An Unusual Case of Eosinophilia
Aashika Sunil Janwadkar1, Jitendra Rajendra Ingole2
1 Intern, Department of Internal Medicine, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
2 Professor, Department of Internal Medicine, Smt. Kashibai Navale Medical College and General Hospital, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aashika Sunil Janwadkar, 201, Suprabhat, Jeevan Vikas Kendra Marg, Andheri East, Mumbai-400069, Maharashtra, India.
E-mail: aashika.janwadkar@gmail.com
Various inflammatory markers have been used to show an association between welding and respiratory tract disorders due to inhalation of fumes. We hereby present a case of 19-year-old male, welder by occupation who presented with upper respiratory tract infection and was documented to have persistent moderate eosinophilia on serial Complete Blood Count (CBC) examination. This was also confirmed by bone marrow examination which was suggestive of increased eosinophilic precursors. Eosinophils are an inflammatory marker and are increased most commonly in respiratory tract of welders due to inhalation of metal fumes. Treatment with steroid is gratifying and provides short term symptomatic relief. Avoidance of metal fumes and/or change of job is the long term preventive measure. Welding occupation, as a risk factor, should be considered for causation of persistent respiratory tract inflammation with eosinophilia.
Metal fumes, Occupational hazards, Welders
Case Report
A 19-year-old male patient presented with chief complaints of fever and joint pain since two days which was gradual in onset and progressive in nature. The symptoms did not relieve by NSAIDs. There were no aggravating factors. There was no history of vomiting, cough, cold, bleeding manifestations or difficulty in breathing. The patient was admitted to the ward. After admission, the patient had fever for three days (fever spike of 104°F for two days) and thereafter the symptoms were relieved.
The patient had a past history of similar complaints one and a half month back. No other major surgical and medical past history was present.
The patient had normal bowel and bladder movements, no change in appetite or sleep patterns. No history of any addictions. The patient is a welder by occupation and performs shielded metal arc welding. He gave the history of using face mask but the face mask does not give full protection. The gases produced during welding are inhaled by the patient giving rise to burning of eyes, photophobia, running nose and sneezing. Family history was non contributory.
Patient came with outside laboratory report of CBC examination which was suggestive of eosinophilia (E-30.33%) with absolute eosinophil count of 2142 /cumm. He was referred for further management to our institute.
On admission, the patient was febrile with temperature of 104o F with tachycardia (HR=108 beats/min). Other vital parameters were within normal limits. No evidence of pallor, cyanosis, clubbing or lymphadenopathy was noted. Systemic examination was unremarkable.
Peripheral blood count showed the result as shown in [Table/Fig-1].
Peripheral blood count results.
| Day | Haemoglobin (g/dl)(N-12-17 g/dl) | RBC count (×106/μl)(N- 4.2-6.1 ×106 μl) | Total WBC count(N-4500-10,000) | Neutrophils (×103/μl)[N- 2.0-7.0×10μ9/l (40–80%)] | Lymphocytes (×103/μl)[N- 1.0-3.0×10μ9/l (20–40%)] | Monocyte (×103/μl)[N- 0.2-1.0×10μ9/l (2–10%)] | Eosinophils (×103/μl)[N- 0.02-0.5×10μ9/l (1%–6%)]Absolute Eosinophilic Count (AEC)(N- 30-350) | Basophils (×103/μL)[N- 0.02-0.1×10μ9/l (< 1–2%)] | Platelets (×106)(N-1.50 -4.50×106) |
|---|
| First | 13.3 | 4.61 | 9720 | 5 (51.5%) | 1.21 (12.4%) | 0.31 (3.2%) | 3.14 (32.3%)AEC=3139 | 0.06 (0.6%) | 1.53 |
| Fourth | 13.5 | 4.70 | 6340 | 1.73 (27.3%) | 2.12 (33.4%) | 0.19 (3.0%) | 2.29 (36.1%)AEC=2288 | 0.01 (0.2%) | 1.35 |
| Fifth | 14.3 | 5.01 | 7580 | 1.81 (21.7%) | 1.92 (23%) | 0.34 (4.1%) | 4.27 (51.1%)AEC=2122 | 0.01 (0.1%) | 1.36 |
RBC morphology: Normocytic normochromic RBC. Reticulocyte count was 0.1%. Stool examination and urine routine microscopy was normal, no parasite detected in stool. Serum chikungunya antibodies level was negative.
Renal function test (blood urea, serum creatinine and serum electrolytes) and liver function test (bilirubin, SGOT and SGPT) were within normal limits. Filarial antigen test was negative and chest X-ray was normal.
Serial CBC counts were suggestive of moderate eosinophilia [1]. In view of persistent eosinophilia on CBC examination, bone marrow examination was done to rule out underlying hematological conditions such as eosinophilic leukemia.
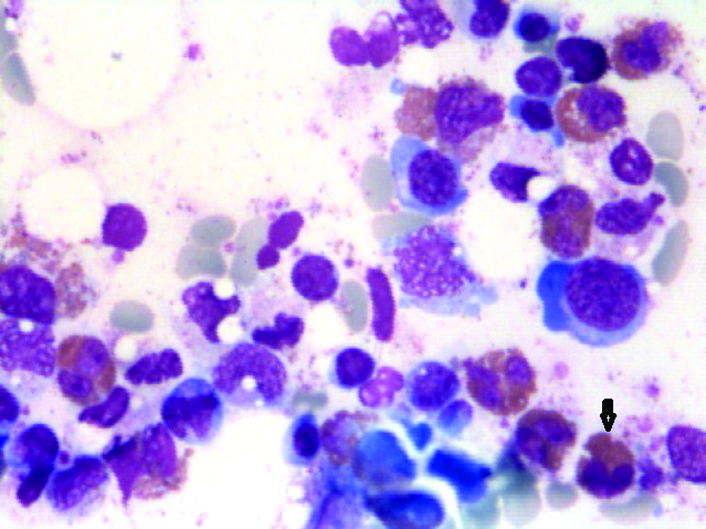
The bone marrow examination showed increased eosinophilic precursors with marrow showing normoblastic maturation along with normal cellularity with myeloid: erythroid ratio of 2:1. [Table/Fig-2] shows the photomicrograph of bone marrow smear showing eosinophils and its precursors. The arrow points at a mature eosinophil.
Eosinophils and its precursors.
Arrow: mature eosinophil
The patient was treated with oral prednisolone in dose of 1mg/kg/day and was significantly relived of majority of symptoms within 10 days of admission. His steroid doses were tapered off and stopped in next few days. He took leave of absence from his job as welder and returned for follow up to hospital after one month. The repeat CBC and Absolute Eosinophilic Count (AEC) report was suggestive of resolution of eosinophilia.
Discussion
Welders are commonly exposed to the metal fumes and their inhalation cause common respiratory tract diseases. Even though the pathophysiology is unclear, it has been documented that welders commonly suffer from respiratory tract infection [2]. Workers developing this condition often do so within the first 1-2 years of exposure [3]. If the condition is not treated there is decline in pulmonary function test. The following inflammatory markers: interleukin-8, tumour necrosis factor-α, myeloperoxidase, matrix metalloproteinase-9, immunoglobulin IgA and α2-macroglobulin, are increased in inflammation caused due to exposure to metal fumes in welders; which in turn causes elevation in counts of eosinophils and basophils [2]. A study suggested that eosinophils are commonly present in the peripheral tissue where mucosal-environment interface is present [4].
Metal fumes contain elements like oxides which are responsible for the respiratory symptoms (also known as metal fume fever). The fumes cause oxidative damage at the mucosal-environmental interface of the respiratory tract, thus inducing eosinophilia.
Other major causes of eosinophilia are parasitic infections primarily with helminthes, manifests as gastrointestinal symptoms and significant eosinophilia. Negative history of worms in stool and the stool examination showing absence of ova and cyst negated the possibility of the helminthic infestation as the cause [5]. Other infective aetiologies are fungal infections (allergic bronchopulmonary aspergillosis, coccidiomycosis). Absence of immunocompromising conditions, normal chest x-ray suggested other aetiology than fungal infection, in this patient.
Drug-associated eosinophilias (penicillins, cephalosporins) and atopic diseases are common examples of allergy associated eosinophilias and can be excluded from the diagnosis by a detailed medicine intake history. The patient, in this case, denied intake of any such medicines prior to development of the symptoms.
Leukemia (acute myelogenous leukemias most commonly, B-cell ALL), chronic eosinophilic leukemia and lymphomas (particularly Hodgkin’s, T- and B-cell lymphomas) are also one of the differentials and can be confirmed by typical findings following bone marrow examination.
Other conditions like graft-versus-host-disease (in transplant patients), primary immunodeficiency diseases (hyper IgE syndrome) and lung carcinoma (usually associated with smoking) have also shown association with increased eosinophilic count. These possibilities were ruled out in this patient by history and investigations performed.
Conclusion
Welding as an occupation is a potential risk factor for eosinophilia, due to toxic metal fumes generation. Since eosinophils are predominantly found in peripheral tissues such as the respiratory mucosa, it can be used as a chronic marker for occupational diseases due to inhalation.
[1]. Weller PF, The immunobiology of eosinophilsN Engl J Med 1991 324(16):1110-18. [Google Scholar]
[2]. Palmer KT, McNeill-Love RM, Poole JR, Coggon D, Frew AJ, Linaker CH, Inflammatory responses to the occupational inhalation of metal fumeEuropean Respiratory Journal 2006 27:366-73. [Google Scholar]
[3]. Nicholson P, Cullinan P, Newman T, Burge P, Boyle C, Evidence based guidelines for the prevention, identification, and management of occupational asthmaOccup Environ Med 2005 62(5):290-99. [Google Scholar]
[4]. Singh V, Gomez VV, Swamy SG, Vikas B, Approach to a case of eosinophiliaIJASM 2009 53(2):58-64. [Google Scholar]
[5]. Thomas B, Nutman MD, Evaluation and differential diagnosis of marked, persistent eosinophiliaImmunol Allergy Clin North Am 2007 27(3):529-49. [Google Scholar]