Cytomorphology of Basaloid Squamous Cell Carcinoma: A Diagnostic Dilemma
Tanya Sharma1, Garima Goel2, Kaushik Majumdar3, Deepti Joshi4, Neelkamal Kapoor5
1 Assistant Professor, Department of Pathology, Peoples Medical College, Bhopal, Madhya Pradesh, India.
2 Assistant Professor, Department of Pathology & Lab Medicine, AIIMS, Bhopal, Madhya Pradesh, India.
3 Assistant Professor, Department of Pathology, GB Pant Hospital, Delhi, India.
4 Associate Professor, Department of Pathology & Lab Medicine, AIIMS, Bhopal, Madhya Pradesh, India.
5 Professor, Department of Pathology & Lab Medicine, AIIMS, Bhopal, Madhya Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Garima Goel, Department of Pathology & Lab Medicine, AIIMS, Saket Nagar, Bhopal, Madhya Pradesh, India.
E-mail: garima.patho@gmail.com
Basaloid Squamous Cell Carcinoma (BSCC) is an unusual and high grade variant of Squamous Cell Carcinoma (SCC) with a predilection for the upper aerodigestive tract. The cytomorphologic diagnosis of this tumour is challenging as it shares common cytomorphologic features with its differential diagnoses. However, a careful examination of the cytology can help in delivering a diagnosis of BSCC. In this case report we present the imprint cytology findings of histologically proven BSCC in a 60-year-old male who presented with an ulcerated lesion at the umbilical region.
Aerodigestive tract, Smears, Ulcerated, Umbilicus
Case Report
A 60-year-old male presented with an ulcerated lesion completely replacing the umbilicus, measuring 1.5x1.0 cm. The lesion appeared five years back as a tiny mole measuring about 0.2 cm in diameter and had been gradually increasing in size since then. For last three months, the lesion rapidly increased in size with formation of a discharging ulcer having bluish-black margins [Table/Fig-1].
Clinical picture depicting a bluish black discharging ulcerated lesion completely replacing the umbilicus.

The physical, haematological, biochemical, urine and radiological examination of the patient were within normal limits. A provisional clinical diagnosis of Basal Cell Carcinoma (BCC) was considered.
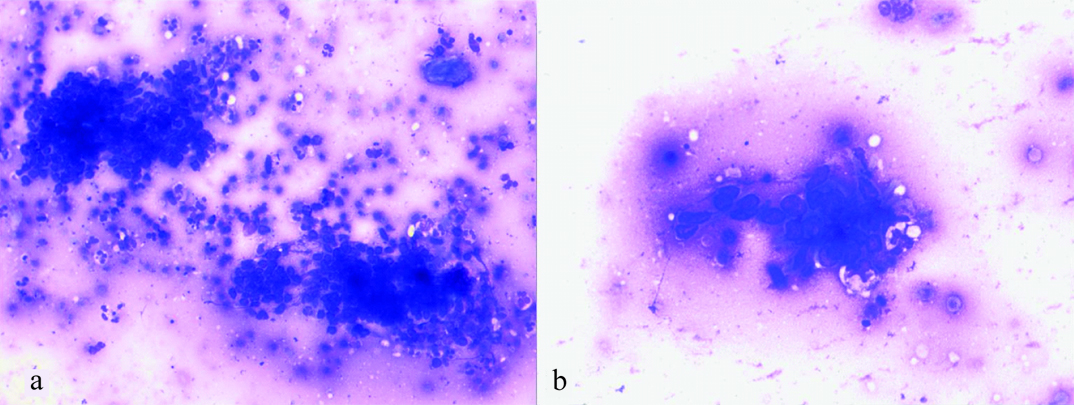
Imprint smears were prepared from the base of the discharging ulcer. Smears were air dried and stained with Giemsa stain. Cytological smears were moderately cellular. There were small overlapping clusters as well as dispersed population of small round to spindle shaped cells with hyperchromatic nuclei and scant to moderate basophilic cytoplasm [Table/Fig-2a]. Few groups of squamoid cells [Table/Fig-2b] and occasional clusters of cells with intracytoplasmic pigment deposition were also observed in the smear. A cytomorphological diagnosis of poorly differentiated carcinoma with focal squamous differentiation was considered.
a) Imprint smear showing clusters of small round to spindle shaped cells with hyperchromatic nuclei and scant cytoplasm (Wright Giemsa, 100X); b) Cells with squamoid differentiation (Wright Giemsa, 200X).
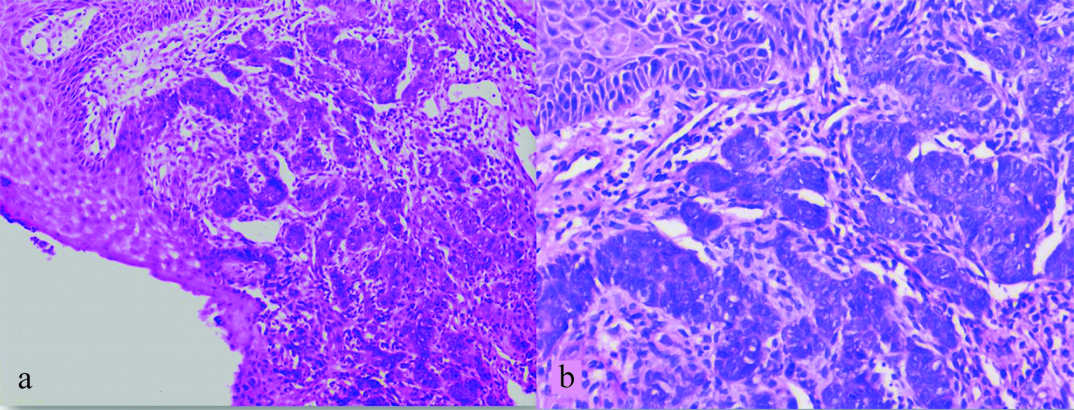
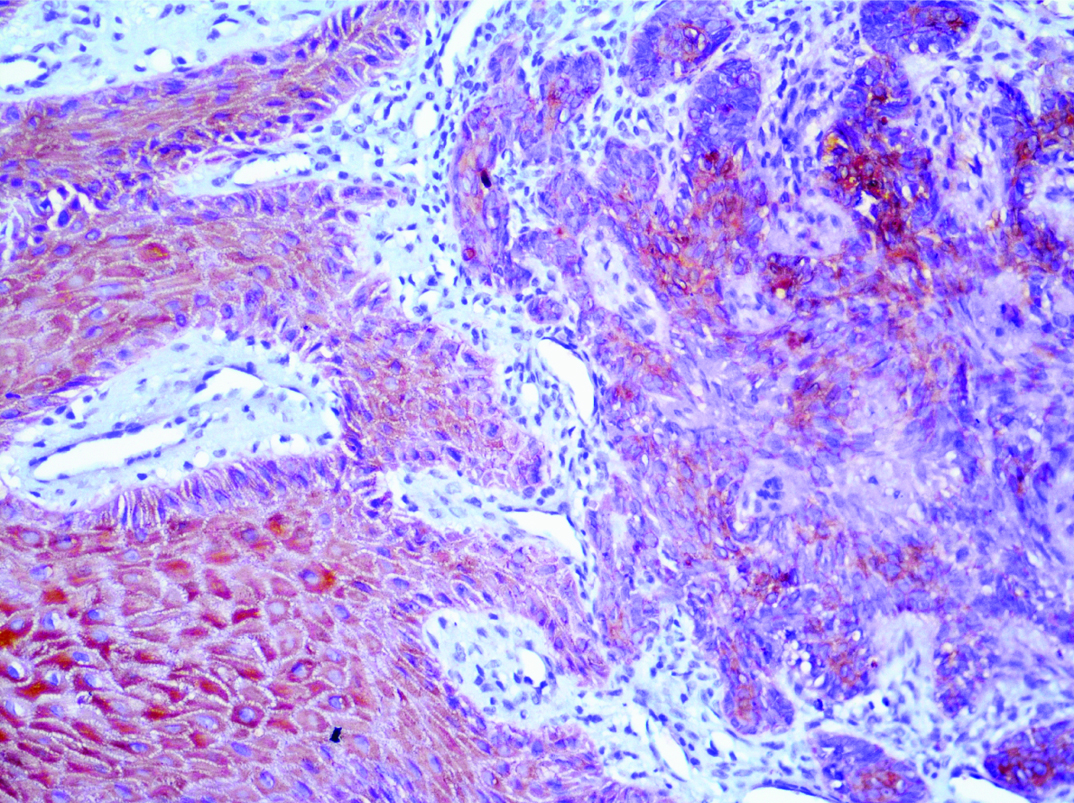
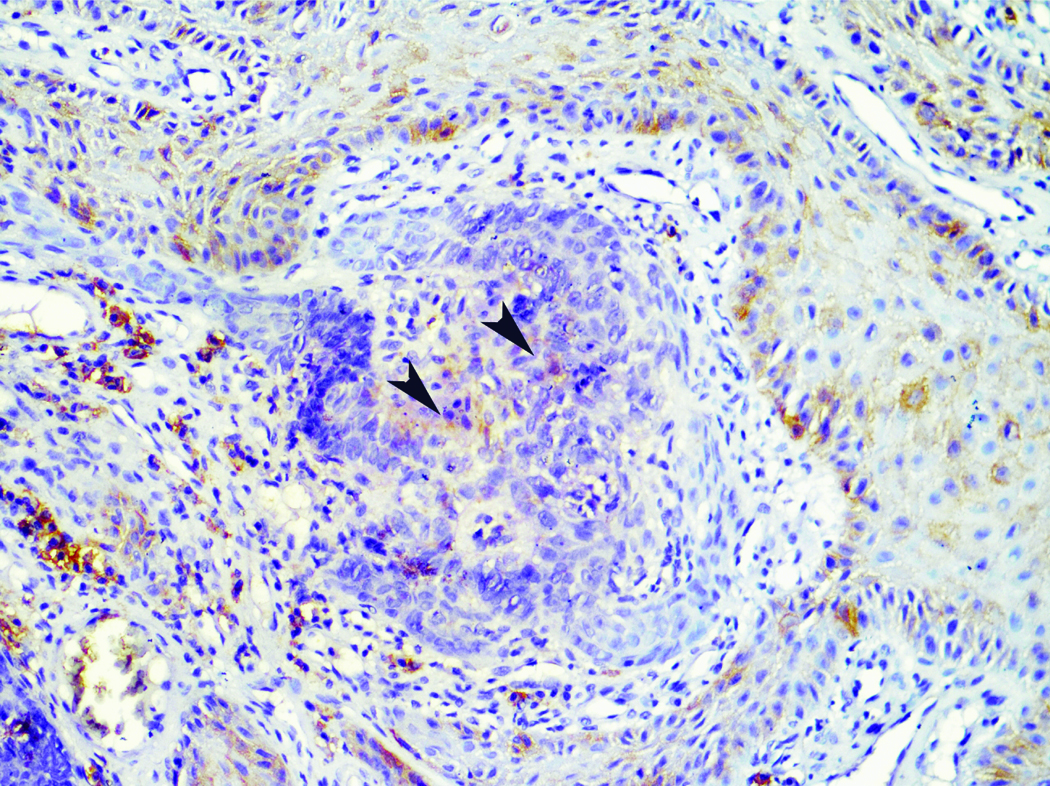
An excisional biopsy was done and histopathological examination revealed a tumour arising from the epidermis [Table/Fig-3a] comprising of islands, nests, trabeculae and cords of cells with scant cytoplasm, vesicular to hyperchromatic, round to spindle shaped nuclei and variable nucleoli [Table/Fig-3b]. Few areas showed peripheral palisading of nuclei and focal central necrosis. Few mitotic figures and apoptotic cells were also seen. On immunohistochemistry tumour cells show positive expression for CK5/6 [Table/Fig-4] and focal positivity for Epithelial Membrane Antigen (EMA) [Table/Fig-5]. A diagnosis of Basaloid Squamous Cell Carcinoma (BSCC) was made. The lesion was treated by wide local excision. The patient is on follow up without any sign of recurrence till date.
a) Section showing a tumour arising from the epidermis (H&E, 100X); b) Section showing tumour cells in nests and trabeculae with peripheral palisading (H&E, 200X).
Infiltrating tumour showing CK5/6 expression indicating squamoid differentiation (DAB, 400X).
Infiltrating tumour showing focal EMA expression (arrows); note the membranous positivity in the overlying normal squamous epithelium(right) (DAB, 400X).
Discussion
In 1986 Wain SL et al., first described the BSCC as a discrete and aggressive variant of SCC with a predilection to occur in the upper aerodigestive tract [1]. The occurrence of BSCC in the umbilical region has not been described in literature to the best of our knowledge.
In 2005 WHO defined BSCC as a high grade variant of sqamous cell carcinoma arising from the totipotential cells of the basal layer of squamous epithelium and these tumours comprise of both squamous and basaloid elements. The histological diagnosis of BSCC is uncomplicated as the histological features of BSCC have been adequately described. However, a cytological diagnosis of BSCC is problematic as only a few case reports and a rare case series have described the cytomorphology of BSCC [2-5].
In 1992, Banks ER et al., first described the cytomorphology of BSCC. They reported the cytological findings of metastatic BSCC of head and neck. The FNAC smears consisted of cohesive fragments and singly scattered small cells with scant cytoplasm, fine granular chromatin and inconspicuous nucleoli. Nuclear moulding, foci of necrosis, pseudo-glandular spaces, single keratinized cells and stromal material were also noted [6]. In addition, some authors also described the presence of metachromatic stromal material in the background [2]. In the present case we noticed clusters as well as dispersed population of small cells along with cells having squamoid differentiation.
The cytological differential diagnoses of BSCC comprises of tumours having small basaloid cells like BCC, Adenoid Cystic Carcinoma (ACC), Small Cell Undifferentiated Carcinoma (SCUC) and pilomatricoma [2,3,7]. Both BCC and BSCC show presence of clusters of small basaloid cells but in BSCC the cells show nuclei with clumped chromatin and prominent nucleoli along with mitoses and necrosis which are absent in BCC. ACC shows presence of pseudoglandular spaces and cribriform sheets of cells enclosing metachromatic hyaline stroma which may also be seen in BSCC but ACC lacks the squamous differentiation which is seen in BSCC [3]. Cytology smears of SCUC may show the presence of nuclear moulding but there is absence of squamous differentiation and hyalinized stromal fragments which are a feature of BSCC [2]. The clinical presentation of pilomatricoma is different from that of BSCC but it may be considered in the cytological differential diagnoses because of the presence of basaloid cells. The presence of ghost cells, calcification and multinucleation makes the differentiation of pilomatricoma uncomplicated [7].
The clinical diagnosis of BCC and the presence of cells with intracytoplasmic melanin pigment prompted the differential diagnosis of Pigmented Basal Cell Carcinoma (PBCC), melanoma and BSCC in the present case. The other differential diagnoses were ruled out as they do not show presence of melanin pigment. The cytological smears of PBCC show presence of cohesive sheets and syncytial clusters of small basaloid cells with peripheral palisading, which was not seen in the present case. Cytology of melanoma shows mainly dispersed cells with hyperchromatic nuclei, prominent macronucleoli and bi and multinucleation. However, due to scant cellularity on imprint smears a cytological diagnosis of poorly differentiated carcinoma with focal squamous differentiation was rendered initially but on retrospective analysis the cytological features in the present case favour a diagnosis of BSCC.
BSCC is characterized histologically by presence of irregular nests of small basaloid cells interspersed with mucin filled cystic spaces and foci of squamous differentiation. Hyalinisation of stroma, comedonecrosis and foci of keratinization may also be noted [1,2]. In the present case the histological features were characteristic of BSCC hence a final diagnosis of BSCC was given. Immunohistochemistry may aid in the diagnosis of BSCC, it shows positivity for EMA which is negative in BCC. BSCC and ACC may be distinguished with use of p63 immunostaining, which is a specific and accurate marker. BSCC shows diffuse p63 positivity, while ACC display a compartmentalized pattern within tumour nests [8]. Melanoma shows positivity for HMB-45 and Melan-A which is negative in BSCC [7].
Conclusion
To conclude BSCC an aggressive and rare variant of SCC may present in unusual sites like umbilical region as an ulcerated mass. Though the cytological diagnosis of BSCC is difficult and challenging a meticulous exploration for characteristic features like cells with squamous differentiation, keratinization and necrosis may help the cytologist in making a diagnosis of BSCC.
[1]. Wain SL, Kier R, Wollmer RT, Basaloid-squamous carcinoma of the tongue, hypopharynx, and larynx: report of 10 casesHum Pathol 1986 17:1158-66. [Google Scholar]
[2]. Joshi D, Shivkumar VB, Sharma SM, Gangane N, Cytomorphologic diagnosis of Basaloid squamous cell carcinomna: A rare case reportActa Cytol 2009 53:89-92. [Google Scholar]
[3]. Marks RA, Cramer HM, Wu HH, Fine-needle aspiration cytology of basaloid squamous cell carcinoma and small cell carcinoma: A comparison studyDiagn Cytopathol 2013 41:81-84. [Google Scholar]
[4]. Rau AR, Kini H, Naik R, Sahu KK, Case reports of basaloid squamous cell carcinoma- an aggressive variant of squamous cell carcinomaIndian J Pathol Microbiol 2005 48:31-33. [Google Scholar]
[5]. Kim MJ, Ha SY, Kim NR, Cho HY, Chung DH, Kim GY, Aspiration cytology features of pulmonary basaloid carcinomaCytopathology 2009 20:336-39. [Google Scholar]
[6]. Banks ER, Frierson HF. Jr, Mills SE, Basaloid squamous cell carcinoma of the head and neck. A clinicopathologic and immunohistochemical study of 40 casesAm J Surg Pathol 1992 16:939-46. [Google Scholar]
[7]. Jain M, Madan NK, Agarwal S, Singh S, Pigmented basal cell carcinoma: Cytological diagnosis and differential diagnosesJ Cytol 2012 29:273-75. [Google Scholar]
[8]. Emanuel P, Wang B, Wu M, Burstein DE, p63 Immunohistochemistry in the distinction of adenoid cystic carcinoma from basaloid squamous cell carcinomaModern Pathology 2005 18:645-50. [Google Scholar]