Dental Avengers: Taking Retainer Stability and Aesthetics into Next Era
Sayam Patil1, Sanjeev Jakati2
1 Reader, Department of Orthodontics, Tatyasaheb Kore Dental College and Research Centre, Kolhapur, Maharashtra, India.
2 Senior Lecturer, Department of Orthodontics, Swargiya Dadasaheb Kalmegh Smruti Dental College and Hospital, Nagpur, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sanjeev Jakati, Flat no 201, Susheela Appartments, Ganesh Colony, Sangam Road, Wanadongri, Hingna, Nagpur-441110, Maharashtra, India.
E-mail: sanjeevjakati@gmail.com
Adult patients are realizing that practical, realistic options now exist to “straighten” their teeth because the cosmetic dentistry revolution has begun to include even “adult short-term cosmetic orthodontics” as an integral part. Previously, the patients were bound to select between either the aesthetic benefits of ceramic or the bondability characteristic of composite, however this can now be fabricated in such a manner that still allows placement of a lingual splint so as to steady the orthodontic movement. This article describes a case study whereby the patient can attain the aesthetic benefits of an all ceramic crown or a veneer which was retained by incorporating/reinforcing a metal framework of crown itself. Orthodontic treatment was initiated to correct the alignment, overjet and overbite which were followed by endodontic, periodontic and prosthodontic rehabilitation with full ceramic crowns to achieve ideal aesthetics, and an improved occlusion and stable function.
Interdisciplinary, Multidisciplinary Dentistry, Crown, Retainer, Retention
Case Report
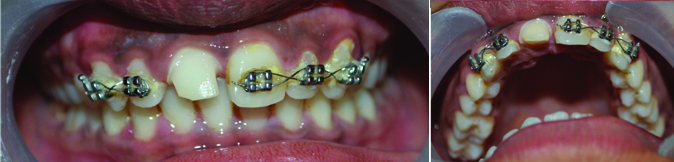
An 18-year-old male patient reported to the clinic with a chief complaint of crowding in upper arch. The patient had no relevant medical history but gave a history of fall from a motorcycle one year back. On intraoral examination Ellis Class II fracture was observed in relation to upper right central incisor #11. The left permanent maxillary canine #23 was placed high (labially and apically). The patient had Angle’s Class II Div 1 subdivision molar relation [Table/Fig-1]. A diagnosis of Angle’s Class II Div 1 Malocclusion was established. Treatment objectives were to achieve proper alignment, ideal overbite and overjet, perfect soft tissue drape as well as to restore the fractured tooth #11 and maintain its stability.
Pretreatment Intraoral view.

Treatment Procedure/Clinical Steps
The patient was presented with a couple of options before the start of treatment. The first one included the conventional orthodontic treatment followed by restoration of the tooth #11, which would take a minimum of two years at least. The second option provided was six month smile treatment followed by restoration of tooth #11. The procedures of both the treatments were informed to the patient and his parents before commencing all the steps in detail. The patients were concerned about the treatment time frame and hence chose the second option. Very few case studies are available regarding this protocol both in print and on the web. Hence they were shown cases from the website www.6monthsmiles.com. Through this all their queries were clarified. Consent was obtained and the treatment was started. Chronologically the steps included:
1. Teeth were aligned via six month smile orthodontic braces [1] protocol. In the first appointment, records were taken which include extraoral and intraoral photographs, impression of dental arches, orthopantomograms and lateral cephalograms. In the second appointment, MBT brackets were bonded in both arches and 0.014 NiTi wire was placed. The next appointment was scheduled after a week, during which fixed jack screw was placed for expansion and to create space in the maxillary arch. In the next appointment after 15 days, NiTi wire was engaged in the highly placed canine. Before the next appointment which was scheduled after a month, the canine had drifted downwards and all other teeth were aligned in unison. Space was maintained for the width of the crown at the right upper central incisor region i.e., #11. Overjet of 2 mm was maintained in the anterior region.
During the nest visit, pulp testing showed a non vital right upper central incisor i.e., #11 and hence intentional single sitting Root Canal Treatment (RCT) was done [Table/Fig-2].

In the next visit, orthodontic extrusion of the tooth #11 was done by placing the bracket gingival to its original position and crown lengthening procedure was carried out by the periodontist to help in alignment and crown preparation [Table/Fig-3].
Orthodontic extrusion, crown lengthening, crown preparation.
After another month, in the next appointment, prosthodontist did crown preparation with respect to full ceramic crown for the tooth #11 [Table/Fig-3].
A rubber base putty impression was taken with the brackets still on and sent to the lab with instructions to fabricate a porcelain crown on the tooth #11 within the width of the crown space created during step one.
Placement of a ceramic crown would hinder the durability and stability of the composite lingual retainer. Hence it was decided to include the retainer within crown design [Table/Fig-4]. Within a week the same was delivered by the lab.

In the next appointment, after bracket debonding and polishing of all the teeth, the crown was cemented to the tooth #11 along with its lingual metal retainer designed to be locked with the proximal undercuts [Table/Fig-5].
Post-treatment intraoral view.

This entire treatment procedure was completed within a short time of nine months with stable results. Even though the level of aesthetics achieved can be considered as sub standard according to many “text book practitioners”, but the patient was completely satisfied with the level of aesthetics achieved and he wasn’t in the favour of still prolonged orthodontic treatment to achieve the best text book finish. The extraoral pre and post-treatment photos were inconclusive, but sufficient degree of makeover was visible in the intraoral pre and post-treatment photographs [Table/Fig-1,5].
Discussion
Recently the cosmetic dentistry revolution has begun to include even “adult short-term cosmetic orthodontics” as an integral part of its development and future. Many people have concurrent mild to moderate orthodontic problems often associated with other aesthetic problems and this can’t be corrected by orthodontics alone. One of these conditions commonly observed is the missing, malformed or fractured teeth, which require fabrication of permanent prosthesis using ceramic and its substitutes. Previously one had to compromise in terms of choosing between aesthetic benefits of ceramic or the bondability of composite [2,3]. But modern technological advances now allow these prosthetic designs to be fabricated in a way that allows placement of a lingual splint into the orthodontic retainer design itself.
With the ever challenging demand of the patients to an aesthetically and functionally stable treatment result, the trend in dentistry is shifting from super specialisation to team approach. The role of orthodontist in such an interdisciplinary treatment approach can be primary or secondary [4]. Primary consists of cases like those requiring tooth build up to match a Bolton discrepancy, missing teeth, periodontal rehabilitation, surgical exposure of an impacted tooth, etc., [4], while secondary consists of cases where the orthodontic treatment is provided an adjunct to other treatments designed [4].
In our above mentioned case, patient was administered the benefits of full ceramic crown, which was retained for practical and conservative purposes, by incorporation of the metal frame work of the crown directly into the retainer, instead of the traditional lingual composite-Ribbond splint. The customised meshwork design also aids as a permanent post orthodontic retainer and simultaneously maintains the aesthetic quality of smile. Orthodontic therapy aided the restoration and reconstruction of the fractured tooth. Because the tooth preparation design for full ceramic crown encroached on the biological width, orthodontic extrusion of the root portion to an appropriate level was carried out. Our multidisciplinary approach achieved ideal aesthetics and improved occlusion and functional stability. Simultaneously, this method also resolved the problem of orthodontic relapse in adult patient [5-7].
This particular case falls well within the feasibility and standard aesthetics set by the “six month smile braces protocol” [1,8,9]. Even though these type of cases are frequently carried out in the western countries, it was first of its type in India and well suited for our common people, mainly because of the low risk orthodontics and lesser treatment cost for the same, thus satisfying the patient as well as the operator. Hence we can proudly claim, in this particular case, to have achieved results very similar to any other case treated by this protocol [8,9].
Conclusion
This case is a better way to display that enhanced smile aesthetics and good functional occlusion can be achieved with an interdisciplinary approach and long term stability of achieved occlusion can be maintained easily.
[1]. CC Georgaklis, Six-month adult aesthetic orthodontic treatmentDent Today 1999 18:110-13. [Google Scholar]
[2]. A Husein, T Berekally, Indirect resin-bonded fibre-reinforced composite anterior bridge: A Case ReportAust Dent J 2005 50:114-18. [Google Scholar]
[3]. JC Meiers, RB Kazemi, Chairside replacement of posterior teeth using a prefabricated fiber reinforced resin composite framework technique: A Case ReportJ Esthet Restor Dent 2005 17:335-42. [Google Scholar]
[4]. K Savana, A Ansari, PR Hamsa, M Kumar, A Jain, A Singh, Interdisciplinary therapy in orthodontics: An overviewInt J Adv Health Sci 2014 1(5):23-31. [Google Scholar]
[5]. MD Chan, An adult malocclusion requiring a combination of orthodontic and Prosthodontic treatmentAm J Orthod Dentofacial Orthop 1997 111:100-05. [Google Scholar]
[6]. WB Miller, WJ McLendon, FB Hines, Two treatment approaches for missing or peg-shapedmaxillary lateral incisors: a case study on identical twinsAm J Orthod Dentofacial Orthop 1987 92:249-56. [Google Scholar]
[7]. E Nestel, JS Walsh, Substitution of a transposed premolar for a congenitally absent lateral incisorAm J Orthod Dentofacial Orthop 1988 93:395-99. [Google Scholar]
[8]. C Georgaklis, Difficult Case Types, Part 1: A Discussion of Adult Short-Term OrthodonticsDentistry todayJune 2012. Last access date-Aug 2016. [Google Scholar]
[9]. G Hall, SmileFast - predictable short-term cosmetic orthodontics: A case reportAustralasian Dental Practice 2015 :156-63. [Google Scholar]