PCNL has been recognized as the most critical step for access to the collecting system. Fluoroscopy, Ultrasonography (US) and Computed Tomography (CT) guidance are considered the major tools to perform PCNL [1]. Relatively better acquaintance among urologist and clear visibility [2,3] makes fluoroscopy the major tool to achieve renal access in PCNL procedures. A number of modifications like insertion of the needle pointed to an opaque stone as a guided landmark [4,5] have been put forth regarding the entrance to Pyelocalyceal System (PCS). It has been recognized that PCS has to be delineated before dilation of tract. Air, contrast or both can be used to achieve this. These agents can be gradually established in PCS by antegrade or retrograde means [6]. The proposed practice uses room air for retrograde/antegrade identification of calyceal anatomy. Use of air has certain advantages over contrast, like initial filling of posterior calyces when the patient is in prone position, preserves observation of the stone, reduces risk of extravasations [7] and contrast allergy. Keeping all these facts in view, the current investigation was aimed to compare safety, efficacy and outcome of antegrade air pyelogram for PCNL with retrograde air pyelography access using ureteric catheter.
Materials and Methods
The cross-sectional study was conducted during 2013 to 2014 at Department of Urology, SMS Medical College, Jaipur, Rajasthan, India. A clearance from Ethical Committee of Institution was obtained prior to the investigation. A written informed consent was also obtained from each patient before the study.
Sample size was calculated, based on previous similar study [8] and keeping in mind the fact that power of study should be at least 80% with 5% significance level. So, 100 patients were included with radio opaque renal calculi indicated for PCNL. Patients with congenital anomalies, uncorrectable coagulopathy, pregnancy and chronic renal failure, were excluded from the study. Patient baseline assessment included the demographic characterization, medical history, physical examination, urine analysis, urine culture and sensitivity, renal function test, coagulation test and the complete blood count.
All patients were evaluated following intravenous urography or CECT abdomen to ascertain the size and location of calculi, anatomy of upper urinary tract and the grade of hydronephrosis. Access to the PCS was defined to gain entry to the targeted urinary system and desired calyx. All patients were randomly assigned by using odd even formula in two groups namely antegrade air pyelogram group and retrograde air pyelogram group designated as Group-I and Group –II respectively. Each group contained 50 patients.
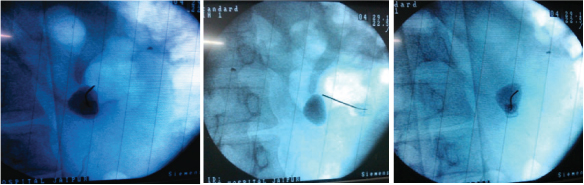
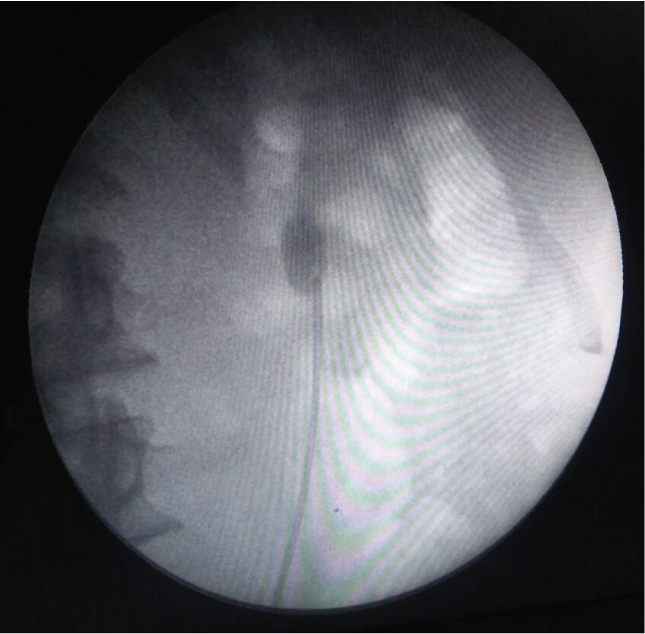
In Group-I (antegrade air pyelogram), the collecting system was delineated by targeting the renal stone using a 22 gauge spinal needle under fluoroscopic guidance while the patients were in the prone position [Table/Fig-1a-c]. A 22 gauge spinal needle was positioned at 0/30-degree by rotating C-arm enabling the urologist to aspirate urine from the collecting system hence confirming the proper positioning. Then the air pyelogram was performed using air. Following this the targeted calyx was punctured with 18 gauge diamond tip initial puncture needle and 0.038 inch J-tip PTFE guide wire put. Whereas, in Group-II (retrograde air pyelogram) urethral catheter was inserted in lithotomy position and then patient was turned from the lithotomy to prone position. Room air was injected through ureteric catheter for PCS identification [Table/Fig-2]. Targeted calyx was identified and access was attempted under fluoroscopic guidance with 18 gauge diamond tip initial puncture needle and J-tip guide wire put. Subsequent tract dilatation and stone extraction were same in both groups. Assessment of following parameters was made:
Antegrade air pyelogram: Percutaneous access utilizing air antegrade pyelogram to aid in opacifying the collecting system. a) Targeting the renal stone using spinal needle. (b) Air injected, 0 degree view (c) & 30 degree view (c).
Retrograde air pyelogram using ureteric catheter.
Duration of access was calculated from after positioning the patient and up to putting guide wire in the targeted calyx;
Duration of radiation exposure during access;
Outcome was evaluated with plain X-ray following the operation (determination of residual stone);
Relative cost-effectiveness of both procedures.
Statistical Analysis
Student’s t-test was applied to determine the significance of differences recorded during the present study. Qualitative data was expressed in percentage and proportion. Quantitative data was expressed as Mean±SD. Chi-square test at p<0.05 was applied to ascertain significance of differences in data.
Results
[Table/Fig-3] presents the baseline demographic features and other characteristics of the two groups which showed no significant difference.
Baseline characteristics of cases using antegrade and retrograde air pyelogram.
| Characteristics | Group-I(Antegrade air pyelogram) | Group-II(Retrograde air pyelogram) | p-value |
|---|
| Number of patients | 50 | 50 | |
| Gender (% male) | 70.00% (35 patients) | 76.00% (38 patients) | 0.32 |
| Age | 41.7±13 yrs | 41.4±13.6 yrs | 0.91 |
| Stone size ± SD | 2.65±0.38 cm | 2.72±0.63 cm | 0.51 |
| Duration of access±SD | 2.66±1.00 min | 19.48±5.00 min | 0.001 |
| Side of involved kidney (% right) | 44.00% (22 patients) | 48.00% (24 patients) | 0.841 |
| Duration of radiations±SD | 0.90±0.32 min. (54±18 sec.) | 0.85±0.26 min. (51±15 sec.) | 0.367 |
| Degree of hydronephrosis |
| No. of patients without hydronephrosis | 10 | 10 | 1.000 |
| No. of patients with mild hydronephrosis | 13 | 14 | 0.818 |
| No. of patients with moderate hydronephrosis | 16 | 11 | 0.258 |
| No. of patients with severe hydronephrosis | 11 | 15 | 0.362 |
| Targeted calyx |
| Superior | 7 | 6 | 0.764 |
| Middle | 16 | 14 | 0.659 |
| Inferior | 27 | 30 | 0.541 |
| Additional procedure cost | 1 USD (68 INR approx.) | 45 USD (3060 INR approx.) | 0.001 |
Note: Values represent mean±standard deviation. Statistical analysis was done using Chi-square and t-test.
Mean duration of access was 2.66±1.0 minutes after prone positioning in Group-I and 19.5±5.0 minutes in Group-II, after lithotomy followed by prone positioning of the patient (p-value 0.001).
Mean duration of access was statistically significant. Duration of radiation exposure was, nearly similar in both groups. No difference in outcome was observed between the two groups. Total of 48 (96%) patients in Group-I, whereas, in the Group-II, 49 (98%) patients were stone free after operation (p=0.351 > 0.05). On follow up imaging residual stones were found in two patients and one patient in Group-I and Group-II respectively. Mean hospital stay was 2.5 days in Group-I and 2.6 days in Group-II, respectively (p=0.193 > 0.05). Prevalence of post-PCNL fever was in 8 (16%) patients of Group-I and 10 (20%) patients of Group-II (p=0.334 > 0.05). Postoperatively blood transfusion was required in two patients in group-I and one patient in Group-II (p=0.251 > 0.05). In Group-I additional use of 22 gauge spinal needle and 10 c.c. syringe was required (coasting 1 USD/ 68 INR approximate). In Group-II cost of procedure to additional use of ureteric catheter, guide wire, painting and draping (costing 45 USD/3060 INR approximate), wearing and tearing of instruments and cystoscopy as compared to Group-I (p=0.001).
Discussion
PNCL plays an important role in management of renal calculi. Initial renal access is the important step in the PCNL and it requires a thorough understanding of renal, retroperitoneal and thoracic anatomy to minimize the risk of complications. Access to fluoroscopy and the proper equipments are necessary for complete stone removal [9]. Our study described the technique of initial renal access for PCNL used in a highvolume endourology centre, where the urologist is concern about all aspects of the procedure (time, money, safety, efficacy and outcome of the procedure).
Air can be used instead of contrast for visualization of PCS without the risk of extravasations of contrast. This preserves visualization of the stone, reduces the risk of contrast allergy and reduces difficulties in differentiation between residual stone and residual contrast [7]. Air can be injected in PCS either via antegrade or retrograde pyelography [6,8]. Present study confirms advantage in term of duration of access and cost-effectiveness between two procedures (retrograde and antegrade air pyelogram). Another potential disadvantage of retrograde air pylogram is ascending infection which can be avoided by antegrade method. In cases of minimal dilated PCS and small stone retrograde method is advantageous over antegrade method. In none or minimal dilated PCS sometimes multiple punctures may be required.
Although, there is risk of vascular injury in antegrade air pyelogram group but it is minimized using of small diameter spinal needle. No untoward event was recorded while using the air pyelogram technique during the current investigation. It has been reported that in rare cases, air embolism may take place during air pyelography [10]. However, this complication was not recorded in the present study. At high volume endourology centre, both time and cost of procedure are crucial which were significantly reduced in the current investigation in Group-I. Tabibi A et al., compared the outcomes of managing renal stones with and without retrograde pyelography using air and contrast. According to this study duration of radiation exposure, mean hospital stay, prevalence of post-PCNL fever and stone free rate were similar in both groups [8]. Similar results are obtained in our study regarding these aspects (outcome and complications). The contrasting feature of current investigation study is that air was used instead of contrast to compare the both the groups. Furthermore the current investigation also emphasizes on the duration of access and cost-effectiveness of procedure.
Limitation
Our study was also not free from limitations. In cases of none or minimally dilated PCS multiple puncture may required (although in our study only one patient in Group 1 required multiple puncture). Risk of vascular injury and air embolism may be in these kinds of procedures although we didn’t encounter such kind of complications in our study.
Conclusion
Our study ascertain that access for PCNL using antegrade air pyelogram can an acceptable alternative to retrograde air pyelogram with decreased access time and similar radiation exposure.
Conclusion
Neonatal outcome is seen to improve in groups 2A, 4A, 7A, 10A of Robson’s classification, whereas operative obstetric intervention is decreased in Group 2A but with the same neonatal outcome as intermittent foetal heart rate monitoring. CEFM will benefit patients in groups 2A, 4A, 7A and 10A of Robson’s classification in labour.
Note: Values represent mean±standard deviation. Statistical analysis was done using Chi-square and t-test.