CVD has been a leading cause of morbidity and mortality in India. Recent trends indicate that CVD has escalated to younger age groups as well [1]. Global Burden of Disease (GBD, 2015) report revealed that since 1990, deaths due to CVD in India have increased by 85% [2]. At such a fast rate of increasing prevalence, there is an emergent need of prophylaxis against CVD and dynamic resistance exercises have been beneficial in this respect.
The role of Resistance Exercise (RE) for development and mainte-nance of muscular strength, endurance, power as well as muscle mass has been well accepted [3,4]. Evidences show that higher level of muscular strength is associated with a lower cardiometabolic risk [4]. Moreover, cardiac patients and the elderly are prone to develop chronic diseases that can be favourably affected by RE [5,6]. Thus, RE is strongly recommended for implementation in primary and secondary CVD prevention programs [4].
RE can be static (also known as isometric), dynamic, or both. Isometric RE is contraindicated for hypertensive individuals or those who are at risk of developing coronary artery disease. The static contraction may produce a substantial increase in intrathoracic pressure, which reduces venous return, increases the workload of the heart, and causes a significant rise in the BP. Dynamic RE comprises of concentric (muscle shortening contractions) and eccentric (muscle lengthening contractions) phase [7,8].
The contraction of skeletal muscle promotes the synthesis and secretion of cytokines and peptides from myocytes commonly termed as ‘myokines’. IL-6 is the first myokine to be released in the blood in response to exercise. IL-6 mediates both anti-inflammatory responses and metabolic adaptations, contradicting the prevailing view that IL-6 is a proinflammatory cytokine. IL-6 may reduce the incidence of cardiovascular diseases, by favourably enhancing lipid and glucose metabolism and suppressing pro-inflammatory cytokines [9,10].
The acute elevation in blood pressure during exercise is known to become accentuated with ageing. It would be dangerous to prescribe resistance exercise in the elderly with CVD risk factors, without proper medical facilities in the vicinity. A study had shown that there is no age-related difference in the cardiovascular response to either concentric or eccentric exercise [11]. Hence, the present study compares the cardiovascular response and serum IL-6 level in young healthy individuals after an acute bout of concentric and eccentric exercise involving four major muscle groups.
Materials and Methods
The present non-randomised crossover study was conducted from June 2015 to January 2016, at the Exercise Physiology Laboratory, in collaboration with Department of Biochemistry, after approval from the Ethical Committee of King George’s Medical University, Lucknow, Uttar Pradesh, India.
Sample size: Sample size (n) was calculated by the G*power software version 3.1.9.2 for Windows [12,13]. In a study, MAP after ten days of the exercise was 100±7.57 in the concentric training group and 92.60±7.604 in the eccentric training group [14]. Assuming 80% power, 5% significance level, and 50% correlation between the groups, calculated sample size was 11 if two-tailed paired t-test or Wilcoxon test is to be used. We involved 24 subjects in our study.
Inclusion criteria: Apparently healthy individuals, aged 18-25 years, having a Body Mass Index (BMI) of 18-23 kg/m2, sedentary lifestyle (inactive or moderately inactive in ‘general practice physical activity questionnaire’ [15]) and willing to participate in the study.
Exclusion criteria: History of any known disease that may adversely affect the participant’s health and/or study result. Any abnormality detected during the general and systemic examination. Residual muscle soreness or unwillingness to participate in the study after familiarisation sessions. All individuals were required to fill their response in ‘Physical Activity Readiness Questionnaire’ (PAR-Q) [16] before getting involved as a participant in the study. ‘Yes’ as an answer to any of the question in PAR-Q was one of the exclusion criteria.
Training protocol: All participants performed the Concentric Exercise (CE), as well as Eccentric Exercise (EE). A rest period of 15 days was provided between the two types of exercise.
Participants were asked to refrain from any strenuous physical activity during the study period. To eliminate the effect of circadian rhythm both exercise sessions were done between 2 pm to 4 pm. Participants were advised to wear non-restrictive, comfortable clothing for exercise.
Six familiarisation sessions, 48 hours apart, were done to ensure that the muscle soreness, anxiety and the effect on BP were minimal, whereas, specific coordination of eccentric and concentric contractions is maximal.
On test day, participants walked on ‘Pro Bodyline Fitness Treadmill 950’ at a brisk pace of 5-6 km/hr for three sessions of 10 min. A minute of rest followed each session. During CE treadmill was inclined by +.21 grade or 12° slope for ‘uphill’ or emphasised concentric walk. Similarly, for ‘downhill’ or emphasised eccentric walk, the treadmill was declined by -.21 grade or -12° slope [17].
After the treadmill, three sets of 15 repetitions were done for each: ‘Dumbbell biceps curl’ for biceps brachii muscle of the arm, ‘Standing dumbbell triceps extension’ for triceps brachii muscle of the arm, ‘Dumbbell stiff legged dead lifts’ for hamstrings muscle of the leg, and ‘Dumbbell squats’ for quadriceps muscle of the leg.
For example in ‘dumbbells bicep curls’-when the weight is curled up, the muscle fibres shorten, pulling at the elbow joint and lifting the forearm, thereby constituting concentric action. When the weight is lowered, the fibres lengthen, constituting eccentric phase. For CE-participant flexed his forearm with the dumbbells until they are at shoulder level, and then the investigator took dumbbells from participant’s hand to cut-off the resistive eccentric contraction that would have occurred in lowering the dumbbell. Dumbbells were again given to the participant once his forearm becomes fully extended. For EE-participant flexed his forearm without dumbbells, and then the investigator handed them the dumbbells to lower it. When the forearm of the participant was fully extended investigator took the dumbbell from his hand to cut-off the resistive concentric contraction that would have occurred in flexing the forearms with dumbbells in hand.
Similar procedure was done for other dumbbell exercises. Nearly 30 seconds of rest periods were allowed between each set. Dumbbells of 5-7 kg were utilised for weight lifting.
Study parameters: Parameters were recorded/measured just before and after the exercise. Omron HEM 7130’ automatic blood pressure monitor (a validated machine [18]) was used for systolic blood pressure (SBP in mm Hg), diastolic blood pressure (DBP in mm Hg) and heart rate (HR as beats/min) measurement. Pulse pressure (PP = SBP – DBP mm Hg) and mean arterial blood pressure {MAP = DBP + 1/3(SBP-DBP) mm Hg} was calculated later.
Almost 1 ml of venous blood was drawn by venipuncture under all aseptic conditions, just before and after exercise by a trained technician. Samples were kept in serum separator tube and left undisturbed at room temperature for proper clotting. Serum was separated by centrifugation at 2000 g for 15 minute. The separated serum samples were collected in the plastic vials and stored at -80°C for IL-6 level (pg/ml) estimation by RayBio Human IL-6 ELISA (enzyme-linked immunosorbent assay) kit.
Statistical Analysis
Statistical analyses were performed using the software IBM SPSS statistics version 24.0 for Windows (IBM Corp. Armonk, New York. Released 2016). The Shapiro-Wilk test and histogram with distribution curve were used to analyse the normality of data distribution. Means and standard deviations were reported in the descriptive analyses of quantitative data. Data from all the participants were pooled and segregated into two groups. One group represents the response of the participants to concentric exercise while the other group represents the response of participants to eccentric exercise. For comparative statistics, paired-samples t-test or Wilcoxon signed-rank test (for non-normally distributed data) were appropriately applied for analysing the data within-group and in-between group data. The p-value <0.05 was considered significant.
Results
Participant characteristics: All participants were male, aged 19.7±1.5 years, having a BMI of 20.2±1.8 kg/m2. No dropouts were recorded during the study.
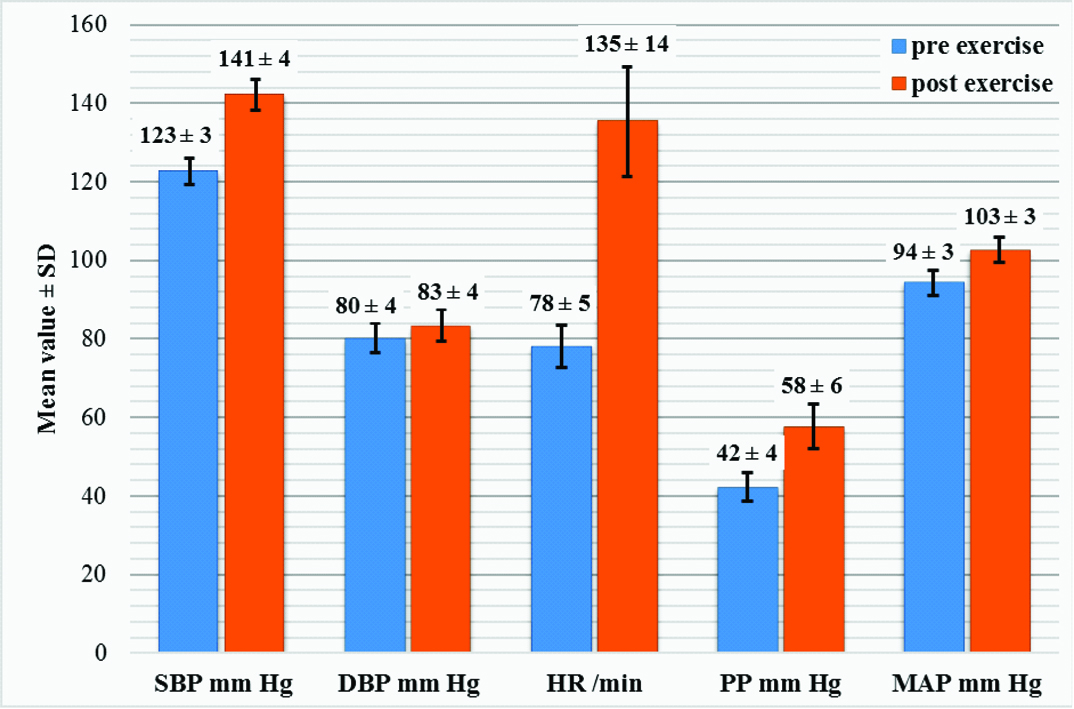
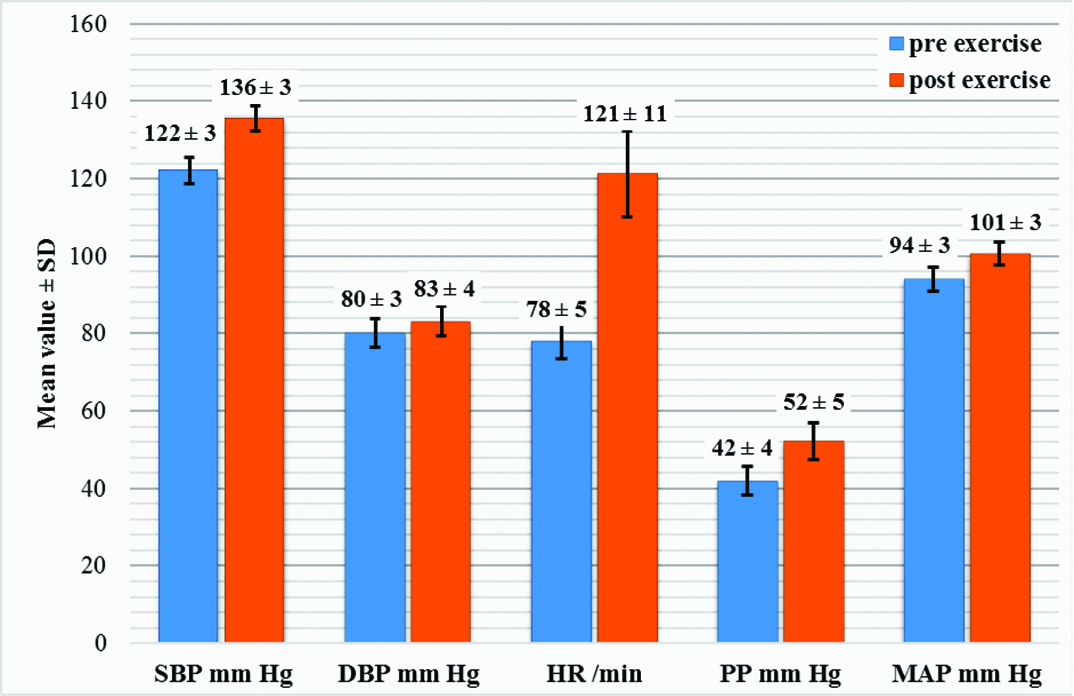
Cardiovascular response: The results of the study showed a statistically significant rise in all cardiovascular variables in response to both CE and EE. [Table/Fig-1,2] shows the cardiovascular response to CE and EE respectively. The mean absolute change (i.e., the difference between post-exercise and pre-exercise value) was significantly higher in CE than EE for all cardiovascular variables except DBP. [Table/Fig-3] represents the comparison of the mean absolute change in parameters between CE and EE.
Cardiovascular response to concentric exercise.
paired t-test, p<0.001 for all parameters, n=24
Cardiovascular response to eccentric exercise.
paired t-test, p<0.001 for all parameters, n=24
Comparison of mean absolute change in parameters between concentric exercise and eccentric exercise.
| Parametern=24 | Mean change (difference in pre-exercise topost-exercise) | p-value |
|---|
| Concentric exercise | Eccentric exercise |
|---|
| SBP (mmHg) | 18.54±3.06 | 13.38±1.72 | 0.001* |
| DBP (mmHg) | 3.25±2.79 | 3.08±1.89 | 0.446† |
| HR (/min) | 57.21±10.73 | 43.25±8.34 | 0.001* |
| PP (mmHg) | 15.25±5.29 | 10.21±3.16 | 0.001* |
| MAP (mmHg) | 8.35±1.40 | 6.50±1.0 | 0.001* |
*paired samples t-test, †Wilcoxon signed-rank test, p<.05 is significant.
Comparison of SBP, DBP, HR, MAP, and PP before CE (122.54±3.32, 80.21±3.73, 78.13±5.42, 94.32±3.15, 42.28±3.63 respectively) with SBP, DBP, HR, MAP, and PP before EE (122.17±3.35, 80.17±3.70, 78.00±4.58, 94.18±3.10, 42.08±3.75 respectively) yielded a statistically non-significant (p-value: 0.258, 0.328, 0.812, 0.244, 0.356 respectively) result on applying paired t-test.
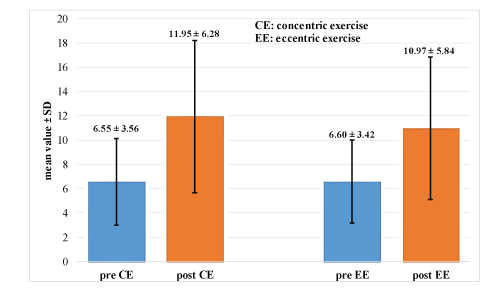
Serum IL-6 response: A statistically significant rise in the serum IL-6 level in response to both CE and EE was obtained in the present study. [Table/Fig-4] represents the comparison of IL-6 response to CE (pre-exercise value: 6.55±3.56 vs. post-exercise value: 11.95±6.28, p-value 0.001 in Wilcoxon test) and EE (pre-exercise value: 6.60±3.42 vs. post-exercise value: 10.97±5.84, p-value 0.001 in Wilcoxon test). The mean absolute change in serum IL-6 level was significantly higher in CE than EE as shown in [Table/Fig-5].
Serum Interleukin-6 level (pg/cL) before and after concentric and eccentric exercise.
Wilcoxon signed-rank test, p<0.001, n=24
The mean absolute change in serum IL-6 level in response to concentric and eccentric exercise.
| Parametern=24 | Mean change (difference in pre-exercise topost-exercise) | p-value |
|---|
| Concentric exercise | Eccentric exercise |
|---|
| IL-6 (pg/cL) | 5.40±3.13 | 4.36±2.54 | 0.009* |
*Wilcoxon signed-rank test, p<0.05 is significant
Comparison of serum IL-6 level before CE (6.55±3.56) with serum IL-6 level before EE (6.60±3.42) yielded a statistically non-significant (p-value: 0.650) result on applying Wilcoxon test.
Discussion
The present study compared the cardiovascular response and serum IL-6 level in concentric and eccentric exercise done at the same absolute workload by young individuals. Twenty-four, apparently healthy male, aged 18-24 years, having a BMI of 18-23 kg/m2 and follow a sedentary lifestyle, performed concentric and eccentric exercise bout for about 45 minutes.
Our present findings demonstrated that there was no significant difference in SBP, DBP, HR, MAP, PP and serum IL-6 level before CE and before EE. Hence, each participant acted as their own control as the baseline values before performing EE and CE were similar. SBP, DBP, HR, MAP, PP and serum IL-6 increased significantly after both CE and EE. The mean change (difference in pre-exercise to post-exercise) in SBP, HR, MAP, PP and serum IL-6 level was significantly less after EE as compared to CE. The mean change in DBP was non-significantly less after EE as compared to CE.
In our best knowledge, this is the first study in India, which was conducted to determine the cardiovascular response and serum IL-6 level during concentric and eccentric resistance exercise in young healthy individuals. Most of the previous studies have used isokinetic machines to perform the exercise on a single muscle group [19]. Therefore, it is difficult to compare our results directly with those of previous studies because of differences in exercise protocols and subject characteristics. We used a submaximal intensity exercise protocol in our study, which utilised inclined (for concentric) and declined (for eccentric) treadmill and dumbbells, involving four major muscle groups — two from upper limb and two from the lower limb.
Cardiovascular response: A series of cardiovascular adjustments occurs in response to exercise for providing adequate blood supply to the contracting muscles, to dissipate the heat generated by active muscles, and to maintain the blood supply to vital organs like brain and heart.
HR elevation during exercise is primarily controlled by sympathetic stimulation from the higher somatomotor centres of the brain. The HR response is directly proportional and linear to the intensity of exercise [20].
The increase in Stroke Volume (SV) during exercise occurs because of enhanced ventricular force of contraction. Homeometric and heterometric regulation governs myocardial force of contraction. Homeometric regulation is independent of the length of myocardial fibres at the end of diastole, and it increases the strength of ventricular contraction through increased sympathetic discharge as well as circulating catecholamines. Heterometric regulation depends on the length of myocardial fibres at the end of diastole and is mainly affected by the venous return. Venoconstriction, skeletal muscle pump, and the respiratory pump influences increase in venous return during exercise. The increase in venous return increases end-diastolic volume, which causes stretching of ventricular muscle fibres resulting in an increase in SV via the Frank-Starling mechanism. Cardiac output (Q) is defined as the product of HR and SV. As, both HR and SV increases during exercise, hence, Q also increases [20].
The increased catecholamines as well as sympathetic discharge and reduced parasympathetic activity to the heart and blood vessels results in an abrupt increase in Q at the start of exercise. Increased Q results in elevated BP. As exercise progresses, a steady state is achieved particularly in submaximal cardiorespiratory exercise, leading to the stabilisation of BP. Thus, SBP, MAP and PP rises sharply after the initiation of exercise and then get stabilised at a new level higher than the pre-exercise level. In contrast, DBP does not change substantially due to the release of local vasodilators by the exercising muscles which decrease Total Peripheral Resistance (TPR) of the vessels, a phenomenon called ‘sympatholysis’ [20].
The cardiovascular response to EE was less as compared to CE. A potential explanation for this finding may be attributable to the difference in active muscle mass utilised in these two modes of muscle contraction. At same absolute workload, recruitment and discharge rate of motor units is known to be less during eccentric contraction than during concentric contraction [21]. The results of our study are in agreement with few previous studies that have compared the cardiovascular response to eccentric and concentric exercises [22-26]. Reports from these studies indicate that the eccentric exercise causes a less cardiovascular stress. However, there were wide variations in training protocols, measurement techniques, and subject characteristics, among these studies.
IL-6 response: Initially, the increased plasma IL-6 level in response to exercise was attributed only to the muscle damage that occurs during strenuous exercise. However, later studies proved that the myocytes are responsible for the production and release of IL-6 in response to muscle contraction. Hence, muscle injury is not a necessity for incremented IL-6 level obtained after exercise [27,28]. Delayed Onset Muscle Soreness (DOMS) occurs when unaccustomed resistance exercise is performed at maximal intensity, particularly if eccentric contractions are involved. Repetition of the same exercise reduces the incidence of DOMS and is known as ‘repeated bout effect’. As few as a single familiarisation session provides sufficient protection against DOMS [29]. Hence, in the present study, exercise intensity was kept submaximal, and six familiarisation sessions were done to avoid muscle damage.
Recent evidence points at Tumour Necrosis Factor-alpha (TNF-α) as a driver in the metabolic syndrome which stimulates IL-6 production. Human skeletal muscle is unique in that during the contraction it can produce strictly TNF-independent IL-6, suggesting that muscular IL-6 has a role in metabolism rather than in inflammation [30,31].
IL-6 acts locally within the skeletal muscle (autocrine or paracrine action) and is released into the circulation to act on the peripheral organs (endocrine action). IL-6 assists in the clearance of glucose and lipoproteins from circulation and improves insulin sensitivity. The circulating levels of the anti-inflammatory cytokines IL-1 receptor antagonist (IL-1ra) and IL-10 follow the increment in IL-6, thereby having an anti-inflammatory effect. IL-6 may prevent the initiation and development of CVD as inflammation, lipoproteins and insulin resistance are integral in the formation of the fatty streak and atherosclerotic plaque [30,31].
Both CE and EE caused a significant increment in circulating IL-6. Exercise-induced IL-6 levels majorly depend on exercise intensity, duration, carbohydrate availability and muscle mass involved [32,33]. The augmented release of IL-6 has been reported from contracting muscles when intramuscular glycogen levels are low. Increased carbohydrate availability suppresses the IL-6 release.
As discharge rate and recruitment of motor units might be less for EE [21], hence work done and energy expenditure in EE could be less, as compared to CE. Heart rate after EE was significantly less, therefore it can be postulated that EE might be less intense than CE at the same absolute workload. EE induced a slightly lower IL-6 response because exercise intensity in eccentric contractions might be less than concentric contractions; moreover, due to less energy expenditure in EE, IL-6 release might have been suppressed.
The IL-6 response obtained in our study is in agreement with a most recent study that has also reported a statistically significant higher IL-6 concentration after CE than after EE [34].
Limitation
The crossover design was adopted to overcome the small sample size that might be considered as a weakness of our study. The present study was conducted on normal subjects, so the result of this study may not be generalised to patients.
Future studies should include Electromyography (EMG) data, as well as hormonal markers, which would provide a better picture of the physiology underlying the eccentric contraction. Larger sample sizes and longer duration of exercise training will also increase the accuracy of data.
Conclusion
Eccentric exercise not only caused a lesser cardiovascular demand as compared to concentric exercise but also a significant increment in IL-6 level. Exercise-induced IL-6 may prevent the initiation and development of CVD. Hence, eccentric exercise training might be recommended for reducing morbidity and mortality in elderly, frail individuals or those at risk of cardiovascular disease.
*paired samples t-test, †Wilcoxon signed-rank test, p<.05 is significant.
*Wilcoxon signed-rank test, p<0.05 is significant