Among all gynaecological malignancies, ovarian cancers are the ones with the highest mortality rate. It is the sixth most common cancer in women worldwide. Surface epithelial stromal tumours form two thirds of all ovarian neoplasms and 90% of all ovarian cancers. Ovarian cancer is the third most common cancer among women in India [1].
Ovarian tumours present a great challenge to the gynecological oncologist. The diagnosis of ovarian masses is important for the surgeon to conserve the other ovary in young patients with benign tumours and early institution of chemotherapy in malignant tumours [2].
It is important to identify the prognostic factors and established clinicopathologic parameters that predict which patients are at high risk for tumour progression, as this is significantly helpful for better treatment and improvement of survival rate of patients with ovarian carcinoma [3].
For tumour growth and metastasis, angiogenesis is an essential phenomenon. VEGF, one of the key mediators of angiogenesis, promotes the proliferation, survival, and migration of endothelial cells and is essential for blood vessel formation [3]. With the recent advancement and better understanding of the molecular pathways which control tumour angiogenesis have led to the development of novel VEGF-targeting agents for the treatment of ovarian cancer [4]. Many agents have been used in clinical trials, and some of them have shown promising clinical activity against ovarian cancer [4]. The aim of our study was to see the expression of VEGF in the spectrum of various types of epithelial ovarian neoplasms by IHC and correlate it with histological grading and staging in malignant cases.
Materials and Methods
We conducted a cross-sectional, observational study from February 2015 to July 2016 in the Department of Pathology in association with Department of Gynaecology and Obstetrics of NRS medical college and hospital, Kolkata, West Bengal, India. In all 50 cases of surface epithelial ovarian tumours, diagnosed in our department were included in this study. Specimens of ovarian tumours were fixed for 24 hours in neutral buffered formalin (10%), dehydrated in alcohols, cleared in xylene and embedded in paraffin. Conventional 4μ thick sections were cut from the blocks and spread on clean, grease free glass slides. All the histological slides were stained with Hematoxylin and Eosin (H&E) and mounted with DPX. Blocks rich in tumour tissue were selected and marked. Sections were cut from the block and spread on poly-l-lysine coated slides for IHC. IHC was carried out manually by using a rabbit monoclonal VEGF antibody. On microscopic examination, positive staining for VEGF was observed as granular, brown cytoplasmic staining in the tumour cells.
The scoring was done by evaluating the intensity of cytoplasmic staining [Table/Fig-1] and the percentage of positive tumour cells [Table/Fig-2]. The two scores were added to get the final scores.
| Score | Intensity of cytoplasmic staining |
|---|
| 0 | Absent staining |
| 1+ | Mild staining |
| 2+ | Moderate staining |
| 3+ | Strong staining |
| Score | Percentage of positive tumour cells |
|---|
| 0 | <1% positive cells |
| 1 | 1-10% positive cells |
| 2 | 11-50% positive cells |
| 3 | 51-100% positive cells |
Based on the scores, the surface epithelial tumours were categorized as high VEGF expressors (Scores 5 and 6) and low VEGF expressors (Scores 4 and below) [5].
Statistical Analysis
Statistical analysis was done using appropriate statistical method and statistical significance and correlation was tested by using Pearson’s chi-square test and Spearman’s correlation test respectively.
Results
A total of 50 cases of ovarian surface epithelial ovarian neoplasms were studied. The age of the patients ranged from 17-70 years with a median age of 43 years. A 26 (52%) of the 50 cases were found in the age range of 40-59 years. The incidence of malignant neoplasms was significantly associated with increased age (p=0.032). Most of the patients presented with pelvic pain (32%) or abdominal pain (28%).
On gross examination, 21 (42%) of all the cases were of mixed solid and cystic consistency, 25 (50%) cases were cystic, out of which 26% were multiloculated and 24% were uniloculated, 4 (8%) cases were of solid consistency.
Of the 50 cases, there were 24 (48%) benign neoplasms, 4 (8%) borderline neoplasms and 22 (44%) malignant neoplasms. The findings related to the subtypes of neoplasms in these three categories have been included in [Table/Fig-3].
Distribution of ovarian tumours according to subtypes.
| Histological subtype | Number of cases | Percentage |
|---|
| Serous cystadenoma | 10 | 20 |
| Mucinous cystadenoma | 9 | 18 |
| Serous cystadenofibroma | 4 | 8 |
| Borderline mucinous tumour | 2 | 4 |
| Borderline serous papillary tumour | 1 | 2 |
| Borderline endometrioid tumour | 1 | 2 |
| Serous papillary cystadenocarcinoma | 14 | 28 |
| Mucinous cystadenocarcinoma | 5 | 10 |
| Endometrioid tumour | 2 | 4 |
| Benign Brenner tumour | 1 | 2 |
| Clear cell carcinoma | 1 | 2 |
| Total | 50 | 100 |
A total of 76.5% of all the carcinomas were high grade neoplasms, most of which were of serous papillary morphology. A 22.7% carcinomas presented in Stage I, 9.1% in Stage II and 45.5% in Stage III and another 22.7% cases in stage IV, having pleural effusion with positive cytology. Most of the serous carcinomas presented at later stages.
VEGF Expression in Epithelial Ovarian Neoplasms
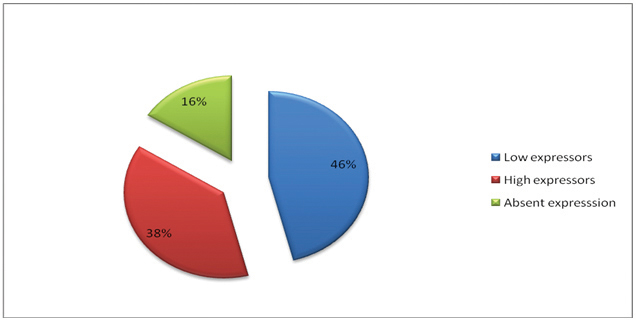
A total of 42 of the 50 cases (84%) of surface epithelial ovarian neoplasms were positive for VEGF [Table/Fig-4]. VEGF expression was significantly higher in carcinomas as compared to benign and borderline neoplasms (p=<0.001). Out of the 24 benign epithelial neoplasms, 18(75%) were low expressors and 6 (25%) had no expression of VEGF. There were no high expressors in the benign category. Among the four cases in borderline category, 2 (50%) cases were low VEGF expressors, one case showed high expression and there was no expression in another case. Among the 22 malignant cases, 18 (81.8%) were high expressors, only 3 (13.6%) were low expressors and expression was absent in one case.
VEGF expression in ovarian epithelial neoplasms.
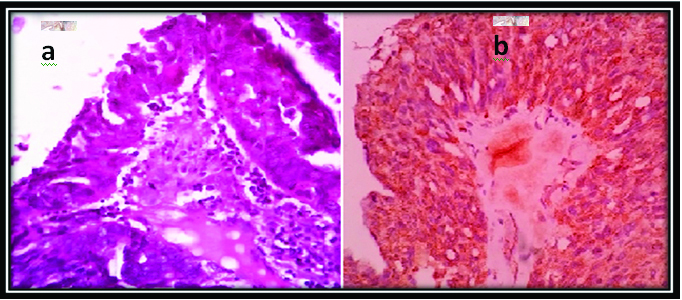
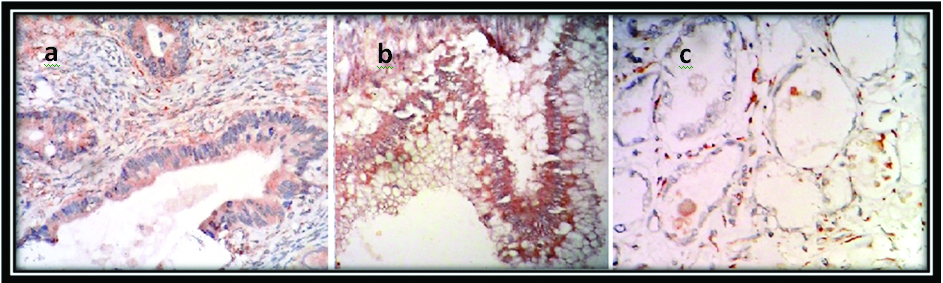
All the 11 cases of high grade serous papillary cystadenocarcinoma [Table/Fig-5], five cases of mucinous cystadenocarcinoma and two cases of endometrioid carcinoma showed high VEGF expression. VEGF expression was absent in clear cell carcinoma [Table/Fig-6].
(a) High grade serous papillary cystadenocarcinoma (H&E stain, 40X); (b) IHC with VEGF showing intense cytoplasmic expression in the tumour cells. (40X).
Positive VEGF expression in: (a) endometrioid carcinoma (IHC, 10X); (b) mucinous carcinoma (IHC, 10X) and absent expression in; (c) clear cell carcinoma (IHC, 40X).
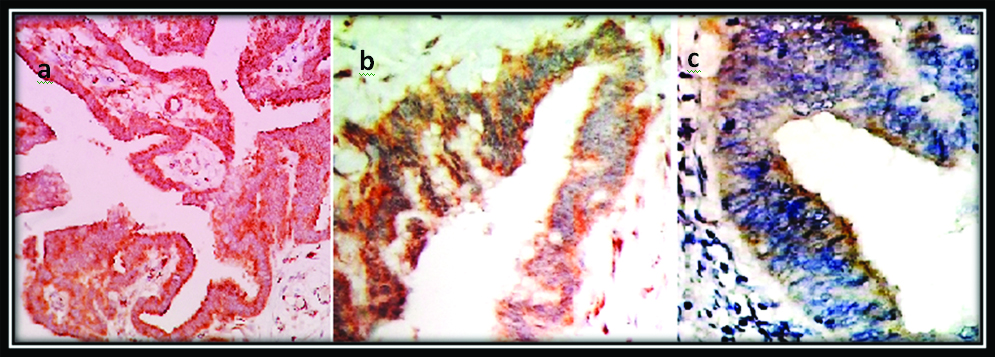
Among the low grade carcinomas, VEGF expression was low with one exception. Out of the borderline neoplasms, only borderline serous papillary neoplasms showed high expression of VEGF while borderline endometrioid tumour and one case of borderline mucinous tumour showed low expression [Table/Fig-7]. In the benign category, all the 10 cases of serous cystadenoma and four cases of serous cystadenofibroma were low expressors. Out of nine cases of mucinous cystadenoma, four cases were low expressors. Among the nine cases with absent VEGF expression, five were mucinous cystadenomas, one was a borderline mucinous tumour and there were one case each of benign brenner tumour and clear cell carcinoma [Table/Fig-8,9].
IHC showing high VEGF expression in: (a) borderline serous papillary tumour (IHC, 4X); and low VEGF expression in; (b) borderline mucinous tumour (IHC, 10X); and (c) borderline endometrioid tumour (IHC, 10X).
Distibution of VEGF according to histological type.
| Histologic type | Histological subtype | Lowexpressors | Highexpressors | Absent expression | Total |
|---|
| Benign | Serous cystadenoma | 10 | 0 | 0 | 10 |
| Mucinous cystadenoma | 4 | 0 | 5 | 9 |
| Serous cystadenofibroma | 4 | 0 | 0 | 4 |
| Benign Brenner tumour | 0 | 0 | 1 | 1 |
| TOTAL | 18 | 0 | 6 | 24 |
| Borderline | Borderline mucinous tumour | 1 | 0 | 1 | 2 |
| Borderline serous papillary tumour | 0 | 1 | 0 | 1 |
| Borderline endometrioid tumour | 1 | 0 | 0 | 1 |
| TOTAL | 2 | 1 | 1 | 4 |
| Malignant | Serous papillary cystadenocarcinoma | 3 | 11 | 0 | 14 |
| Mucinous cystadenocarcinoma | 0 | 5 | 0 | 5 |
| Endometrioid carcinoma | 0 | 2 | 0 | 2 |
| Clear cell carcinoma | 0 | 0 | 1 | 1 |
| TOTAL | 3 | 18 | 1 | 22 |
| TOTAL | 23 | 19 | 8 | 50 |
Distribution of VEGF according to morphology.
| Morphology | Subtype | Lowexpressors | Highexpressors | Absentexpression | Total |
|---|
| Serous | Cystadenoma | 10 | 0 | 0 | 10 |
| Cystadenofibroma | 4 | 0 | 0 | 4 |
| Borderline tumour | 0 | 1 | 0 | 1 |
| Cystadenocarcinoma | 3 | 11 | 0 | 14 |
| TOTAL | 17 | 12 | 0 | 29 |
| Mucinous | Cystadenoma | 4 | 0 | 5 | 9 |
| Borderline tumour | 1 | 0 | 1 | 2 |
| Cystadenocarcinoma | 0 | 5 | 0 | 5 |
| TOTAL | 5 | 5 | 6 | 16 |
| Endometrioid | Borderline tumour | 1 | 0 | 0 | 1 |
| Carcinoma | 0 | 2 | 0 | 2 |
| TOTAL | 1 | 2 | 0 | 3 |
| Clear cell | Carcinoma | 0 | 0 | 1 | 1 |
| Brennner | Benign | 0 | 0 | 1 | 1 |
| TOTAL | 23 | 19 | 8 | 50 |
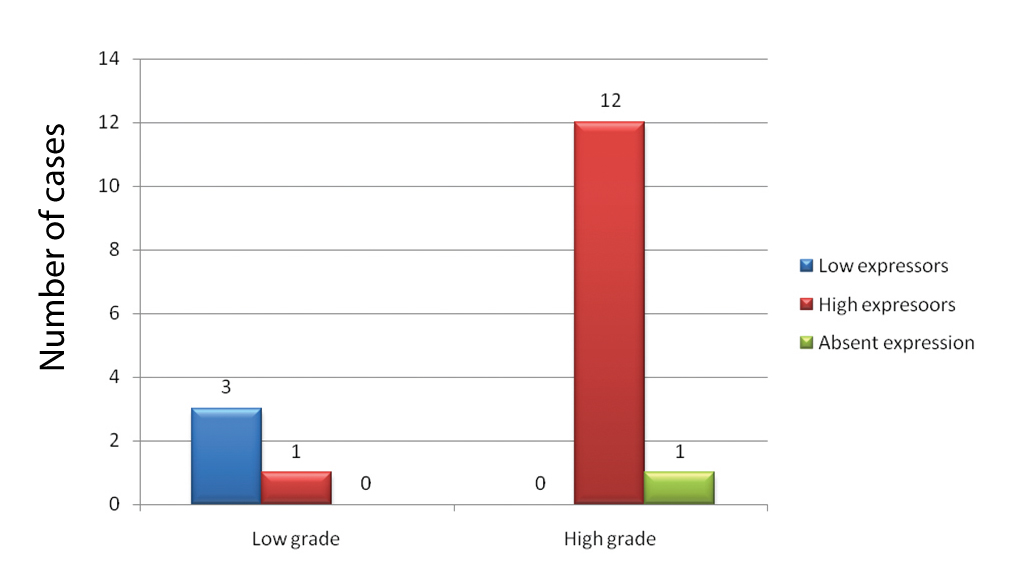
VEGF Expression and Histological Grade
A significant association (p=0.003) and a strong positive correlation (rho=0.764) was seen between grade of carcinomas and VEGF expression. In our study, 92% of the cases with high expression of VEGF were high grade neoplasms [Table/Fig-10]. VEGF expression was positive in serous morphology throughout the spectrum of cystadenoma, serous cystadenofibroma, borderline serous papillary tumour and serous cystadenocarcinoma.
Distribution of VEGF according to histological grade.
Test of significance: χ2=11.870; df=2;p =0.003
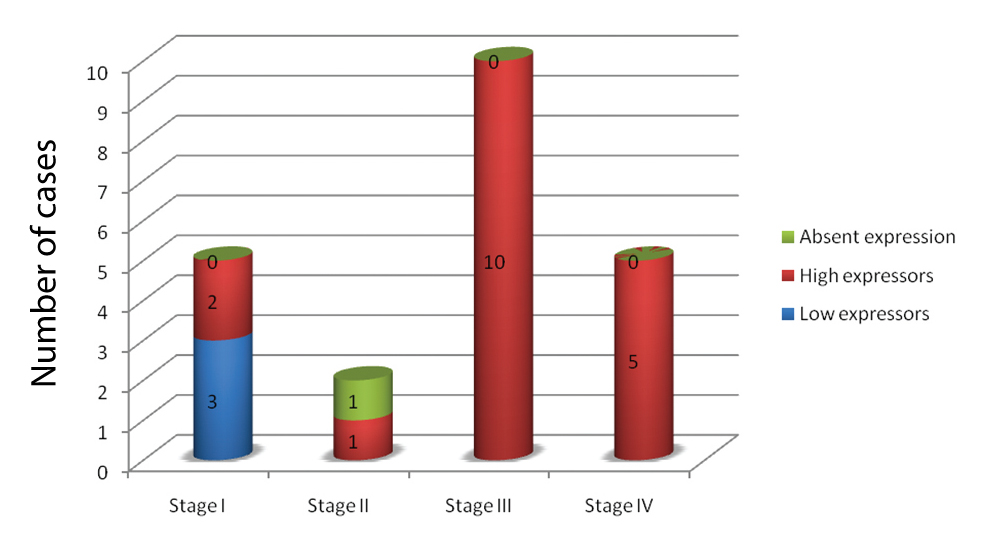
VEGF Expression and Stage
High VEGF expression was significantly associated with advanced stage of disease in our study (p-value=0.001). Positive correlation was also seen with stage but it was not statistically significant (rho-0.394, p=0.069). All the 10 cases of Stage III carcinomas and 5 cases of stage IV carcinomas with malignant pleural effusion were high expressors of VEGF [Table/Fig-11].
Distribution of VEGF according to stage of carcinomas.
Test of significance: χ2=22.122; df=6; p=0.001
Discussion
A tumour cannot grow beyond 2 mm diameter without neoangiogenesis [6], thus angiogenesis plays a major role in tumour growth, invasion, and metastasis [6,7]. The balance of pro and antiangiogenic factors regulates angiogenesis. “Angiogenic switch” i.e., the transition of a tumour from ‘avascular phase’ to ‘vascular phase’ is believed to be stimulated by an increase in expression of pro-angiogenic factors. VEGF is one such factor. Hypoxia is the major physiological stimulus for expression of VEGF and it develops within tumours when cancer cell proliferation exceeds rate of blood vessel formation. Hypoxia Inducible factor-1α (HIF-1α) is a transcriptional activator that acts as a central regulator of oxygen homeostasis. It also regulates the expression of VEGF and promotes angiogenesis [8].
A five year survival rate is more than 90% when the tumour is confined to the ovaries, whereas, when it extends to the intra-abdominal or retroperitoneal cavity, the survival rate decreases to 30% [9]. The prognostic factors for epithelial ovarian carcinomas include histological subtype, grading, surgical staging, lymph node metastasis and residual tumour after cytoreductive surgery [10].
We studied the expression pattern of VEGF in 50 cases of surface epithelial ovarian neoplasms. A 42 of the 50 cases (84%) of surface epithelial ovarian neoplasms showed VEGF expression. Out of the 22 malignant cases, 18 (81.8%) showed high VEGF expression. This finding is comparable to the study of Premalata et al., with 26 of 78 (33.3%) cases of primary malignant epithelial ovarian neoplasm showing high VEGF expression [5].
In our study, VEGF expression was significantly higher in carcinomas as compared to benign and borderline neoplasms (p-value<0.001). This finding was comparable to some studies like that of Yamamoto S et al., with positive immunostaining for VEGF in 97% (68 out of 70) of ovarian carcinomas, which was significantly higher than that of tumours of Low Malignant Potential (LMP) (13 out of 25; 52%) and benign cystadenomas (5 out of 15; 33%) (p < 0.01) [11]. Studies of Inan S et al., and Garzetti GG et al., also showed that VEGF immunostaining was higher in cases of cystadenocarcinomas than in borderline or benign neoplasms [12,13].
High grade serous carcinomas, mucinous cystadenocarcinomas and endometrioid carcinomas- all were high VEGF expressors in our study. This finding was different from Premalata CS et al., where low VEGF expression was seen in endometrioid, clear cell and mucinous morphology [5]. One case of clear cell carcinoma showed no VEGF expression in our study. This finding was different from Yamamoto S et al., where high VEGF expression was associated with clear cell morphology [11].
Serous carcinomas overwhelmingly expressed VEGF throughout the spectrum of benign, borderline and malignant neoplasms. A 9 (81.8%) out of 11 cases of serous carcinomas showed high VEGF expression with a score of 6. This finding is comparable to the study of Ravikumar G and Crasta JA where 35% of the ovarian serous carcinomas were high VEGF expressors with score of 6 [14].
A significant association was seen between grade of neoplasms and VEGF expression (p=0.003). Premalata CS et al., and Shen GH et al., also had similar findings with p-values 0.022 and 0.0004 respectively [5,15].
High VEGF expression was also significantly associated with advanced stage of carcinoma (p=0.001). This finding was similar to the studies of Premalata CS et al., (p=0.006), Yamamoto S et al., (p<0.05) and Shen GH et al., (p=0.002) all of which showed association between high stage and high VEGF expression [5,11,15].
Many other studies have reported the association between high VEGF expression and poor patient outcome. At present inhibitors of angiogenesis like bevacizumab are increasingly being used with success in carcinomas of lung, breast and colon and are being tried in refractory and recurrent cases of ovarian carcinoma [5].
Key messages from this study are:
Most ovarian epithelial cancers are dependent on VEGF for tumour progression.
Serous ovarian neoplasms express VEGF throughout the whole spectrum of benign, borderline and malignant neoplasms.
VEGF expression is significantly associated with grade and stage of ovarian tumours.
High VEGF expression is seen in high grade and advanced stage neoplasms and such patients could be selected for targeted anti-angiogenic therapy.
Limitation
Paucity of cases and limited time period were few limitations of our study.
Conclusion
Thus we conclude that, in our study, VEGF expression was seen in a significant number of the whole spectrum of benign, borderline and malignant ovarian epithelial neoplasms. High expression was seen in 45.2% cases, most of which were associated with carcinomas of serous morphology, high grade and advanced stage of disease. Mucinous and endometrioid carcinomas also highly expressed VEGF. We had a single case of clear cell carcinoma which in spite of being a high grade neoplasm did not express VEGF. More confirmatory evidence might be provided with increased number of cases.
Our findings reveal that most epithelial ovarian cancers are dependent on VEGF for tumour progression and may be useful to select patients and as well as predict the treatment response of ovarian carcinomas to targeted anti-angiogenic therapy.