Acrylic resin and acrylic polymers are commonly used as denture base materials in field of prosthodontics. The successful use of these materials is because of their ease of processing, cost effectiveness, light weight, and colour matching ability with oral mucosa. But they are brittle, less in strength and have low thermal conductivity [1]. Smith DC analysed the practical situation for fracture of dentures and showed two types of failure. Failure caused by impact forces, i.e., a high stress rate extra orally and failure usually in function; this is probably a fatigue phenomenon, i.e. a low and repetitive stress rate intra orally [2]. The need to improve the strength of the denture base has been addressed by chemical modification of poly methyl-methacrylate through the addition of rubbers, fibers and metal powder fillers [3]. In the past research several metal fillers like tin oxide, silver powder and zirconium oxide have been used to improve physical properties of acrylic resins. However, the use of metal powder filler has caused the dentures to be unaesthetic [4]. There is a need for an ideal metal powder that can be incorporated into the resin which increases strength; without affecting other properties. Hence this study was undertaken to find out the effect of adding aluminum oxide powder on the flexural strength of acrylic denture base material.
Materials and Methods
The present in vitro study assessed the flexural strength of different types of denture base resins and was conducted in KLES Institute of Dental Sciences, Bangalore, India. Metal rectangular bar measuring 65 x 10 x 3 mm3 was fabricated in accordance with ADA specification No. 12 for denture base polymers [5] and was invested in the flask with dental stone [Table/Fig-1]. After setting of the dental stone, the flask was opened and the metallic bars were removed, leaving rectangular shaped mould cavity in the dental stone, which was used as matrix for the fabrication of different types of acrylic resin beam specimens [Table/Fig-2]. Separating medium was applied to stone mould.
Metal rectangular bar invested in dental stone.

Rectangular shaped mould cavity. (Images from left to right)

Preparation of Test Samples
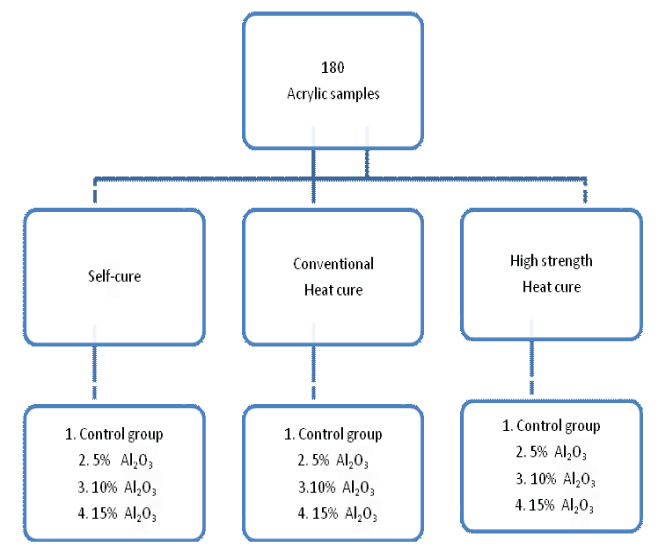
A total of 180 samples were divided into three groups randomly by lottery dip technique, which was further divided into four subgroups with 15 samples in each subgroup. A total of 15 acrylic samples, each of conventional heat-cure, high strength heat-cure and self-cure acrylic resins were taken as control group [Table/Fig-3].
Flow chart showing sampling design.
Acrylic specimens were made by reinforcing aluminum oxide powder 5%,10%,15% by weight to conventional heat-cure polymerizing resin (HC) (Trevlon, Dentsply), High strength heat-cure polymerizing resin (TrevlonHI, Dentsply) and self cure polymerizing resin (Trevlon, Dentsply). Simple mixing of Al2O3 powder fillers with resin powder and liquid monomer resulted in even distribution of filler within the polymer matrix [1]. For 50 gm of polymer powder, 2.5 gm, 5 gm and 7.5 gm of Al2O3 filler was added to get 5%, 10% and 15% of reinforced polymer powder. Electronic weighing machine was used to add alumina powder in different concentrations. Packing and processing was done according to manufacturer’s instructions using compression molding technique at 740C for two hours and increasing the temperature of water bath to 1000C for one hour. Flasks were allowed to cool to room temperature before opening. The rectangular specimens were deflasked, excess acrylic resin was removed by trimming the edges with tungsten steel burs using a hand piece at low speed and with additional hand smoothening using sand paper [Table/Fig-4]. All the specimens were stored in distilled water for one week before flexural strength testing.
Flexural Strength Testing
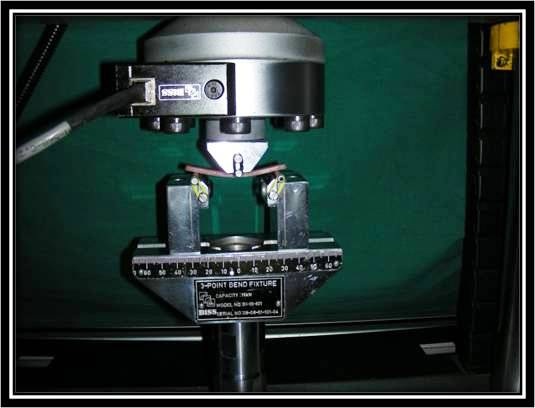
Flexural strength of the specimen was determined using a 3-point bending testing device in a universal testing machine (Instron) [1] [Table/Fig-5]. Flexural strength was calculated using the following equation [1] S=3PI/2bd2 Where S=flexure strength (N/mm2), P=load at fracture (N), I=distance between the supporting wedges (mm), b=width of the specimen (mm) and d=thickness of the specimen and width of each specimen was checked by using caliper device.
3-point bend fixture with specimen.
Statistical Analysis
One-way analysis of variance ANOVA test was done to evaluate the results in between the groups and post-hoc Tukey paired group comparison tests to within the group. A p-value less than 0.05 was considered to be statistically significant.
Results
The mean flexural strength in Megapascals (MPa) of the acrylic resins self cure acrylic (SC), Heat cure acrylic resins (HC) and high strength heat cure acrylic resins (HI) with aluminum oxide at different concentrations (5%, 10% and 15%) was compared using one-way analysis of variance (ANOVA) technique. There was a overall statistically significant difference found in flexural strength of self cure acrylic resin, conventional heat cure acrylic resin and high impact heat cure acrylic resin with different concentrations 5%, 10% and 15% compared to control group [Table/Fig-6]. On post-hoc analysis, there was no statistically significant difference in flexural strength between 5% and 10% and 10% and 15% subgroup except for HC group in which significant difference was found between 5% and 15% subgroups [Table/Fig-7].
Intra-group comparison of mean flexural strength (MPa) of different types of resins at different concentrations of alumina powder.
| SCMean (SD) | HCMean (SD) | HIMean (SD) |
|---|
| Control | 78.24 (7.89) | 90.84 (7.99) | 101.56 (5.73) |
| 5% | 85.15 (7.20) | 98.41 (7.25) | 123.21 (8.38) |
| 10% | 88.39 (4.68) | 105.04 (7.73) | 128.62 (10.00) |
| 15% | 93.58 (3.26) | 108.44 (5.60) | 131.05 (10.13) |
| p-value < 0.001 | p-value <0.001 | p-value <0.001 |
NOVA analysis; p-value less than 0.05 was considered statistically significant.
Pair wise comparison of flexural strength (MPa) with different concentration of alumina and SC, HC, HI.
| Pair wise comparison | SC | HC | HI |
|---|
| MeanDifference(p-value) | MeanDifference(p-value) | MeanDifference(p-value) |
|---|
| Control Vs 5% | -6.91(0.015*) | -7.57(0.028*) | -21.65(<0.001*) |
| Control Vs 10% | -10.15(<0.001*) | -14.20(<0.001*) | -27.06(<0.001*) |
| Control Vs 15% | -15.34(<0.001*) | -17.60(<0.001*) | -29.50(<0.001*) |
| 5 % Vs 10% | -3.24(0.464) | -6.62(0.068) | -5.41(0.336) |
| 5% Vs 15% | -8.44(0.464) | -10.03(0.002*) | -7.84(0.078) |
| 10% Vs 15% | -5.19(0.099) | -3.40(0.571) | -2.43(0.871) |
* p-value less than 0.05 was considered to be statistically significant
Post-hoc tukey test.
Addition of 15% alumina powder to self cure resin showed high flexure strength i.e., 93.58 Mpa and was comparable to the control group of conventional heat cure resin i.e., 90.84 MPa. Addition of 10% alumina powder to conventional heat cure resin shows high flexural strength i.e., 105.04 MPa and was comparable to the control group of high strength heat cure acrylic resins i.e., 101.56 MPa [Table/Fig-8].
Inter-group comparison of mean flexural strength (MPa) in three groups of acrylic resins.
| Control Alumina | 5% Alumina | 10% Alumina | 15% Alumina |
|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) |
|---|
| SC | 78.24 (7.89) | 85.15 (7.20) | 88.39 (4.68) | 93.58(3.26) |
| HC | 90.84 (7.99) | 98.41 (7.25) | 105.04 (7.73) | 108.44(5.60) |
| HI | 101.56 (5.73) | 123.21 (8.38) | 128.62 (10.00) | 131.05(10.13) |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 |
ANOVA analysis; p-value less than 0.05 was considered to be statistically significant.
Flexural strength of high strength acrylic resin was significantly higher than self cure and conventional heat cure acrylic resin. Flexural strength of conventional heat cure acrylic resin was significantly higher than self cure acrylic resin with addition of alumina in different concentrations [Table/Fig-9].
Pair wise comparison of flexural strength (MPa) of three different acrylic resins with alumina.
| Pair wise comparison | Control | 5% Alumina | 10% Alumina | 15% Alumina |
|---|
| MeanDifference(p-value) | MeanDifference(p-value) | MeanDifference(p-value) | MeanDifference(p-value) |
|---|
| SC Vs HC | -12.60 (0.001) | -13.26 (0.001) | -16.64 (0.001) | -14.85 (0.001) |
| SC Vs HI | -23.32 (0.001) | -38.06 (0.001) | -40.23 (0.001) | -37.47 (0.001) |
| HC Vs HI | -10.72 (0.001) | 24.80 (0.001) | -23.58 (0.001) | -22.61 (0.001) |
Post-hoc tukey test.
Discussion
Various studies have been reported in dental literature pertaining to the reinforcement of poly (methylmethacrylate) with various types of fibers and fillers in order to improve its mechanical properties. Reinforcement has been achieved through inclusion of polyaramid fibers [6], carbon fibers [7], glass fibers [8-10], ultra high modulus polyethylene fibers [11], chopped PMMA fibers [12], metal powders [13-16], sapphire whiskers [1,17] and zirconia oxide [18].
Study by Zappini G et al., showed that evaluating the strength of acrylic resins rely mainly on impact strength and this may not simulate the clinical conditions [19]. Flexural strength tests are in fact better than impact strength tests to predict clinical function [18]. Arnold AM et al., have reported that the ultimate flexural strength of a material reflects its potential to resist catastrophic failure under a flexural load [20]. Previous studies done by Ellakwa AE et al., Asar NB et al., Arora N et al., and Marel et al., demonstrated increase in flexural strength by adding metal oxides (alumina, tin, silver and zirconia) and sapphire whiskers [1,18, 21, 22]. Several studies in past also showed that addition of metal oxides (alumina, silver) decreased the tensile strength of acrylic resins [13,18,23]. Studies done in past used different types of resins from different manufacturers. In the current study, alumina oxide powder of 5%, 10% and 15% by weight was added to self-cure; conventional heat-cure and high strength heat cure acrylic resin manufactured by single manufacturer. Simple mixing of Al2O3 powder fillers with resin powder and liquid monomer resulted in even distribution of filler within the polymer matrix [1]. Ceramic filler (Alumina) was preferred over other metal fillers because of lower filler density {the density of alumina (3.99g/cm3) is considerably less than that of other metal fillers i.e., Co (8.9) and Cr (7.1)}[1]. Thus, the light weight of acrylic resin denture bases was retained. Also, the ceramic fillers have the advantage of being more cost-effective and white in colour so less likely to alter the finished appearance of the denture base material than other metal fillers. Results showed that there was statistically significant increase in flexural strength of self-cure group, conventional heat cure group and high strength heat cure group after adding alumina oxide powder 5%, 10% and 15% by weight compared to control group. Study by Zuccari AG et al., showed similar results in which Al2O3, magnesium oxide (MgO) and zirconium oxide (ZrO2) powders were used to reinforce the self-cured acrylic resins to fabricate provisional fixed restorations [24]. In the present study, flexural strength increased with increasing concentration of alumina by 5% to 15%. There was no significant difference between 5% and 10% and between 10% and 15% group. The present study showed that flexural strength of self cure resin can be increased to that of conventional heat cure resin by adding alumina powder. Self cure resin is used for the repair of denture bases and they have low flexural strength compared to conventional heat cure resin. Addition of alumina powder to self cure resin will improve its flexural strength to that of conventional heat cure resin. Similarly, flexural strength of conventional heat cure resin can be increased to that of high strength heat cure resin by adding 10% of alumina powder. In cases, where there is frequent fracture of denture bases due to high masticatory load or repair of denture base is needed, the flexural strength can be improved by adding alumina powder to heat cure and self cure acrylic resin, so as to increase the clinical success of prosthesis.
Limitation
The limitations of this study were that, as this was an in vitro study, material fatigue by thermocycling in water or artificial saliva with or without reinforcement was not carried out to predict the success of material or procedure in a clinical environment. Further research is needed to quantify the filler distribution within the polymer matrix. Also, it must be noted that surface treatment and use of silane coupling agents could be done to enhance the bonding between the filler particles with the resin matrix.
Conclusion
The results of this study conclude that addition of aluminium oxide powder 5%, 10% and 15% by weight to self cure acrylic resin; heat cure acrylic resin and high strength heat cure acrylic resin results in increase in flexural strength of different types of acrylic resins. The flexural strength of the self cure acrylic resin by adding 15% of aluminium oxide powder was comparable to that of conventional heat cure resin and also the flexural strength of conventional heat cure acrylic resin by adding 10% of aluminium oxide powder was comparable to that of high strength heat cure acrylic resins. Increase in flexural strength will increase long term success of the prosthesis.
NOVA analysis; p-value less than 0.05 was considered statistically significant.
* p-value less than 0.05 was considered to be statistically significant
Post-hoc tukey test.
ANOVA analysis; p-value less than 0.05 was considered to be statistically significant.
Post-hoc tukey test.