“Perception” is a Greek word and aesthetic is derived from it which has two dimensions, objective and subjective. The various aesthetic objectives related to orofacial complex such as unity, form, structure, balance, colour, function and display of dentition should be fulfilled by employing suitable technique [1]. Face, by which we greet the world, is the most visible part of human body and anterior teeth can be considered as natural ornaments on it. In the treatment of edentulous patients, effective relocation of anterior artificial teeth in pre-existing position is of utmost importance [2]. Prosthodontists agree upon the fact that dental prosthesis should represent approximately same amount of tissue in same position from where it is lost [3].
If the prosthesis is prepared correctly by taking consideration of some measurable parameters, it not only improves its functional stability but also improves biological and aesthetic viability [4]. The anatomical landmarks such as maxillary labial vestibule, incisive papilla, mandibular labial vestibule, retromolar pad and palatal gingival margin effectively help to achieve this purpose [5,6].
The incisive papilla is a small, pear-shaped eminence situated on the median line of the palate just behind the central incisors in dentate and in edentulous it is situated distal to or on the centre of the ridge [7]. The incisive papilla is one of the most stable landmarks remaining unchanged after tooth extraction and subsequent resorption of the maxillary ridge. Hence, it can serve as an anatomical landmark for assessing the original position of certain key teeth [8]. By determination of incisive papilla, arrangement as well as positioning of artificial teeth in accordance to it will reproduce normal function, speech and pleasing appearance [7].
If we can determine the average vertical and horizontal distance of the maxillary central incisors from the incisive papilla in our population, it will reduce the dentist’s chair side effort and patient’s time by allowing the dental laboratory technicians to reproduce the relationship established between the natural teeth and the orofacial tissues especially in the absence of pre-extraction records.
Most of the researches were carried out to measure the vertical or horizontal distance from the incisive papilla to anterior teeth. However, lot of variations are found in techniques, criteria, formula, reference points and interpretations among these researchers. Another significant factor is population being used in the study because the horizontal and vertical distances also vary within different races and ethnicity, so the result of the study on one particular population cannot be applicable to other population. The present study was carried out to measure these distances within Indian population which is very few in literature and an extra consideration was also given to the different arch forms.
Materials and Methods
An observational study was conducted in the Department of Prosthodontics in KM Shah Dental College, Vadodara, Gujarat, India, and was completed within 21 months duration (December 2013-September 2015). A total of 72 dentate subjects, 24 each of square, ovoid and tapered arch forms were considered for the comparison of the vertical and horizontal distance between mid point of incisive papilla and incisal edge of maxillary central incisors.
Dentate subjects with class 1 molar and canine relationship, ovoid, square and tapered maxillary arches were included in this study.
Patients with missing maxillary incisors, proclined maxillary incisors, supraerupted maxillary incisors, midline diastema, crowding and overlapping in maxillary central and lateral incisors, attrition of maxillary incisors, rotation of maxillary incisors, pathologic migration of maxillary incisors, mobility of maxillary incisors, previous orthodontic treatment of maxillary incisors, inflammation of incisive papilla, fractured maxillary incisors, missing incisive papilla, any pathology involving incisive papilla and maxillary incisors, and cleft lip and palate patients were excluded from the study.
Sample size was calculated as mentioned below:
Minimum 72 (24 per group) observations required to achieve mean difference of horizontal distance between arch forms by 1.09 with SD of 1.17 at 5% risk and 80% power.
N = 2*{(Z1±Z2) * SD/d}2
Where,
(Z1-2.394, Z2-0.842, SD-Standard deviation, d-Mean difference,*-Multiplication)
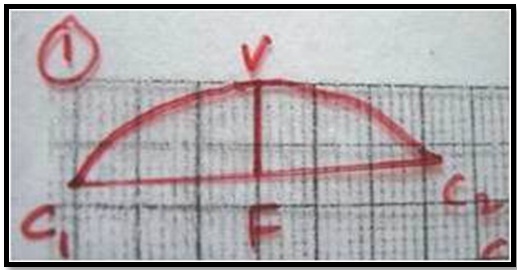
Primary impressions were made with irreversible hydrocolloid impression (Algitex, Alginate dental impression material, DPI, Mumbai, India) in dentulous stock metal trays. Impressions were poured in dental stone (Type III, Kalabhai Kalrok, Mumbai, India) and base made with dental plaster (Kalabhai Karson, Mumbai, India) in a base former. The tip of the canines and the mesial edges of the maxillary central incisors were marked [Table/Fig-1]. The three points were transferred on a graph. The mesial edges of the maxillary central incisors were labeled as “V” and the tip of the canines as C1 and C2. The points C1 and C2 were joined using a scale and a line from “V” perpendicular to C1 and C2 was labeled as “F” [Table/Fig-2]. The  formula was applied. If “R” was below 3.5 it was considered tapering, 3.5 to 4 was considered square and above 4 was considered ovoid arch form [9]. The incisive papilla was outlined and with the help of a digital Vernier’s caliper (Zoom Classic, India) the mid-point of the papilla was established and marked.
formula was applied. If “R” was below 3.5 it was considered tapering, 3.5 to 4 was considered square and above 4 was considered ovoid arch form [9]. The incisive papilla was outlined and with the help of a digital Vernier’s caliper (Zoom Classic, India) the mid-point of the papilla was established and marked.
Marking of mesial incisal edges of central incisors and canine tips on cast.

Markings transferred on graph paper in which C1 and C2 are the canine tips, V is the mesial edge of the central incisor and F is the line drawn ‘┴’ from V to C1 and C2.
Transparent templates are available in the market to classify arch forms in square, tapered and ovoid, but it cannot be used in all arch sizes. Hence, in this study a formula has been used to classify the arch forms.
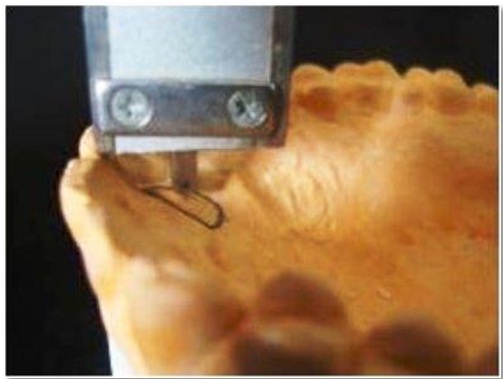
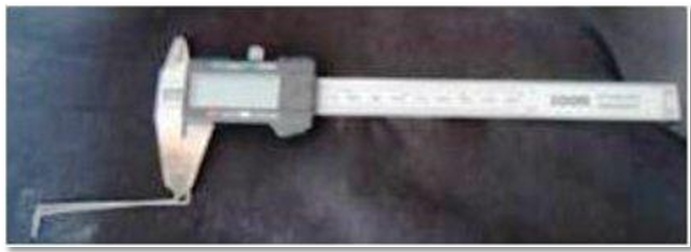
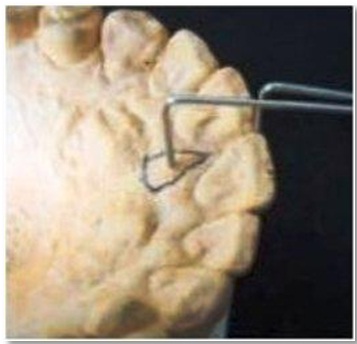
The casts were placed on the surveyor (Smydent, Masco Instruments, India), parallelism of the base of the cast to the floor was achieved. To measure the vertical distance, the digital vernier caliper (Zoom Classic, India) was mounted on the surveyor arm [Table/Fig-3]. The midpoint of the flat edge plane of the depth caliper was marked with graphite. The flat edge plane of the depth caliper contacted the mesial incisal edges of the maxillary central incisors and the midpoint of the flat edge plane of the depth caliper was matched with the mid point of the incisive papilla [Table/Fig-4]. The readings were then recorded in tabular form. To measure the horizontal distance, the digital Vernier’s caliper was modified by straightening orthodontic wire and bending it at right angle which was soldered to each arm of the digital Vernier’s caliper [Table/Fig-5]. One arm of the orthodontic wire which was soldered to the digital vernier’s caliper was placed at the mid-point of the incisive papilla and the other wire was placed on the mesial incisal edge of the maxillary central incisors [Table/Fig-6]. The readings of the horizontal and vertical distances were recorded in tabular form.
Placement of cast on the surveyor to measure the vertical distance.

Measurement of vertical distance from mid point of incisive papilla to mesial incisal edge of maxillary central incisor with the help of flat edge plane of depth caliper.
Orthodontic wire straightened and bent at right angle which is soldered to each arm of Vernier’s caliper.
One arm of the caliper is placed on the mid point of incisive papilla and the other arm at the mesial incisal edge of the central incisor.
Statistical Analysis
The distances measured in the three different arch forms were subjected to statistical analysis by using Students t-test.
Results
Mean and standard deviations of horizontal and vertical distances between mid point of incisive papilla and mesial incisal edge of maxillary incisors in ovoid, tapered and square arch forms were calculated [Table/Fig-7]. Comparison of tapered and square arch form with ovoid arch form shows significant increase in horizontal distance while no significant difference revealed between the comparison of tapered and square arch forms [Table/Fig-8].
Mean and standard deviation of vertical and horizontal distances (in mm) between mid point of incisive papilla and mesial incisal edge of maxillary central incisors in ovoid, tapered and square arch forms.
| Arch form | HorizontalMean ± S.D. | VerticalMean ± S.D. |
|---|
| Ovoid | 6.44±1.44 | 5.93±1.47 |
| Tapered | 7.74±1.57 | 5.54±1.80 |
| Square | 7.50±1.29 | 5.44±1.11 |
Statistical analysis of horizontal distance (Students t-test).
| Primary Group | Secondary Group | Mean Difference | Std. Error | t-value | p-value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Ovoid | Tapered | -1.305 | 0.435 | 2.99 | 0.004 | -2.181 | 0.429 |
| Square | Ovoid | -1.063 | 0.39 | 2.69 | 0.009 | -1.85 | -0.267 |
| Tapered | Square | 0.242 | 0.416 | 0.58 | 0.5 | -0.594 | 1.079 |
There was no significant difference in the vertical distance among the ovoid, tapered and square arch forms [Table/Fig-9].
Statistical analysis of vertical distance (Students t-test).
| Primary Group | Secondary Group | Mean Difference | Std. Error | t-value | p-value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| Ovoid | Tapered | 0.396 | 0.475 | 0.83 | 0.40 | -0.560 | 1.353 |
| Square | Ovoid | 0.490 | 0.377 | 1.29 | 0.2 | -0.268 | 1.249 |
| Tapered | Square | 0.093 | 0.432 | 0.21 | 0.83 | -0.776 | 0.964 |
Discussion
The incisive papilla is an important landmark as it is an immobile structure and usually does not shift in adult life [8,10]. The researchers have used incisor to incisive papilla distance as a biometric guide [11]. Harper RN, Martone AL and Hickey J et al., referred incisive papilla as a useful guide for the proper relocation of the anterior teeth [7,12,13]. Harper RN concluded in his study that the incisive papilla is a dependable basis for a technique designed to reproduce the horizontal and vertical position of the maxillary first incisor [7].
Many studies have been done in which researchers have measured the horizontal distance between the posterior border of incisive papilla and the mesial edges of the central incisors [2,8,14-16]. Studies have measured the horizontal distance between the mid-point of incisive papilla and the mesial edges of the central incisors [12,17-20]. Mersel A et al., have measured the horizontal as well as vertical distance between the posterior border of incisive papilla and the mesial edges of the central incisors [21]. No such study was conducted where the horizontal as well as vertical distance between the mid point of incisive papilla and the mesial edges of the central incisors have been measured in different arch forms.
The anterior part of the incisive papilla may be affected or damaged during extraction of maxillary anterior teeth, or because of the resorption that takes place following loss of teeth. The centre and posterior part of the papilla is more likely to remain constant. Therefore, the centre and posterior parts of the papilla can be used as reference points [10].
There are various instruments used to measure the horizontal and vertical distance from incisive papilla to incisal edges of maxillary central incisors. Harper RN used caliper to measure the horizontal position of the papilla and denture gauge to measure the vertical position of the papilla. But they used these instruments on pre-extraction and post extraction models of the same cases to prove that the papilla is a stable landmark [7]. Ortman HR et al., measured horizontal distances with a profile projection composed of a set of lenses with a magnifying power of 10 and the vertical dimensions was obtained from a dial gauge supported by a brass rod machined to fit into the cross-arm of a surveyor [14]. Lau GC et al., used photographic imaging and a sonic digitizer to measure the horizontal distances [22]. Zia M et al., secured cast to cast surveyor and the horizontal distance between vertical pin of the surveyor and the mesial edges of the maxillary central incisor were measured by placing protector in such a way that its 90 degree marking was almost super imposing the vertical pin of the surveyor which was touching the posterior border of the incisive papilla. After securing protector with sticky wax to the protector and the vertical pin to stop any unwanted movement, horizontal distance was measured on the calibrated transparent protector by using caliper device placed at one end which was coinciding with the vertical pin and the other end on the incisal edges [2]. Ehrlich J et al., used caliper to measure the horizontal distance, Mersel A used caliper to measure the horizontal distance and the vertical pin of the parallelometer along with caliper to measure the height (vertical) distance [8,21]. Guldag MU et al., used digital Vernier’s caliper on the surveyor to measure the vertical distance [23]. In the present study surveyor and digital Vernier’s caliper was used to measure the horizontal and vertical distance of mid point of incisive papilla and the mesial incisal edges of maxillary central incisors.
Few studies have measured the horizontal distance from the mid point of the incisive papilla to the incisal edge of the maxillary central incisors and gave a range of 5-10 mm [12,17-20]. There is a difference of 2 mm in the present study compared to the previous studies because those studies have been done on western population and arch forms were not considered. Mersel A et al., in his study gave a range of horizontal distance 7-9 mm, vertical distance 5-14 mm in ovoid arch form, horizontal distance 7-11 mm, vertical distance 6-11 mm in square arch form, horizontal distance 8-13 mm, vertical distance 6-10 mm in tapered arch form. It was done on Israeli patients and measurements were done from the posterior border of the papilla, hence a direct comparison cannot be made with the present study [21].
The results of the present study gives a range of horizontal distance 4-7 mm, vertical distance 4-6 mm in ovoid arch form, horizontal distance 6-8 mm, vertical distance 4-6 mm in square arch form, horizontal distance 5-8 mm, vertical distance 4-6 mm in tapered arch form. The distances were measured from the mid point of the incisive papilla to the mesial edges of incisal edge of the maxillary central incisors.
Limitation
This original study was limited to Angle’s class I molar and canine relationship only which is the common form of malocclusion compared to class II and class III type of malocclusion.
Conclusion
The range of horizontal distance from incisive papilla to maxillary central incisor is 4-7 mm, 6-8 mm, 5-8 mm and vertical distance is 4-6 mm in ovoid, square and tapered arch forms respectively. The clinical relevance of this study lies in application to complete denture construction and full mouth rehabilitation cases. The dentist and laboratory technician can use the results of this study as a guideline in fabrication of maxillary occlusal rims and to determine the position of the occlusal plane with the reference to other anatomical landmarks also.