Chronic Pulmonary Diseases (CPDs) constituted mainly by Chronic Obstructive Pulmonary Disease (COPD), Interstitial Lung Diseases (ILD) and post infective airway disease which are the major cause of morbidity and mortality worldwide. Global prevalence of COPD stands at 10.1% [1], and that of ILD varies from 13-20/100,000 [2]. With increasing lifespan and treatable communicable diseases, the global burden of chronic diseases is expected to rise, particularly in the developing countries which share 80% of the burden. Significant extrapulmonary effects contribute to the morbidity and affect the quality of life in individual patients. Spirometric analysis is used to predict outcome in CPDs; however, There is an increasing evidence suggesting that there is discrepancy between extrapulmonary effects and airflow limitation [3]. Physical activity has proven to be an important predictor of mortality in several chronic diseases [4-6]. Six minute walk test (6MWT) assesses the functional capacity of patients with cardiopulmonary diseases and provides global analysis of the respiratory, cardiac, and metabolic systems. According to the American Thoracic Society (ATS), the most precise indication for the performance of the 6MWT is mild or moderate lung or heart disease [7]; it is used in order to measure treatment response, as well as to predict morbidity and mortality.
Several studies have been done regarding the correlation of 6MWT and spirometry and the prognostic utility of 6MWT in various diseases [8-11]. However correlation between the dynamicity of 6MWT and spirometry in follow up patients and its utility has not been studied. Our study intends to assess the longitudinal change in 6MWD over time and its relation to change in spirometry findings. We also studied the predictors of mortality in CPD in Indian population. Hence, the study aimed to study the change in 6MWD over a period of one year in CPDs, to study the change in FEV1, FVC, FEV1/FVC over a period of one year in CPDs, to study the correlation of change in 6MWD with change in spirometry over a period of one year and to study the role of 6MWD in predicting mortality in CPDs.
Materials and Methods
Subjects: Patients with CPDs diagnosed on clinical and spirometric basis.
The present prospective cohort study consisted of CPD patients attending the outpatient department of a tertiary care hospital from January 2013 to June 2015, who were selected on the basis of inclusion and exclusion criteria given as follows:
| Inclusion Criteria | Exclusion Criteria |
|---|
| Age >12 years | Patients with physical limitation |
| Spirometry confirmed CPD | H/o recent myocardial infarction/acute coronary syndrome |
| Systolic BP more than 180 mmHg |
| Resting oxygen saturation <88% |
| Patients on long term oxygen therapy |
These patients were categorized into COPD, ILD and post TB sequelae as per history and spirometry. Their demographic profile was noted; 6MWT and spirometry were done as per ATS guidelines at the initiation of study [7]. These patients were treated according to their disease. COPD patients received bronchodilators and pulmonary rehabilitation which included breathing exercises, muscle strengthening exercise and vaccination, post TB sequelae patients were treated with pulmonary rehabilitation which included vaccination, postural drainage, breathing exercises and bronchodilators; whereas, ILD patients were treated with either steroids or immunosuppressants as per the type of ILD and pulmonary rehabilitation which included vaccination and breathing exercises. These patients were followed up at monthly intervals and also whenever patient visited pulmonary outpatient department for other complaints. 6MWT and spirometry were repeated after one year.
Six minute walk test: 6MWT was performed as per ATS guidelines [7]. Patients were made to sit for 20 minutes prior to the start of the test. Meanwhile vital statistics were noted and patients were explained that the aim was to walk as fast as possible for six minutes on a flat 30 meters hospital corridor. Patients were advised to stop walking if they develop chest pain, intolerable dyspnoea, severe muscle cramps, diaphoresis, staggering, pale or ashen appearance and were encouraged to restart walking as early as they could. Vital statistics were noted again at the end of the study. Distance covered in the six minutes was noted and percentage predicted was calculated using Enright PL and Sherrill DL formula and Indian reference equation [12,13].
Spirometry: Spirometry was performed as per ATS guideline [14-15]. The spirometry machine used was Medgraphics Cardiorespiratory diagnostics using Software Breeze Suite 7.1.0.32 and database version 521.
Statistical Analysis
Statistical analysis was done using STATA 13.1. Significance of change in 6MWT and spirometric values between the groups and overall CPD patients was assessed using Wilcoxon signed rank test. Mutivariate analysis was done to analyse predictors of mortality.
Results
Among 139 patients included in the study 82 (59%) were males. Age group of these patients ranged between 16 to 80 years with mean age of 51 years. There was no significant difference between the baseline characteristics of all the three groups except FVC [Table/Fig-1].
Baseline characteristics.
| Interstitial Lung Disease | Chronic ObstructivePulmonary Disease | PostTB Sequelae | Overall | p-value |
|---|
| Age (mean in years) | 43.57692 | 57.26923 | 53.3 | 51.22222 | 0.594 |
| Sex | Males | Females | Males | Females | Males | Females | Males | Females | 0.028 |
| 33 | 36 | 28 | 11 | 21 | 10 | 82 | 57 |
| Height (mean, in cms) | 153.5 | 158.6923 | 160.35 | 157.2778 | 0.654 |
| Weight (mean, in kgs) | 54.90385 | 56 | 53.45 | 54.89583 | 0.547 |
| 6MWD (mean, in meters) | 324.5188 | 286.0146 | 357.385 | 319.744 | 0.789 |
| FEV1 (mean, in litres) | 1.600769 | 1.246923 | 1.137 | 1.344167 | 0.1754 |
| FEV1% predicted (mean) | 69.88462 | 60.65385 | 56.25 | 62.76389 | 0.610 |
| FVC (mean, in litres) | 2.043846 | 1.897308 | 1.908 | 1.953194 | 0.003 |
| FVC% predicted (mean) | 66.23077 | 72.88462 | 71.75 | 70.16667 | 0.008 |
| FEV1/FVC (mean) | 79.07692 | 63.26923 | 60.7 | 68.26389 | 0.158 |
From this table it can be observed that at the initiation of study there was no significant difference in age, height, weight, 6MWD, FEV1, among three groups as determined by One-Way ANOVA. Also as determined by Kruskal-Wallis test there was no difference in FEV% predicted, FEV1/FVC among three groups. However there was significant difference in gender (Chi square test), FVC and FVC% predicted among three groups.
Out of 139 patients 72 patients completed the study, 38 patients died during the study, of which 26 patients had ILD, four had post TB sequelae and eight had COPD. Mean 6MWD for patients who died was 201.60 meters. In all the cases, death was due to progression of underlying disease. Of the total, 29 patients were considered drop outs as they didn’t turn up for the follow up test. Of the 72 patients who completed the study 26 (36%) were ILD, 26 (36%) COPD and 20 (28%) were post TB sequelae cases.
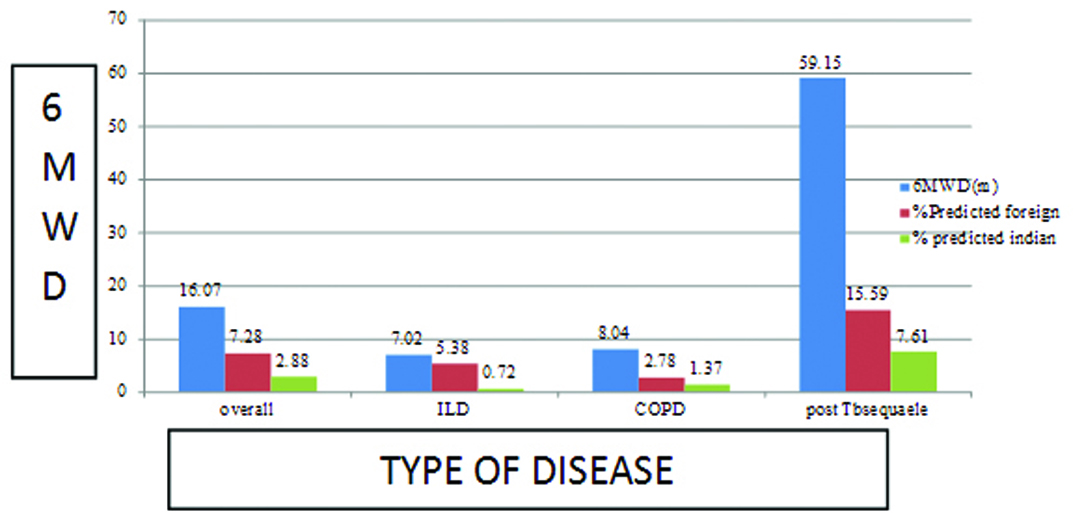
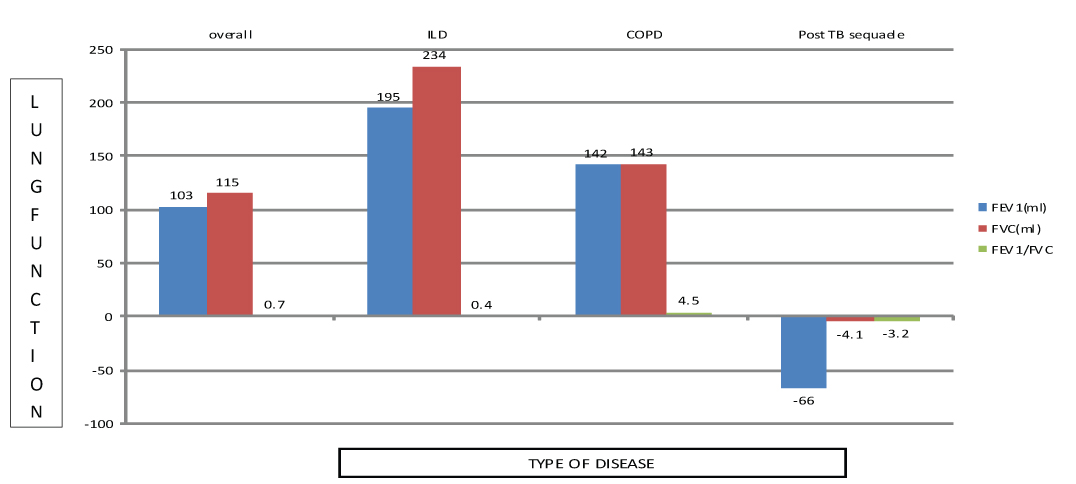
Mean decline in 6 MWD over a period of one year was 16.07 m/year and was maximum in post TB sequelae (-59.15 meters) and minimum in ILD (-7.02 meters). In COPD patients there was a decrease in 6MWD by -8.04 meters [Table/Fig-2]. Our study noted improvement in lung function in COPD (FEV1: 142 ml; FVC: 143 ml) and ILD (FEV1: 195 ml; FVC: 234 ml) patients with treatment; however, lung function declined in post TB sequelae patients with treatment [Table/Fig-3]. Though the baseline 6MWD showed significant correlation with baseline FEV1/FVC, no significant correlation was noted between 6MWD and FVC, FEV1, FEV1/FVC during follow up tests done after one year.
| Overall | ILD | COPD | Post TB sequaelae |
|---|
| 6MWD (in m) | -16.07 | -7.02 | -8.04 | -59.15 |
| Foreign Predicted (%) | -7.28 | -5.38 | -2.78 | -15.59 |
| Indian Predicted (%) | -2.88 | -0.72 | -1.37 | -7.61 |
 |
Change in lung functions.
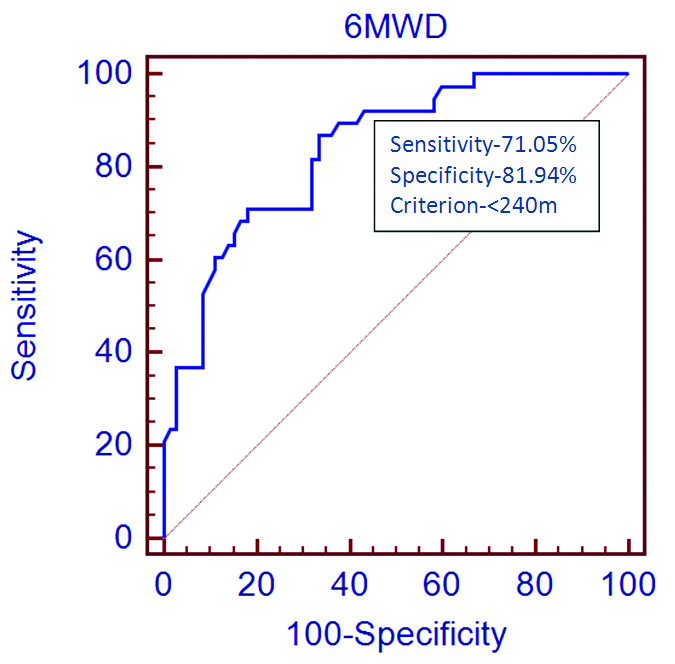
Mortality predictors were calculated by applying Mann-Whitney test and on univariate analysis FEV1/FVC, and 6MWD predicted mortality significantly among various other factors [Table/Fig-4]. Age and sex had no effect on mortality in our study. However, on doing multivariate analysis, 6MWD was the sole independent predictor of mortality irrespective of FEV1% (p<0.001), FVC% (p<0.001), FEV1/FVC (p=0.004) [Table/Fig-5]. A ROC analysis provided a cut off value of 240 meters for 6MWD, having sensitivity and specificity of 71.05% and 81.94% respectively, in predicting mortality [Table/Fig-6].
Predictors of mortality (Univariate analysis)
| Variables | 6MWD | FEV1/FVC | FEV1% | FVC% |
|---|
| Status | ALIVE | DEAD | ALIVE | DEAD | ALIVE | DECEASED | ALIVE | DEAD |
|---|
| Sample size | 72 | 38 | 72 | 38 | 72 | 38 | 72 | 38 |
| Lowest value | 136 | 48 | 33 | 43 | 23 | 18 | 27 | 23 |
| Highest value | 585 | 382.7 | 106 | 122 | 138 | 111 | 130 | 116 |
| Median | 335 | 191.625 | 69 | 76 | 60.5 | 59.9 | 70 | 62.75 |
| 95% CI for the median | 303.0000 to 361.9225 | 156.4968 to 224.5032 | 62.0000 to 76.7880 | 71.4968 to 89.0000 | 52.6360 to 68.0000 | 51.4968 to 71.5161 | 61.2120 to 76.1521 | 54.9936 to 71.0064 |
| Interquartile range | 261.3750 to 400.0000 | 150.0000 to 281.0000 | 54.0000 to 82.0000 | 68.0000 to 91.0000 | 39.5000 to 77.0000 | 47.0000 to 91.0000 | 57.0000 to 83.0000 | 52.0000 to 74.0000 |
| p-value | < 0.0001 | 0.0098 | 0.6713 | p = 0.1131 |
From this table, we can note that 6MWD, FEV1/FVC significantly predict mortality (p<0.05). Test applied was Mann-Whitney test and p-value was calculated by two tailed probability.
Predictors of mortality (Multivariate analysis).
| Standard error | 95% Confidence Interval | z-statistic | Significance level |
|---|
| 6MWD ~FEV1/FVC | 0.0659 | 0.0588 to 0.317 | 2.852 | p=0.004 |
| 6MWD ~ FVC% predicted | 0.0679 | 0.113 to 0.379 | 3.623 | p<0.001 |
| 6MWD ~ FEV1% predicted | 0.0731 | 0.170 to 0.457 | 4.29 | p<0.001 |
| FEV1/FVC ~ FEV1% predicted | 0.0564 | 0.0151 to 0.236 | 2.227 | p=0.026 |
| FEV1/FVC ~ FVC predicted | 0.0784 | 0.0956 to 0.212 | 0.741 | p=0.459 |
| FEV1%predicted ~FVC% predicted | 0.104 | -0.136 to 0.270 | 0.651 | p=0.515 |
By multivariate analysis we can note that 6MWD is a better predictor of mortality than FEV1/FVC (p=0.004), FEV1% (p<0.001), FVC% (p<0.001). Log rank test was applied to calculate p-value.
Discussion
Spirometry though is the gold standard test in assessing CPDs; it requires high cost, considerable skill and is not easily available at peripheral center. Though spirometry is often described as a simple screening test, due consideration is essential on equipment selection, test performance and interpretation of the results. Apart from chronic airflow limitation wide range of extrapulmonary effects occur in CPD like reduced physical activity, cardiovascular diseases, weight loss, depression and anaemia. These have impact on severity of disease as well as affect quality of life significantly [16-19]. With the development of CPD, an abnormal metabolic profile is associated with the muscular atrophy, which results in loss of muscle mass and muscle weakness which adversely effects exercise tolerance and overall morbidity [20]. Evaluation of exercise tolerance of these patients helps to understand the patients’ quality of life and predicts the prognosis. 6MWT is a simple tool widely used for assessing functional capacity in CPDs. It is easy to perform, reproducible, and inexpensive. It reproduces the activity of daily living and correlates well with peak oxygen uptake determined by cardiopulmonary exercise test. 6MWT is useful to assess the severity of disease, monitor the treatment efficacy and also to prognosticate mortality and morbidity in congestive heart failure, COPD [21], Idiopathic Pulmonary Fibrosis (IPF) [22] and Pulmonary Arterial Hypertension (PAH) [23]. It is essential to study the longitudinal change in 6MWD and spirometric values for comprehensive assessment of CPD.
Our study included 139 patients of which 72 patients completed the study, 38 patients died during the study and 29 patients were lost to follow up. Of the 72 patients 26 patients had ILD, 26 patients had COPD and 20 patients had post TB sequelae. There was no significant difference in baseline demographics and spirometric characteristics between the groups except for FVC and gender distribution as observed in [Table/Fig-1].
Decline in 6MWD and spirometry over a period of time is influenced by a variety of factors like age, sex, height, and weight. In our study, with demographic profiles being similar in the three groups we noted that decline in 6MWD and spirometric values was more in post TB sequelae than in COPD and ILD. Overall decline in 6MWD in CPD was 16.07 m/year, i.e., 2.88%. (8.04 m/year in obstructive group; 7.02 m/year in restrictive group and 59.15 m/year in post TB sequelae) as depicted in [Table/Fig-2]. The decline in 6MWD over a period of time is heterogenous. Decline in 6MWD over a period of three years in COPD was 62±57 meters as per study by Dajczman E et al., [24]; however, in ILD, Swigris JJ et al., observed no significant difference in 6MWD over a period of one year [10]. There are very few studies regarding 6MWD in post TB sequelae. Sivaranjini S et al., in their study observed lower average 6MWD in post TB sequelae than normal population [25]. Di Naso FC et al., noted more functional impairment in those with multidrug resistant TB [26]. Further studies are required in the field of post TB sequelae to draw any conclusion.
Change in spirometry over a period of time is also heterogeneous. It is influenced by BMI, baseline spirometric values, variability in technique, environmental exposures and insufficient number of measurements, independent of the course of the underlying lung pathology. Thus inability to show a significant physiologic decline of spirometric values in a given subject does not necessarily mean non progression of disease [27]. Casanova C et al., concluded that the progression of COPD is very heterogeneous [27]. Most patients in their study showed no statistically significant decline of FEV1. Anthonisen NR et al., observed decline of FEV1 by 39 ml/yr in COPD patients who were on treatment [28]. Collard HR et al., observed improvement of FVC in one year in ILD in 13 patients out of 51 and 23 patients had less than 10% decline in FVC, and rest had more than 10% decline [29]. Sputum positive pulmonary tuberculosis, longer duration of treatment, high radiological score before treatment and less radiological improvement after treatment are associated with more decline in lung functions in post TB sequelae [30]. Another study showed that the annual decrease in FEV1 was 35.3 ml in patients with obstructive defects within 15 years after the end of anti-tuberculosis treatment [31]. We observed improvement in spirometric values in ILD (FVC-234 ml, FEV1-195 ml) and COPD (FEV1-142 ml, FVC-143 ml) and in post Tb sequelae there was decline in spirometric values (FEV1: -66 ml, FVC: -4.1 ml) as depicted in [Table/Fig-3].
Though 6MWD correlated significantly with FEV1/FVC at the initiation of the study, change in 6MWD has no correlation with change in FEV1, FVC and FEV1/FVC. Similar findings were noted in study by Pinto-Plata VM in COPD [32]. This is most probably because several factors like co-morbidities, nutrition significantly influence 6MWT.
Morbidity and mortality in CPD depends on several variables like the disease severity, exacerbations, complications of the disease, associated co-morbidities etc. Prediction of mortality helps to categorize the patients and plan effective treatment. In our study we observed that FEV1/FVC (p=0.0098)and 6MWD (p<0.001) have significant effect on mortality as shown in [Table/Fig-4]; however, multivariate analysis revealed that 6MWD is a better predictor of mortality than FEV1, FVC and FEV1/FVC as depicted in [Table/Fig-5]. Pinto-Plata VM in his study concluded that 6MWD is an independent predictor of mortality in COPD [32]. Zanoria SJ and ZuWalllack R noticed that COPD patients with 6MWD less than 350 meters were at increased risk of respiratory related hospitalization [33]. Dajczman E et al., observed only 58% survival in those COPD patients with initial 6MWD less than 150 meters [24]. In their study, du Bois RM et al., noted that decline in 6MWD by 50 m/year is associated with four fold increase in death in one year in IPF [34]. Thus, despite its weak associations with spirometry, 6MWD aids in predicting the prognosis of CPDs. We found that at cut off value of 240 meters, sensitivity and specificity of 6MWT in predicting mortality was 71.05% and 81.94% respectively. However, majority of deceased population in our study were in ILD group, whether this applies to post TB sequelae and COPD, needs to be evaluated.
It was observed that in evaluation of CPD 6MWT has been underutilized in clinical institutes. In patients with severe respiratory disability who have difficulty in performing spirometry, or when spirometry is contraindicated, lung function test may be an insensitive tool for measuring functional status. Moreover, the 6MWT can be easily performed even in patients with advanced respiratory conditions. Though in our study, small sample size is the major limitation, our study demonstrates that for comprehensive assessment of CPDs, 6MWT is an essential tool besides spirometry. This study supports the use of 6MWT as tool in assessing mortality in CPD. Most published data in 6MWT looked at disease specific groups; however we considered heterogeneous population which included CPDs like COPD, ILD and post TB sequelae. Thus, we aimed at assessing the utility of 6MWT in patients with CPDs as a whole.
Conclusion
6MWD change is independent to change in spirometry findings and 6MWD is an independent predictor of mortality in CPDs. Also, 6MWD can be a potential tool in assessing prognosis of CPDs.
From this table it can be observed that at the initiation of study there was no significant difference in age, height, weight, 6MWD, FEV1, among three groups as determined by One-Way ANOVA. Also as determined by Kruskal-Wallis test there was no difference in FEV% predicted, FEV1/FVC among three groups. However there was significant difference in gender (Chi square test), FVC and FVC% predicted among three groups.
From this table, we can note that 6MWD, FEV1/FVC significantly predict mortality (p<0.05). Test applied was Mann-Whitney test and p-value was calculated by two tailed probability.
By multivariate analysis we can note that 6MWD is a better predictor of mortality than FEV1/FVC (p=0.004), FEV1% (p<0.001), FVC% (p<0.001). Log rank test was applied to calculate p-value.