures and investigations (complete blood count, haemoglobin, random blood glucose levels, HbA1c) were performed. Blood cultures were positive for Streptococcus pneumoniae and a few group B streptococci. It was at this time when the random blood glucose of the patient was observed to be above 500 mg/dl, Hb A1c at a level of 7.5% and the patient was first diagnosed with IDDM.
Supportive care included IV antibiotics, IV insulin, total parenteral nutrition, and mechanical ventilation via orotracheal intubation.
After being weaned from the ventilator (total of eight days of intubation) a deep palatal groove in the midline at the junction of the hard and soft palate was observed. A very small palatal perforation (around 0.5 mm) at the anterior end of the groove was documented by the plastic surgery team. Surgical closure was not planned as the defect was very small and predicted to resolve spontaneously. The patient was kept on subcutaneous insulin; parents were instructed to monitor pre-prandial plasma glucose levels every day and to follow up in every three months.
According to the history given by the parents, the pre-prandial plasma glucose levels of the child were perpetually above 250 mg/dl, inspite of administration of the instructed doses of insulin. Within a few weeks after discharge, the palatal hole became more noticeable to the parents. They reported with the above complaint to the Department of Plastic Surgery. Mild enlargement of the palatal perforation was confirmed. The palate was also examined carefully for any clinical signs (bifid uvula, thin translucent central zone of the soft palate or notching of the posterior hard palate) of an underlying submucous cleft which possibly led to the enlargement of the perforation. There was no such sign as well as there was a negative history of any feeding difficulty or middle ear infections by the patient which ruled out the presence of a submucous cleft. Surgical closure of the defect was deferred due to uncontrolled glucose levels.
The parents revealed that the hole insidiously increased in size till the patient was around two years of age. The child faced greater feeding difficulties despite using specially designed bottles advised by the doctors. Finally, the patient was referred to our department when she was four years old and the parents repeatedly complained the doctors about nasal regurgitation of any fluid items that were given to her. Her blood glucose levels were still uncontrolled deterring the possibility of any surgical intervention.
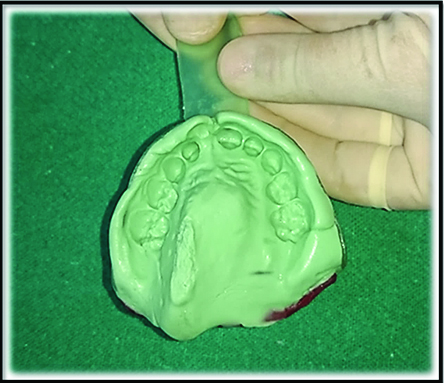
On intraoral examination, an approximately 1.5 cm x 0.5 cm palatal perforation was observed immediately left to the midline, in the hard palate, extending the entire mesiodistal dimension of the second primary molar and slightly beyond it into the soft palate [Table/Fig-1]. The pre-prandial plasma glucose level of the patient on the day of the examination was 206 mg/dl. Thus, a palatal obturator was planned for the patient as an interim treatment till her glucose levels were under control and a definitive surgical closure of the defect could be planned. Final impression was taken with medium body vinyl polysiloxane impression material and dental stone was poured to prepare a cast [Table/Fig-2]. A palatal obturator was fabricated with cold cure acrylic and delivered to the patient [Table/Fig-3].
Palatal perforation observed on oral examination.

Palatal obturator delivered.

Discussion
Palatal perforations create a communication between the nasal cavity and the oral cavity. Most often palatal defects are congenital. Occasional cases of acquired palatal perforations due to local infections [1], cocaine abuse [2], systemic diseases [3], cysts, tumours or trauma [4] have been reported. The present report describes an unusual case of an insidiously enlarged palatal perforation caused due to orotracheal intubation in a child with IDDM. Bartlett E et al., reported a similar case, in which a 2 cm palatal perforation was noted at the junction of the hard and soft palate, in a six-weekold infant subsequent to orotracheal intubation for five days. Like the present case, the infant in this case was in a state of relative immunodeficiency with sepsis and poor wound healing [5].
Diabetes is a group of metabolic diseases characterized by hyperglycaemia, resulting from defects in insulin secretion, insulin action, or both [6]. Patients with diabetes mellitus have an increased incidence of infections and their associated complications when compared to those without diabetes. Factors responsible for increased risk of infections are: decreased cellular and humoral immune responses to infections, increased virulence of some microorganisms in the high glucose environment and greater adherence of microorganisms to diabetic compared to non diabetic cells [7].
Further, experimental studies of diabetes mellitus have demonstrated delayed wound healing, including poor collagen formation and poor tensile strength, especially of deep surgical wounds [8]. Exaggeration of inflammatory reaction is observed in diabetic condition. Conversely, increased local inflammation itself increases the hyperglycaemic state [9]. This condition often necessitates frequent alterations in insulin dosage to ensure adequate blood glucose control.
In addition to the factors stated above, trauma via orotracheal intubation probably contributed to the formation of palatal perforation in this case. It was found in previous studies that normal wound healing can be expected in the diabetic patients who are treated intensively and a blood glucose level of below 250 mg/dl is established [8]. In the present case, initial size of the perforation was very small and should have healed spontaneously because adequate dosage of insulin was being administered regularly. However, the blood glucose level of the patient was continuously above 250 mg/ dl, despite frequent dose adjustment, probably causing deterioration or enlargement of the perforation. No enlargement was noticed after the patient was two years of age possibly because of better glucose control to a level below 250 mg/dl.
Palatal injuries after orotracheal intubation have been reported previously [10]. Prolonged pressure on the median palatine suture from the orotracheal tubes, inhibition of the molding forces of the tongue on the normally prominent lateral palatine ridges in a neonate, along with medial hypertrophy adjacent to the tube, all contribute to the oral complications associated with intubation [5,11]. These complications include cleft palate, palatal grooving, alveolar grooving, primary tooth dilacerations, cross-bites, high palatal vaults, poor speech intelligibility, and enamel hypoplasia [12]. Palatal perforations after orotracheal intubations however, have been reported only in immunodeficiency states or in patients with poor wound healing resulting from certain systemic illness like disseminated intravascular coagulation, diabetic ketoacidosis, etc., [5].
Conclusion
This paper highlights the fact that assisted ventilation in immunodeficient neonates can lead to formation of palatal perforations. Thus, it is extremely essential that such patients should be provided with adequate nutrition and meticulously monitored for any increase in palatal pressure. Endotracheal tubes should be secured passively avoiding excessive pressure on any surrounding structures.
[1]. F Lucatorto, LR Eversole, Deep mycoses and palatal perforation with granulomatous pansinusitis in acquired immunodeficiency syndrome: case reportsQuintessence Int 1993 24(10):743-48. [Google Scholar]
[2]. JC Smith, A Kacker, VK Anand, Midline nasal and hard palate destruction in cocaine abusers and cocaine’s role in rhinologic practiceEar Nose Throat J 2002 81(3):172-77. [Google Scholar]
[3]. CB Fowler, JF Nelson, DW Henley, BR Smith, Acquired immune deficiency syndrome presenting as a palatal perforationOral Surg Oral Med Oral Pathol 1989 67(3):313-18. [Google Scholar]
[4]. K Al-Sebeih, K Karagiozov, A Jafar, Penetrating craniofacial injury in a pediatric patientJ Craniofac Surg 2002 13(2):303-07. [Google Scholar]
[5]. E Bartlett, RC Mahabir, CN Verheyden, Traumatic palatal perforation after orotracheal intubation: a case report and a review of the literatureCleft Palate Craniofac J 2013 50(5):614-17. [Google Scholar]
[6]. R Kumar, S Mehta, R Kalra, American Diabetes Association. Diagnosis and classification of diabetes mellitusDiabetes Care 2010 33:62-69.Suppl 1 [Google Scholar]
[7]. SE Geerlings, AI Hoepelman, Immune dysfunction in patients with diabetes mellitus (DM)FEMS Immunol Med Microbiol 1999 26(3-4):259-65. [Google Scholar]
[8]. McMurry AS Kashyap, F James, Wound healing with diabetes mellitus: better glucose control for better wound healing in diabetesSurgical Clinics of North America 1984 64(4):769-78. [Google Scholar]
[9]. B Mealey, Diabetes and periodontal diseases ReviewCorrected and republished in: J Periodontol 2000 71(4):664-78. [Google Scholar]
[10]. BS Saunders, D Easa, RJ Slaughter, Acquired palatal groove in neonates. A report of two casesJ Pediatr 1976 89(6):988-89. [Google Scholar]
[11]. R Bhowate, A Dubey, Nasotracheal intubation: an unusual cause of palatal perforation in an insulin dependent diabetes mellitus patientJ Clin Pediatr Dent 2004 29(1):79-81. [Google Scholar]
[12]. GM Angelos, DR Smith, R Jorgenson, EA Sweeney, Oral complications associated with neonatal oral tracheal intubation: a critical reviewPediatr Dent 1989 11(2):133-40. [Google Scholar]