Maxillary Second Molar with Fused Root and Six Canals- A Case Report
Mitthra Suresh1, Kittappa Karthikeyan2, Sekar Mahalaxmi3
1 Reader, Department of Conservative Dentistry and Endodontics, Sree Balaji Dental College and Hospital, Bharath University, Chennai, Tamil Nadu, India.
2 Reader, Department of Conservative Dentistry and Endodontics, Srm Dental College and Hospital, SRM University, Ramapuram, Chennai, Tamil Nadu, India.
3 Professor and Head, Department of Conservative Dentistry and Endodontics, SRM Dental College and Hospital, Srm University, Ramapuram, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kittappa Karthikeyan, Reader, Department of Conservative Dentistry and Endodontics, SRM Dental College and Hospital, Srm University, Ramapuram, Chennai, Tamil Nadu, India. Email: dockarthicck@yahoo.com
One of the known aberrations in root canal morphology of maxillary second permanent molars is the presence of collateral mesiobuccal canals. This case report describes the endodontic management of a maxillary second molar that had a single fused root with six canals that was successfully managed with the aid of dental operating microscope. Six canal orifices were located namely MB1 (Mesiobuccal), MB2, MB3, DB1 (Distobuccal), DB2 and palatal. During the cleaning and shaping, instrument separation occurred at the apical third of the palatal canal which was removed with ultrasonics. After cleaning and shaping, the canals were obturated with resin sealer and laterally condensed gutta-percha. The patient was recalled for periodic review. After two years of follow up the patient remained asymptomatic. Cone Beam Computed Tomography (CBCT) evaluation revealed satisfactory periapical status.
Additional canals, Cone beam computed tomography, Dental operating microscope, Endodontic management, Root canal morphology
Case Report
A 20-year-old female patient reported with pain in the right upper back tooth region. The medical history was noncontributory. Clinical examination revealed a fractured class II temporary restoration in the permanent maxillary right second molar, with tenderness on percussion. On visualization of the pre-operative radiograph, a coronal radiopacity suggestive of the restorative material approximating the pulp with widening of the periodontal ligament space was observed in the specified tooth. On examination of the intra-oral periapical radiograph morphological variation of the root canal anatomy was not evident; however it revealed the presence of a fused root [Table/Fig-1a]. Based on clinical and radiographic evaluation, a diagnosis of symptomatic irreversible pulpitis with apical periodontitis in tooth number 17 (maxillary right second molar) was made.
The tooth was anaesthetized; and removal of the temporary restoration revealed secondary caries beneath the restoration. There was extensive loss of the coronal tooth structure, hence pre-endodontic composite build up was done and the tooth was isolated under rubber dam. The access cavity preparation revealed the orifices of four canals: two mesiobuccal, one distobuccal and one palatal. Since both mesiobuccal canals were far apart, anticipating an additional canal, the line between the two mesiobuccal canals was troughed with ultrasonic tip. This revealed another orifice midway between two mesiobuccal canals. Further probing of the groove along distobuccal canal revealed the presence of second distobuccal canal. The final access cavity revealed the presence of six canal orifices (three mesiobuccal, two distobuccal and one palatal) which was confirmed by visualization under the dental operating microscope (Seiler Revelation®, Seiler Instruments, St Louis, Missouri, USA) [Table/Fig-1b] [1].
Working length was determined using apex locator (Root ZX; Morita, Tokyo, Japan) and confirmed with radiograph. Cleaning and shaping was carried out using stainless steel K- files (Mani, Tochigi, Japan) till 2% 20 size followed by rotary ProTapers (Dentsply, Maillefer) till F2 size. Irrigation was done using 3% sodium hypochlorite solution throughout the procedure. During canal preparation, approximately 12mm length of ProTaper S1 rotary file separated at the apical portion of the palatal canal. The separated instrument was removed using ultrasonics under the operating microscope.
After completion of the canal preparation, calcium hydroxide (Apexcal, Ivoclar, Vivadent, AG FL – 9494 Schaan/Liechtenstein) intra canal medicament was given and the tooth was temporized with Cavit G (3M, ESPE, Seefeld, Germany). After one week, the canals were obturated with lateral condensation technique using AH plus resin sealer (Maillefer, Dentsply, Konstanz, Germany) & guttapercha points (Dentsply, Maillefer) [Table/Fig-1c]. This was followed by composite resin core build-up and a post endodontic metal ceramic restoration. The patient was recalled for periodic review. After two years of follow up [Table/Fig-1d] the patient remained asymptomatic. A CBCT evaluation at two years follow up revealed satisfactory periapical status [Table/Fig-2] [1].
(a) Pre-operative radiograph; (b) Phtograph showing the access cavity with six canal orifices in tooth 17 (maxillary right second molar); (c) Immediate post-operative radiograph; (d) Radiograph at two years follow up.

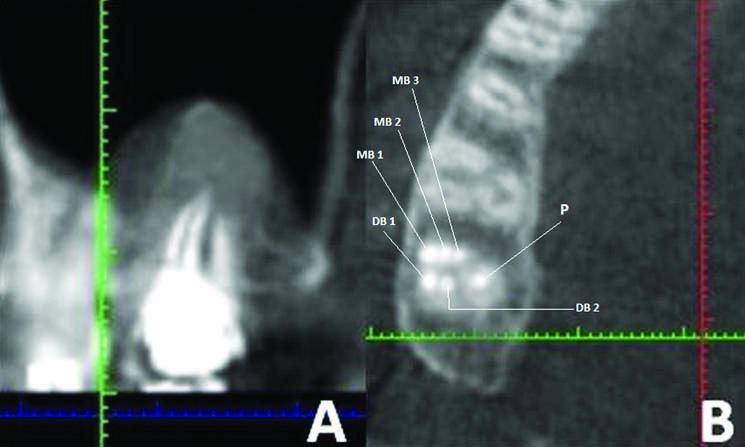
CBT images at two years follow up.
Some clinical studies and case reports of maxillary second molars with unusual canal morphology.
| Author name | Year | No. of canals | No. of teeth studied | Root Configuration | Canal anatomy details |
|---|
| Fahid & Taintor [7] | 1988 | 5 | 1 | 4 roots | separate DB roots with a separate apex |
| Christi WH et al., [12] | 1991 | 4 | 16 First and second molars | 4 roots | 2 palatal roots |
| Peikoff MD al., [8] | 1996 | 3,4,2,1 | 520 | 3,2,1,4 | 3 separate roots with 3 canals, 3 separate roots with 4 canals, 2 roots each with a single canal, 1 root with 1 canal, 4 roots with 4 canals |
| Zmener & Peirano [16] | 1998 | 4 | 1 | 4 roots | Three separated buccal roots |
| Fava LRG et al., [3] | 2000 | 1 | 4 | 1 roots | 1 root with a single canal |
| Alani AH et al., [6] | 2003 | 4 | 2 | 4 roots | 4 roots with 4 canals |
| Junior BP et al., [9] | 2007 | 6 | 1 | 4 roots | Three palatal root canals with a single palatal root |
| Kottoor J et al., [1] | 2010 | 5 | 1 | 5 roots | 5 roots with 5 root canals MB1, MB2, DB, DP(distopalatal) and palatal |
| Zhao J et al., [13] | 2011 | 5 | 1 | 4 roots | Three separate root canals (MB1, MB2, MB3) in a single MB root |
| Patel S & Patel P [14] | 2012 | 4 | 2 | 4 roots | Two separate palatal roots |
| Brito M Jr et al., [15] | 2013 | 5 | 1 | 5 roots | Three buccal roots (MB, mid-buccal, DB) |
| Zhang Q et al., [11] | 2014 | 3,4 | 187 | 3,4 roots | Three separate roots (57.7%) and fused roots (42.5%). Canal merging between: MB, DB canals (16 teeth)/ MB, DB/ P canals (9 teeth) |
| Zeng C et al., [10] | 2016 | 5 | 1 | 4 roots | MB root (C shaped) with 2 canals, 2 fused DB roots with 2 separate canals |
Discussion
Maxillary molars have three roots (96.2%) two buccal and one palatal [2]. The possible variations in the external root morphology in these teeth are extra root, fused roots or a single conical root. A tooth with a single conical root usually has a single large canal [3]; however, teeth with fused roots will definitely have more than one canal. Due to the extensive use of magnification and illumination aids, the incidence of extra roots and/or canals in the maxillary molars and their management has been extensively discussed in the literature [2-5].
So far the number of canals in maxillary second molar have been reported to vary from 1-6 [4-10]. Moreover occurrence of fused roots is more prevalent in maxillary second molars (42%) [10,11]. Morphological variations of the maxillary second molar in the number of roots and root canal anatomy reported by various authors has been summarized [Table/Fig-3] [1,3,6-16].
On comparison of the maxillary first, second and third molars, a considerable difference exists in between the degree of root separation and fusion. According to Percora and his researchers, among a total of 744 maxillary first, second and third molars observed, complete separation of all three roots was 86.4%, 75.9%, 18.8 % respectively. Whereas fusion of all three roots and fusion of only the buccal roots was 0.07%, 1.8%, 17.4% and 7.9%, 20.4%, 28.9% respectively [17].
The incidence of six canals in a maxillary second molar with a single root/fused roots has not been reported in the literature so far. This article presents one such case report. The canal configuration reveals one palatal, 3 mesiobuccal and 2 distobuccal canals. In the present case the preoperative radiograph showed the presence of conical root morphology, which can be single root or fused roots. Preoperative Radio Visio Graphy (RVG) images in different angulations did not give sufficient information about the number of root canals. The extra canals were identified by visualizing the bleeding spots under magnification, troughing with ultrasonic tips and probing with DG 16 explorer. Working length radiograph confirmed the presence of six canals.
Separation of endodontic files is a common incident during root canal treatment that prevents efficient cleaning and shaping of the root canal and may result in treatment failure [18]. During the canal preparation, rotary ProTaper instrument (S1) separated in the apical third of the palatal canal. This was removed by using ultrasonic equipment under high magnification.
Although CBCT is a diagnostic tool used for evaluating the root canal morphology [10,13,15], it was not used preoperatively since in the present case the initial radiographs indicated the presence of fused roots, but did not show any variation in the canal anatomy. As per the guidelines set by the American Association of Endodontists, CBCT is advocated only when conventional radiographs or other imaging techniques fail to disclose important diagnostic and clinical information. However, a postoperative CBCT analysis was performed when the patient reported for her second year follow up to confirm the root and canal morphology and to evaluate the periapical status [Table/Fig-2].
Conclusion
This unique case report gives an insight to yet another variation in the root and canal morphology of a maxillary second molar. Extra canals and/or roots can occur in any tooth and a tooth with single root may not always contain one canal. This is the first report that describes the endodontic management of a maxillary second molar with fused roots and six canals. Failure to locate and treat additional canals can adversely affect the outcome of endodontic therapy. Various adjuncts such as dental operating microscope and CBCT enable the clinician to perform endodontic treatment in a more precise and predictable manner.
Acknowledgements
I affirm that I/We have no financial affiliation (e.g., employment, direct payment, stock holdings, retainers, consultantships, patent licensing arrangements or honoraria), or involvement with any commercial organization with direct financial interest in the subject or materials discussed in this manuscript, nor have any such arrangements existed in the past three years. Any other potential conflict of interest is disclosed.
[1]. J Kottoor, S Hemamalathi, R Sudha, N Velmurugan, Maxillary second molar with 5 roots and 5 canals evaluated using cone beam computerized tomography: a case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod 2010 109:e162-65. [Google Scholar]
[2]. BM Cleghorn, WH Christie, CSC Dong, Root and root canal morphology of the human permanent maxillary first molar: a literature reviewJ Endod 2006 32:813-21. [Google Scholar]
[3]. LRG Fava, I Weinfeld, FP Fabri, CR Pais, Four second molars with single roots and single canals in the same patientInt Endod J 2000 33:138-42. [Google Scholar]
[4]. K Karthikeyan, S Mahalaxmi, New nomenclature for extra canals based on four reported cases of maxillary first molars with six canalsJ Endod 2010 36:1073-78. [Google Scholar]
[5]. JVB Barbizam, RG Riberiro, MT Filho, Unusual anatomy of permanent maxillary molarsJ Endod 2004 30:668-71. [Google Scholar]
[6]. AH Alani, Endodontic treatment of bilaterally occurring 4-rooted maxillary second molars: case reportJ Can Dent Assoc 2003 69:733-35. [Google Scholar]
[7]. A Fahid, JF Taintor, Maxillary second molar with three buccal rootsJ Endod 1988 14:181-83. [Google Scholar]
[8]. MD Peikoff, WH Christie, HM Fogel, The maxillary second molar: variations in the number of root and canalsInt Endod J 1996 29:365-69. [Google Scholar]
[9]. BP Junior, CDS Teixeira, RG Silva, LP Vansan, MDS Neto, Treatment of a second maxillary molar with six canalsAust Endod J 2007 33:42-45. [Google Scholar]
[10]. C Zeng, Y Shen, X Guan, X Wang, M Fan, Y Li, Rare root canal configuration of bilateral maxillary second molars using cone beam computed tomographic scanningJ Endod 2016 42:673-77. [Google Scholar]
[11]. Q Zhang, H Chen, B Fan, W Fan, JL Gutmann, Root and root canal morphology in maxillary second molar with fused root from a native Chinese populationJ Endod 2014 40:871-75. [Google Scholar]
[12]. WH Christie, MD Peikoff, HM Fogel, Maxillary molars with two palatal roots: a retrospective clinical studyJ Endod 1991 17:80-84. [Google Scholar]
[13]. J Zhao, Y Li, W Yang, PJ Wang, Y Meng, Three-dimensional computed topography analysis of a patient with an unusual anatomy of the maxillary second and third molarsInt J Oral Sci 2011 3:225-28. [Google Scholar]
[14]. S Patel, P Patel, Endodontic management of maxillary second molar with two palatal roots: a report of two casesCase Rep Dent 2012 2012:590406 [Google Scholar]
[15]. M Brito Jr, G Moreira Jr, JA Normanha, AL Faria-e-Silva, CC Camilo, RN Savioli, Midbuccal canals of maxillary molars evaluated by cone beam computed tomography: endodontic management of two casesBraz Dent J 2013 24:575-79. [Google Scholar]
[16]. O Zmener, A Peirano, Endodontic therapy in a maxillary second molar with three buccal rootsJ Endod 1998 24:376-77. [Google Scholar]
[17]. JD Pecora, JB woelfel, MDS Neto, Morphologic study of the maxillary molarsBraz Dent J 1991 2:45-50. [Google Scholar]
[18]. AA Madarati, AJE Qualtrough, DC Watts, A microcomputed tomography scanning study of root canal space: changes after the ultrasonic removal of fractured filesJ Endod 2009 35:125-28. [Google Scholar]